
Abstract
Introduction
Subjective cognitive decline (SCD) is a self-perceived decline in cognition that may progress to mild cognitive impairment or Alzheimer's disease. SCD may be associated with difficulties in daily functioning and psychological distress. Previous research has shown the association between functional difficulties and SCD via mentally unhealthy days (MUDs). However, whether income levels influence the mediation effect of MUDs is less understood.
Objectives
This study examined the association between subjective functional difficulties and the odds of SCD through MUDs, and whether the mediation effect was moderated by income levels.
Methods
Cross-sectional data were obtained from the 2019 Behavioral Risk Factor Surveillance System (N = 13,160 older adults aged 65+; 7,370 women). SCD was assessed by more frequent or worse memory loss and confusion in the past 12 months. Subjective functional difficulties represented difficulties with daily activities. MUDs denoted the days that a person felt mentally unwell within the past 30 days. We used path analysis with 5,000 bootstrapped confidence intervals and logistic regression to classify the risks of SCD based on subjective functional difficulties and MUDs.
Results
Subjective functional difficulties were positively associated with SCD through mediation by MUDs (b = 0.119, 95% CI 0.102, 0.137). After accounting for covariates, we found that greater subjective functional difficulties were associated with 2.50 times the odds of SCD (AOR = 2.50; 95% CI: 2.14, 2.91); MUDs were related to 1.06 times the odds of SCD reporting (AOR = 1.06; 95% CI: 1.05, 1.07). Income levels moderated the indirect effect of MUDs in the subjective functional difficulties-SCD relationship, with an income of <$15,000 showing the most prominent effect. Those earning ≥$50,000 self-reported a lower SCD than those earning <$15,000.
Conclusions
Our study extends previous findings by demonstrating that greater subjective functional difficulties are associated with higher odds of SCD through more frequent MUDs, with higher income levels being associated with more SCD reporting.
Keywords
Introduction
Older people may experience difficulties with activities of daily living (ADLs), also reporting a cognitive decline. Subjective cognitive decline (SCD) is a self-perceived decline in cognition, which may lead to a more severe cognitive impairment such as dementia or Alzheimer's disease (Jessen et al., 2020). Perceiving a decline in one's ability to function may cause mental distress due to frustration with daily tasks (Roehr et al., 2019; Stogmann et al., 2016). Older adults may show higher negative reactivity as a psychological response toward frequent functional daily stressors, leading to mental distress (Charles et al., 2013; Sin et al., 2015). Despite increased studies reporting the association between functional difficulties and SCD (Roehr et al., 2019; Stogmann et al., 2016), subjective functional difficulties (SFDs) is underexplored in the presence of psychological distress. For example, a scoping review examining the functional performance indicators of SCD revealed that of the 2,032 titles and abstracts being reviewed, only eight studies considered psychological comorbidities influencing the experience of SCD (Komalasari et al., 2022). While increasing evidence showed that psychological distress is a confounder of SCD (Caselli et al., 2014; Edwards et al., 2016), fewer studies have examined how psychological distress, as a response to daily functional challenges, is associated with SCD at differing income levels.
Review of Literature
Increased functional difficulties may harm life domains in aging populations if inadequately intervened. Without targeted interventions, challenges in performing basic ADLs, such as eating and toileting (Hall et al., 2011), and more complex ADLs (or instrumental ADLs), such as managing finances or medication (Reppermund et al., 2013; Stogmann et al., 2016), may be early signs of cognitive impairment leading to dementia (Jessen et al., 2020; Roehr et al., 2019). Older adults with SCD may be less capable of performing daily living activities (Cornelis et al., 2017; McAlister & Schmitter-Edgecombe, 2016; Stogmann et al., 2016), affecting their needs for mobility, personal care, or social engagement. Longitudinal studies among community-dwelling older adults have found that difficulties with cognitively more demanding ADLs may precede mild cognitive impairment (Reppermund et al., 2013; Roehr et al., 2019). When these needs are unmet due to inadequate coping or healthcare resources, older adults’ mental well-being might be negatively affected (Bouldin et al., 2021; Sin et al., 2015), increasing their risks of developing SCD.
There is substantial evidence of the association between SCD and psychological distress. The experience of SCD in older age often presents more challenges that may lead to a higher risk for psychological distress. Psychological distress may include factors such as anxiety and depression (Caselli et al., 2014) and could be represented in mentally unhealthy days (MUDs) (Edwards et al., 2016). MUDs are the average days within a month when an individual feels not mentally well (Centers for Disease Control and Prevention [CDC], 2000). The association between SCD and psychological distress has been examined in several studies. In a cross-sectional study using the 2013 Behavioral Risk Factor Surveillance System (BRFSS) data, women with SCD were reported as having 14 or more MUDs than men, which may adversely impact their quality of life (Edwards et al., 2016). Other cross-sectional studies showed that older adults with SCD experienced more psychological distress (Caselli et al., 2014; Komalasari et al., 2022, 2023) and more depressive symptoms (Stogmann et al., 2016). The association between SCD and psychological distress may be influenced by sociodemographic factors, like lower access to healthcare and more difficulties with daily living activities (authors). The effects of functional difficulties on psychological distress may differ within contextual factors. Sociodemographic factors like age or age cohorts (Jessen et al., 2020) and gender (Edwards et al., 2016) have been reported to vary the association between psychological distress and SCD.
The experience of subjective decline in cognition may vary across income levels. Although there is strong evidence of higher income being associated with SCD (Gupta, 2021; Taylor et al., 2018), a different study showed that income levels were not directly associated with SCD but rather through other factors, such as unmet physical or psychological needs (Bouldin et al., 2021; Peterson et al., 2019), suggesting further investigation of its impact on SCD reporting. Aging studies aiming at understanding factors modifying the association between functional difficulties, psychological distress, and SCD were limited to age-cohort effects, with the middle-old age cohort showing the most substantial effect (Komalasari et al., 2022, 2023). Less understood, however, is how this association is influenced by income levels. Therefore, this study examined the association between SFD and SCD and whether the association is mediated through MUDs and moderated by income levels. The findings will clarify the associations among these variables among older adults to inform interventions to improve their quality of life.
Methods
Design
Using the 2019 wave of the BRFSS data from the Centers for Disease Prevention and Control (Centers for Disease Control and Prevention, 2019), this study cross-sectionally examined the association between SFDs and SCD and whether MUDs mediated this relationship. Additionally, we evaluated whether the indirect effect of MUDs was moderated by income levels. The BRFSS dataset is a large nationally collected database of community-dwelling individuals aged 18 + in the U.S. The SCD data was from an optional Cognitive Decline survey with data among adults 45 years and older, collected by an overall 24 U.S. states in 2019 (CDC, 2019).
Following this conceptual model (see Figure 1), we addressed the following research questions:
Are higher subjective functional difficulties associated with higher risks for SCD, accounting for age, gender, education, and race/ethnicity? Are the effects of greater subjective functional difficulties on higher risks for SCD mediated by MUDs, accounting for age, gender, education, and race/ethnicity? Do income levels moderate the MUDs’ conditional