
Abstract
Introduction
The COVID-19 pandemic has exacerbated psychological distress among frontline and non-frontline nurses. However, several research findings suggest that workplace social capital may have been strengthened during the COVID-19 pandemic, thereby reducing the deterioration of psychological distress.
Objective
This study investigated the perceptions of change in workplace social capital from before the COVID-19 pandemic to the time of the survey. This study also examined the influence of variables related to the COVID-19 pandemic, such as experience of discrimination related to COVID-19, on psychological distress by targeting hospital nurses.
Methods
An online survey was conducted among nurses at 138 hospitals in a prefecture in the Tohoku region of Japan from July 7 to August 8, 2022; respondents worked in their respective hospitals before and during the pandemic (N = 1,075). Generalized estimating equations (GEE) was used with psychological distress as the dependent variable, perceptions of change in workplace social capital and variables related to the COVID-19 pandemic as independent variables, and personal attributes as control variables.
Results
Four hundred and fifteen (38.6%) participants perceived a deterioration in workplace social capital before the COVID-19 pandemic, whereas 194 (18.0%) perceived improvements. Their psychological distress was influenced by marital status, experience dealing with patients suspected of having COVID-19, experience of discrimination based on COVID-19, workplace social capital at the time of the survey, and the perceptions of change in workplace social capital.
Conclusion
Some nurses perceived improvements in workplace social capital owing to the COVID-19 pandemic. Changes in workplace social capital and experiences of discrimination based on COVID-19 were factors affecting nurses’ psychological distress. To prepare for future pandemics, it is necessary to examine the deterioration of workplace social capital and discrimination against medical workers caused by COVID-19 and consider strategies to prevent the worsening of nurses’ psychological distress.
Introduction
The COVID-19 pandemic presented unprecedented challenges to global healthcare systems, significantly impacting the mental health and work environment of medical staff, especially nurses. Numerous studies have highlighted the worsening psychological distress among healthcare providers due to increased workload, exposure risks, and the emotional toll of caring for patients with COVID-19 (Chutiyami et al., 2021; Stuijfzand et al., 2020; Vizheh et al., 2020). While much research has focused on negative stressors like inadequate resources and longer working hours (Arias-Ulloa et al., 2023), surprisingly, some qualitative studies and reviews suggest that positive phenomena such as strong teamwork and increased camaraderie among frontline healthcare workers—that is, increased workplace social capital—may have helped to prevent the deterioration of psychological distress (Billings et al., 2021; Montgomery et al., 2021). This paradoxical observation underscores the importance of examining both adverse and adaptive responses within healthcare teams during crises. In this context, it is crucial to understand how workplace social capital influences psychological distress, not only for frontline nurses but also for other nursing professionals across medical institutions.
The COVID-19 pandemic profoundly affected all hospital nurses, regardless of direct contact with patients with COVID-19. Non-frontline nurses, who may not have been assigned to dedicated COVID-19 units, also reported experiencing comparable levels of psychological distress to their frontline counterparts due to the pervasive nature of the virus and evolving care demands (Tatsuno et al., 2021; Zhang et al., 2020). A key characteristic of COVID-19—the transmission by asymptomatic or presymptomatic individuals through close contact (Jefferson et al., 2022)—meant that all nurses had to provide COVID-19 equivalent care not only to symptomatic patients but also to close contacts of patients with COVID-19 (Xie et al., 2023). This pervasive and unusual experience likely exacerbated psychological distress across the entire nursing workforce.
To provide clarity, this study defines key variables as follows: Psychological distress is broadly defined as a state of emotional distress characterized by depressive symptoms (e.g., loss of interest, unhappiness, hopelessness) and anxiety symptoms (e.g., restlessness, tension; Belay et al., 2021). Workplace social capital is defined as workplace resources that concern employees’ perceptions of the trust, reciprocity, and network interactions that exist among colleagues and individuals (Tsounis et al., 2023). Non-frontline nurses are nurses who work in hospitals and are not primarily responsible for the direct care of confirmed patients with COVID-19 or assigned to dedicated COVID-19 wards, but whose roles have been affected by the pandemic-related demands (defined with reference to Tatsuno et al., 2021; Zhang et al., 2020).
Despite the widespread impact, comprehensive research specifically evaluating nurses’ retrospective perceptions of changes in workplace social capital and its direct link to psychological distress during a pandemic context remains limited. While studies have explored aspects of nurses’ mental health and workplace dynamics during the COVID-19 pandemic, a critical gap exists in understanding how perceived shifts in workplace social capital have influenced psychological outcomes. For instance, Ervasti et al. (2022) measured changes in nurses’ workplace social capital before and after the COVID-19 pandemic, but did not examine the direct impact of workplace social capital on psychological distress. This example highlights the need for research that not only assesses these changes retrospectively but also directly examines their influence on psychological distress among diverse nursing professionals.
Building upon existing knowledge, the aim of this study was to comprehensively address the research gap by evaluating the retrospective recognition of changes in workplace social capital among non-frontline and frontline nurses before and during the COVID-19 pandemic. Furthermore, this study examined the impact of these perceived changes in workplace social capital—alongside other COVID-19-related variables, such as the experience of discrimination—on psychological distress. The purpose of this research was to provide new evidence and knowledge contributing to strategies for maintaining and improving the mental health of nurses during health crises, such as in the recent pandemic and future emerging infectious disease outbreaks.
Review of Literature
Outside the context of the COVID-19 pandemic, positive outcomes of workplace social capital among nurses have been widely reported, including reduced emotional exhaustion, decreased burnout and psychological distress, increased healthy self-behavior, and enhanced job satisfaction, knowledge sharing, organizational commitment, and professional commitment (Xu & Stark, 2021). During the COVID-19 pandemic, the crisis significantly impacted workplace social capital, affecting nurses’ well-being and moral courage (Pirdelkhosh et al., 2022). However, comprehensive research specifically on workplace social capital during the COVID-19 pandemic remains limited. Few studies have examined perceptions of change in workplace social capital before and after the COVID-19 pandemic, particularly concerning its direct influence on psychological distress.
Previous research outside the context of the COVID-19 pandemic has consistently shown positive outcomes of nurses’ workplace social capital, such as reduced psychological distress (Xu & Stark, 2021). Therefore, in this study, the researchers predicted that positive changes in perceived workplace social capital as a result of the COVID-19 pandemic would be associated with reduced psychological distress among nurses. Ribeiro et al. (2022) successfully collected retrospective data on hospital nurses’ practice environment and patient safety culture at two distinct time points, “before the pandemic” and “present,” in a single survey in June 2021. Drawing on such precedents, the researchers designed a cross-sectional observational study utilizing a retrospective approach to clarify how nurses’ perception of their workplace social capital changed due to the COVID-19 pandemic and how these changes affected their psychological distress.
Since several factors influence nurses’ psychological distress, and because this study was designed during the COVID-19 pandemic, it would have been burdensome for nurses to simultaneously measure several variables given their increased workload due to the pandemic (Babamohamadi et al., 2023; Santos et al., 2024). For example, in a review of factors affecting nurses’ mental health, Yang et al. (2024) used the social ecology model to identify 114 potential predictors from the intricate interplay between intrapersonal, behavioral and lifestyle, interpersonal, organizational, political, and environmental factors. However, measuring all these variables simultaneously would further increase the burden on nurses responding to the COVID-19 pandemic.
Therefore, this study focused specifically on variables related to the COVID-19 pandemic that were predicted to cause changes in workplace social capital and affect nurses’ psychological distress. A systematic review of psychological distress among healthcare workers during the COVID-19 pandemic identified that contact with patients with COVID-19 and working on the frontline affected nurses’ psychological distress (Arias-Ulloa et al., 2023). In previous studies, data on nurses who have no history of direct contact with patients with COVID-19 and who work in non-frontline departments have been limited (Tatsuno et al., 2021; Zhang et al., 2020). Thus, experiences in dealing with patients with COVID-19 and those suspected to have COVID-19 were set as predictors of psychological distress.
Regarding discrimination related to the COVID-19 pandemic across regions, healthcare workers in Asia, Africa, North America, and Oceania experience higher levels of societal discrimination than those in Latin America and Europe (Dye et al., 2020). Furthermore, psychological distress increases as nurses who respond to COVID-19 face discrimination; this was included as a predictor in this study (Labrague et al., 2021). Moreover, regarding personal attribute factors used as control variables, a systematic review of the psychological distress of medical workers during the COVID-19 pandemic revealed that professionals who are young, women, and single have a relatively high risk of psychological distress (Arias-Ulloa et al., 2023). Therefore, age, sex, and marital status were also set as control variables in this study. The conceptual framework of this study is presented in Figure 1.
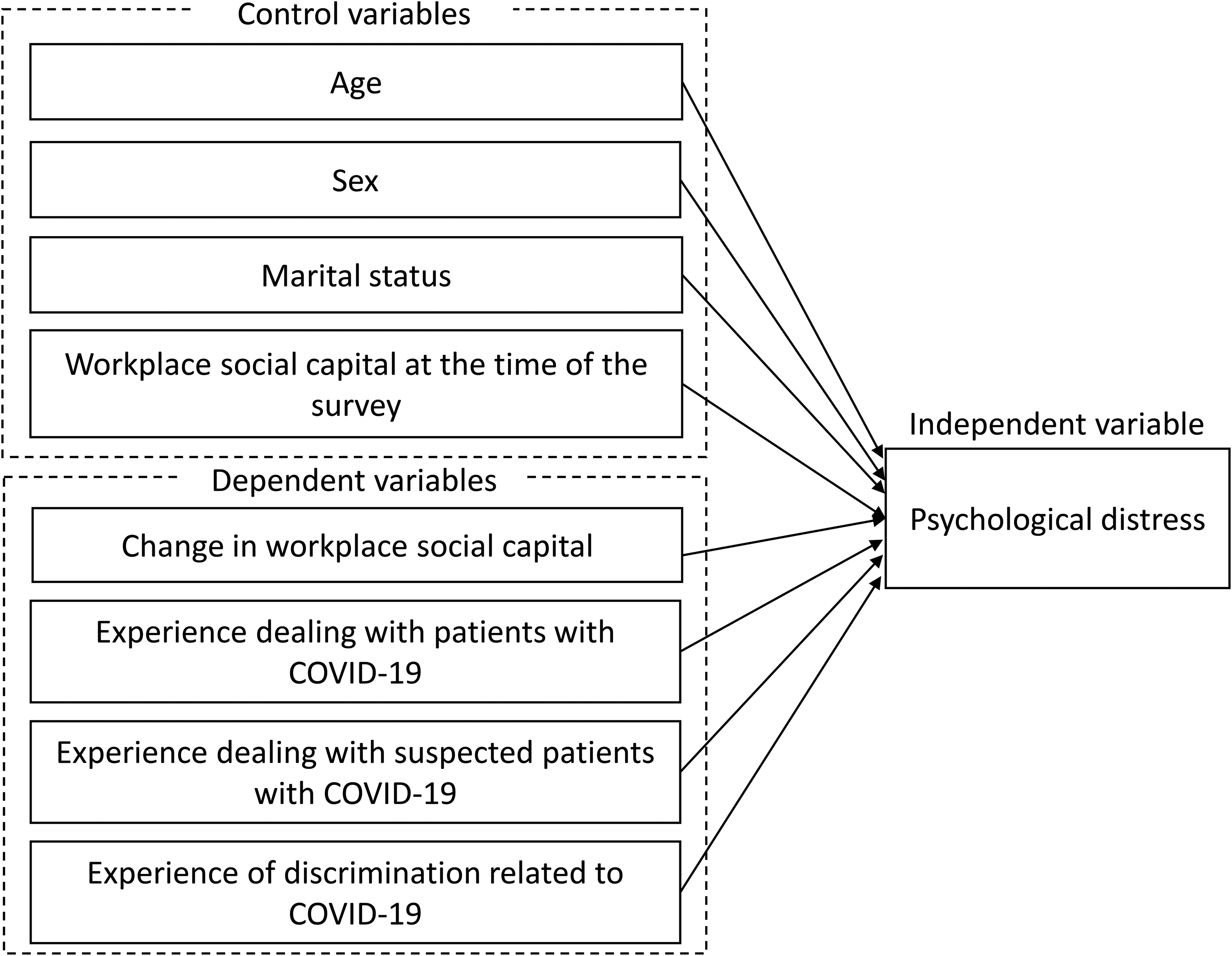
Conceptual Framework.
Methods
Research Design
This study adopted a cross-sectional observational design and complied with the STROBE checklist of items that should be included in published reports of cross-sectional studies (von Elm et al., 2008).
Setting
This study was part of a research project targeting all hospitals in one prefecture in the Tohoku region of Japan that aimed to clarify the extent of psychological distress among nurses during the COVID-19 pandemic. The research project was a panel survey spanning several years, with the survey beginning in 2020. The first panel survey was conducted in May 2020, the second in January 2021, the third in July 2022, and the fourth in November 2023. This study was based on data from the third-panel survey. In 2022, there were a total of 138 hospitals in one prefecture in the Tohoku region of Japan. Of these, 50 (36.2%) had 20–99 beds, 63 (45.7%) had 100–299, and 25 (18.1%) had 300 or more. In Japan, a medical institution with 20 or more inpatient beds was considered a hospital (Japanese Law Translation, 2018).
Data Collection Procedure
A survey request document was mailed to the nursing managers at all 138 hospitals in one prefecture in the Tohoku region. For each hospital, the researchers requested the number of nurse participants equivalent to 20% of the total number of beds in the corresponding hospital (i.e., for each participating hospital, n of nurse respondents who completed and returned the surveys = [n of total beds in that hospital ÷ 5]) for approximately 5,000 nurses. The survey request included a QR code that participants could access using their mobile phones. Nurses at each hospital read the request and then scanned the QR code with their smartphone or other device to complete the survey, which took approximately 10 min to complete. The survey was conducted from July 7, 2022, to August 8, 2022—the period corresponding to the seventh wave of the pandemic, during which the highest number of COVID-19 infections in Japan were recorded.
Measures
The questionnaire is provided in the Appendix.
Participant Characteristics
The researchers collected data on respondents’ age, number of years working as a nurse, sex, marital status, number of children, number of beds in the hospital with which they were affiliated, experience dealing with patients with COVID-19, experience dealing with patients suspected to have COVID-19, and experience of discrimination related to COVID-19.
Workplace Social Capital
The Workplace Social Capital Scale developed by Eguchi et al. (2017) was used. The scale consists of six items; the first three items focus on the aspect of bonding in the network, and items four to six focus on the aspects of trust and reciprocity. Responses were rated on a 4-point Likert scale (1 = no, 2 = somewhat different, 3 = somewhat so, and 4 = yes). The higher the score, the more social capital is cultivated in the workplace. Participants provided answers that applied to their workplace situation at the time of the survey, from July 7 to August 8, 2022, and were then presented with the same scale a second time. They were then asked to choose an answer applicable to the situation in their workplace just before the COVID-19 outbreak in Japan (January 2020).
To ensure that only those nurses who responded that they had worked at the same organization before and after the COVID-19 pandemic were included, this section included the question, “Were you working at your current workplace before the COVID-19 pandemic (before January 2020)?” Because participants answered the survey while recalling the situation at their workplace several years ago, to minimize recall bias, the statement “just before the COVID-19 pandemic in Japan” was specifically written as “January 2020.” The descriptive statistics and Cronbach's alpha are presented in Table 1. Permission to use the tool for research purposes was obtained from the researchers who developed the scale.
Descriptive Statistics of the Scales and Cronbach's α Coefficient.

SD: standard deviation.
Psychological Distress
To measure psychological distress, the researchers used the Japanese version of the Psychological Distress Scale. The original scale was developed by Kessler et al. (2002); Furukawa et al. (2008) verified the reliability and validity of the Japanese version. The latter consists of six items, with responses rated on a 5-point Likert scale (5 = always, 4 = most of the time, 3 = sometimes, 2 = a little bit, 1 = not at all). Higher scores indicate greater psychological distress. This scale was widely used in Japan, including by local governments, hence, no permission was required for its use.
Statistical Analysis
First, descriptive statistics were calculated for the participants’ basic attributes and each scale. Further, the reliability coefficients for each scale were calculated.
Specifically, the researchers calculated the difference in workplace social capital both before the COVID-19 pandemic and at the time of the survey to capture the degree of perceived change. Positive changes indicated that nurses perceived improvement in their workplace social capital, while negative changes indicated that it worsened. The distribution of the degree of perceived change was plotted. Next, the researchers conducted a paired t-test to examine whether the average value of workplace social capital changed between the two periods. Subsequently, the researchers calculated Pearson's product–moment correlation coefficients for age, workplace social capital, and psychological distress. Up to this point, statistical analyses were performed using SPSS ver. 26.0 for Windows (IBM Corporation); all tests were two-tailed, and the significance level was 5%.
Finally, the researchers performed a multivariate analysis using GEE. The dependent variable was psychological distress, and the independent variables included age, sex, marital status, experience dealing with patients with COVID-19, experience dealing with patients with suspected COVID-19, experience of discrimination related to COVID-19, workplace social capital at the time of the survey, and perception of changes in workplace social capital. The GEE approach, an extension of the generalized linear model, was suitable for analyses with correlation structures such as repeated measurements in longitudinal studies and clustered data (Hara et al., 2020). The retrospective questionnaire survey used in this study, along with longitudinal data measured at two points, was expected to exhibit intra-individual correlations and a large variation in the amount of change among individuals. Thus, GEE was used to input the difference between the two data points (value at the time of the survey - value before the COVID-19 pandemic) into a multiple regression model. Continuous variables were converted to z-scores before being entered to evaluate the estimates as standard partial regression coefficients (Lewis-Beck et al., 2003). Statistical processing of GEE was performed using the GENMOD procedure in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at p < .05 (two-sided).
Sample Size
Sample size calculation was performed based on the overall project design. Regarding the sample size of the GEE used in this study, the results of a simulation study showed that the larger the sample size, the smaller the estimation bias and the better the performance (Wang, 2014). Although this depends on the research method, it has been acknowledged that a sample size of 500 or more is desirable (Spiess et al., 2020). The number of participants in this study was 1,075; therefore, it was judged to have sufficient detection power, and GEE was performed (Spiess et al., 2020).
Ethical Considerations
This study was conducted in accordance with the ethical guidelines for medical and health research involving human participants in Japan and the 1995 Helsinki Declaration (revised in Edinburgh, 2000) and approved by the Clinical Research Ethics Committee of Tohoku University Hospital (no. 20110) on September 24, 2020. The purpose and content of the study were explained in writing to the nursing directors at each facility. Before the online survey, individual nurses were informed of the purpose of the study and terms related to voluntary participation and confidentiality via a PDF document. The responses to the web survey were interpreted as consent to participate. All surveys were conducted anonymously.
Results
Descriptive Statistics of Participant Characteristics and Items Related to COVID-19
Of the 1,505 nurses who completed the survey, our analysis included only those (N = 1,084) who met the following inclusion criteria: those who had been working in their present workplace both before and throughout the COVID-19 pandemic period as of the time of the survey; the remaining 421 respondents were excluded. The researchers also excluded nine respondents who had missing answers on the face sheet, resulting in the inclusion of 1,075 nurses (71.43% of total respondents).
Descriptive statistics for participants’ characteristics, experience dealing with patients with COVID-19, and experience of discrimination related to COVID-19 are presented in Table 2. The mean age of the participants is 41.4 years (SD = 10.7), and the majority of the nurses are women (n = 1,002; 93.2%). The average number of years of experience as a nurse is 18.6 years (SD = 10.4). Of the 1,075 participants, 525 (48.8%) have experience dealing with patients with COVID-19, and 863 (80.3%) have experience dealing with patients with suspected COVID-19. Conversely, 343 participants (31.9%) experience discrimination related to COVID-19.
Participants’ Basic Attributes (N = 1,075).

SD: standard deviation.
Perceptions of Changes in Workplace Social Capital Before the COVID-19 Pandemic and During the Survey
The mean and standard deviation of the participants’ workplace social capital before the COVID-19 pandemic and during the study period were 17.5 (SD = 3.5) and 16.7 (SD = 3.7), respectively. A paired t-test result was t (1,074) = 9.64, p < .001, 95% CI [0.61, 0.93]. The effect size r was 0.28. Therefore, the average workplace social capital at the time of the survey was lower, indicating deterioration.
Next, the researchers subtracted the COVID-19 pandemic value of workplace social capital from the value at the time of the survey and plotted the perceptions of change (Figure 2). A zero-change implied that no change was perceived (466 participants, 43.3%). Overall, 194 nurses (18.0%) perceived a positive change, and 415 nurses (38.6%) perceived a negative change.
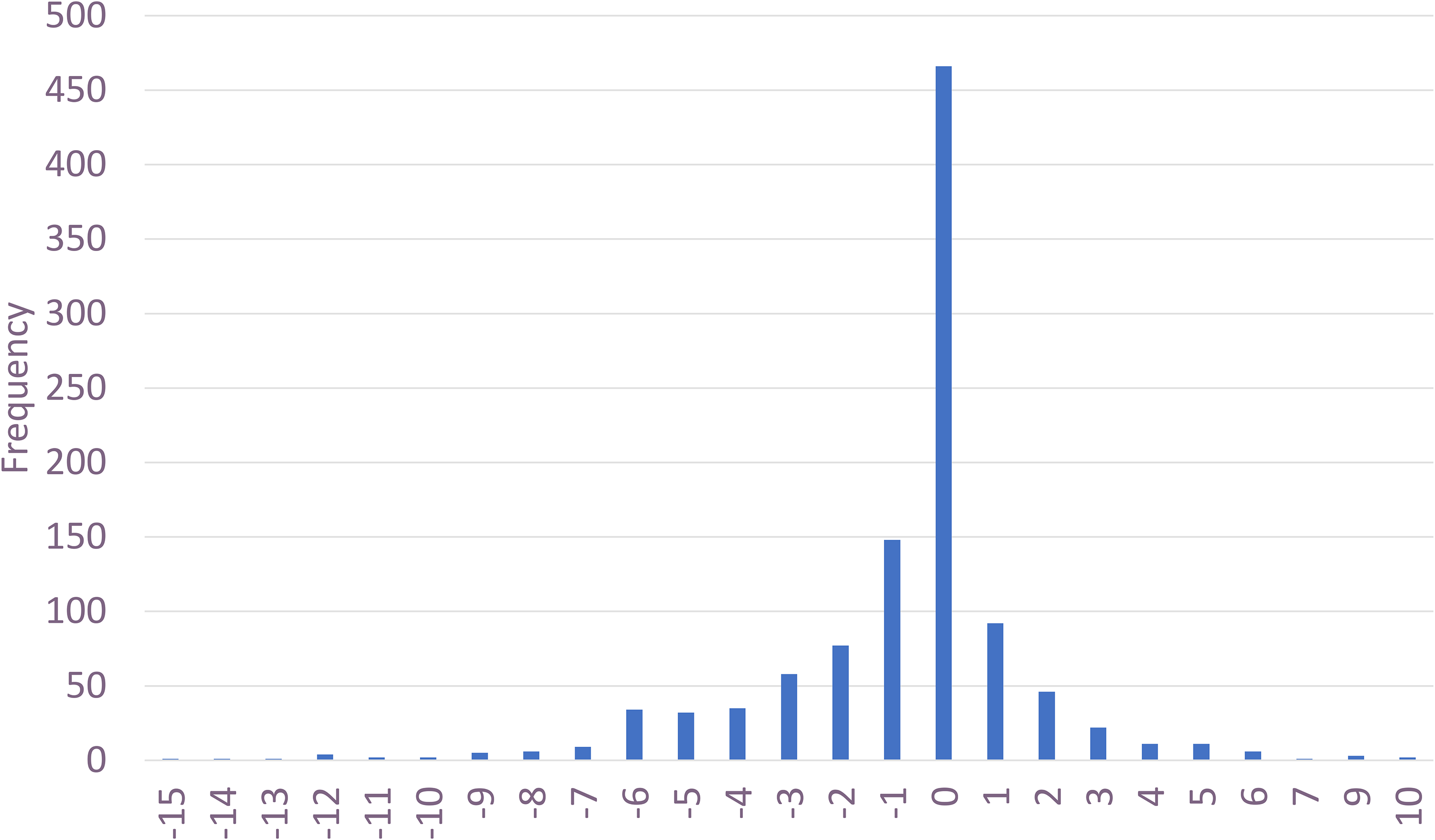
Difference Between Total Workplace Social Capital Scores Before the COVID-19 Outbreak and During the Survey Period.
Correlation Coefficient and GEE With Psychological Distress as the Dependent Variable
Table 3 presents the results of calculations of Pearson product–moment correlation coefficients for age, workplace social capital, and psychological distress.
Correlation Coefficients Between Age, Workplace Social Capital, and Psychological Distress.

Pearson's product-moment correlation coefficients. *p < .05, ** p < .01, *** p < .001.
GEE results revealed that marital status (β = −0.142, p < .05), experience in dealing with patients with suspected COVID-19 (β = 0.186, p < .05), experience of discrimination related to COVID-19 (β = 0.481, p < .001), workplace social capital at the time of the survey (β = −0.211, p < .001), and the perceptions of change in workplace social capital (β = −0.091, p < .01) had a significant effect on psychological distress (Table 4).
Generalized Estimating Equations Predicting Psychological Distress.

*p < .05, ** p < .01, *** p < .001.
†Standardized regression coefficients.
Discussion
To our knowledge, this study was the first to examine the effects of the perceptions of change in workplace social capital before the COVID-19 pandemic and during the survey, as well as variables related to the COVID-19 pandemic, on psychological distress among frontline and non-frontline nurses working in hospitals.
The results of this study showed that, although the degree of change in workplace social capital was less likely to improve than to worsen, 18% of respondents recognized that the COVID-19 pandemic had improved their workplace social capital. Considering the heavy burden the pandemic placed on nurses’ management, including the organization of dedicated wards and medical staff vacancies (Udod et al., 2024), the finding that many nurses perceived their workplace social capital to have worsened is understandable.
However, narratives from frontline managers during the COVID-19 pandemic show that they engage in compassionate actions and build a culture of care for themselves and their staff (Udod et al., 2024). Thus, owing to these efforts, some workplaces maintained and improved workplace social capital, even during the COVID-19 pandemic, which is an important finding in preparing for future pandemics of unknown emerging infectious diseases.
Furthermore, the results showed that not only the workplace social capital at the time of the survey but also the perceptions of change in workplace social capital from before the COVID-19 pandemic influenced nurses’ psychological distress. This result aligns with findings from previous research (Xu & Stark, 2021) that nurses’ workplace social capital affects psychological distress outside the context of the COVID-19 pandemic. Additionally, this study quantitatively verified the results of qualitative studies showing that COVID-19 strengthened team cohesion among staff and reduced psychological distress, adding to existing literature (Billings et al., 2021; Montgomery et al., 2021). As described in the results of a review of qualitative studies targeting frontline healthcare workers, the unfair distribution of work due to the COVID-19 pandemic and the refusal of some colleagues to treat patients infected with the virus (Billings et al., 2021) may have similarly deteriorated workplace social capital in departments that are not on the front lines of the COVID-19 pandemic, leading to increased psychological distress for individual nurses. This study focused only on the perceptions of change in workplace social capital and factors related to the COVID-19 pandemic. In the future, it will be necessary to clarify the factors and mechanisms that affect nurses’ psychological distress by using various predictors, including variables that were not measured in this study, such as the emergency level of the medical institution the nurses are affiliated with and the increased workload due to the COVID-19 pandemic.
Additionally, when variables related to experiences of dealing with patients with COVID-19 and patients with suspected COVID-19 were examined simultaneously, the latter experience, that is, dealing with patients with suspected COVID-19, had a greater impact on psychological distress. The results of this study support the finding that non-frontline nurses also experienced psychological distress to the same extent as frontline nurses (Tatsuno et al., 2021; Zhang et al., 2020), emphasizing the need to also focus on psychological distress for non-frontline nurses.
Many countries have created manuals for the isolation of patients with suspected and confirmed COVID-19 (Xie et al., 2023); therefore, nurses responded by following these manuals. However, a characteristic of COVID-19 is that asymptomatic or presymptomatic individuals can transmit the virus through close contact (Jefferson et al., 2022), and many frontline and non-frontline medical workers fear being infected (Zhang et al., 2020). A review of factors affecting nurses’ mental health identified protective factors as feeling evaluated/rewarded, inclusive/fair leadership, and work controllability (Yang et al., 2024). The COVID-19 pandemic has placed a heavy burden on healthcare workers worldwide, but setting appropriate rewards, leaders demonstrating inclusive and fair leadership, and increasing the work controllability of individual nurses may alleviate the psychological distress of nurses.
Furthermore, the results of this study support previous research that experiences of discrimination due to COVID-19 constitute a factor that influences psychological distress (Labrague et al., 2021). Among the participants in this study, 31.9% reported experiencing discrimination, which was higher than the 18.1% reported by Dye et al. (2020) of healthcare workers around the world, including Asia, who reported experiencing discrimination. This result suggests that discrimination against healthcare workers related to the COVID-19 pandemic may have been observed more frequently in Japan; notably, among the variables used in this study, discrimination experiences due to COVID-19 had a strong influence on the psychological distress of nurses. As Shimizu and Lin (2022) point out, possibly, non-scientific media reports have disseminated misinformation to the public, and strong peer pressure among Japanese people has increased discrimination against healthcare workers. To prepare for future pandemics of unknown emerging infectious diseases, it is necessary to consider effective communication strategies to address discrimination against healthcare workers working on the front lines.
Strengths and Limitations
This study has certain strengths. It was the first to focus on the perceptions of change in workplace social capital prior to the COVID-19 pandemic and throughout the study period. Additionally, the inclusion of non-frontline nurses, alongside frontline nurses working in hospitals settings, enhanced the comprehensiveness of the findings.
In this study, the researchers employed a cross-sectional research design to measure the perceptions of change in workplace social capital; hence, several measurement biases were expected. For example, the study participants answered the survey by recalling the workplace situation several years ago, which may have resulted in recall bias. Additionally, only nurses who answered that they worked in the same organization before and after the COVID-19 pandemic were included in the analysis, but the organization and team members may have been different before and after the COVID-19 pandemic due to resignation or transfer, and the participants themselves may have belonged to a different team. Therefore, they may have evaluated different environments and organizations before and after the COVID-19 pandemic.
Further, nurses who perceived low workplace social capital or high psychological distress may have already left their jobs at the time of the survey. Therefore, nurses who did not leave their jobs even during the COVID-19 pandemic participated in this study, which may have resulted in survivor bias. These factors may affect the design and results of this study; thus, caution is required in interpreting the results. In the future, it may be valuable to conduct a long-term longitudinal study of hospital nurses to avoid these measurement biases and explore various changes even during the outbreak of an unexpected global pandemic.
Additionally, the participants in this study were limited to nurses working in Japanese hospitals. Workplace social capital and its influencing factors may differ between countries and other cultural areas. Therefore, caution should be exercised when applying the results of this study to other cultures. In the future, it will be necessary to conduct similar research in various countries and cultural areas.
Finally, this study was conducted during the COVID-19 pandemic, and to minimize the burden on nurses working in hospitals while participating in the survey, only a limited number of predictors influencing nurses’ psychological distress were measured. A range of factors affecting nurses’ psychological distress, and unknown influencing factors due to the COVID-19 pandemic, such as the emergency level of the facility with which the nurses are affiliated, are suspected; hence, further research is needed.
Implications for Practice
In the event of future irregular circumstances, such as outbreaks of previously unknown infectious diseases, frontline managers may be able to maintain and improve workplace social capital by implementing compassionate interventions and fostering a culture of care for both themselves and their staff. The COVID-19 pandemic has imposed a significant burden not only on frontline nurses but also on non-frontline nursing staff. However, the establishment of appropriate compensation structures, the presence of leaders who exhibit inclusive and equitable leadership, and increasing the controllability of individual nurses’ work may contribute to mitigating nurses’ psychological distress.
Conclusions
This study targeted frontline and non-frontline nurses working in hospitals in Japan and analyzed the impact of the perceptions of change in workplace social capital before the COVID-19 pandemic and during the survey, as well as variables related to the COVID-19 pandemic, on psychological distress. Results showed that while many nurses recognized a deterioration in workplace social capital, some nurses recognized that the COVID-19 pandemic had improved workplace social capital. Nurses’ psychological distress was also influenced by marital status, experience of dealing with patients with suspected COVID-19, experience of discrimination based on COVID-19, workplace social capital at the time of the survey, and the perceptions of change in workplace social capital. The COVID-19 pandemic has placed a heavy burden on medical teams worldwide. To prepare for future unknown emerging infectious diseases, it is necessary to further examine the deterioration of workplace social capital and discrimination against medical workers that occurred during the COVID-19 pandemic and consider strategies to prevent the deterioration of nurses’ psychological distress.
Supplemental Material
sj-docx-1-son-10.1177_23779608251381180 - Supplemental material for Impact of Workplace Social Capital and COVID-19 on the Psychological Distress of Hospital Nurses: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251381180 for Impact of Workplace Social Capital and COVID-19 on the Psychological Distress of Hospital Nurses: A Cross-Sectional Study by Yukari Hara, Shoko Sugiyama, Nozomu Takada, Yoko Nihei, Masako Yamada and Kyoko Asakura in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251381180 - Supplemental material for Impact of Workplace Social Capital and COVID-19 on the Psychological Distress of Hospital Nurses: A Cross-Sectional Study
Supplemental material, sj-docx-2-son-10.1177_23779608251381180 for Impact of Workplace Social Capital and COVID-19 on the Psychological Distress of Hospital Nurses: A Cross-Sectional Study by Yukari Hara, Shoko Sugiyama, Nozomu Takada, Yoko Nihei, Masako Yamada and Kyoko Asakura in SAGE Open Nursing
Footnotes
Acknowledgments
Authors’ Contributions
Yukari Hara contributed to all phases of the study, including the study design, literature review, study procedures, data analysis, and writing of the different versions of the manuscript. Kyoko Asakura, Shoko Sugiyama, Nozomu Takada, Yoko Nihei, and Masako Yamada assisted with the study design and data interpretation as well as with critically reviewing different versions of the study. All the authors have read and approved the final version of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the JSPS KAKENHI (grant number 21H03216).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.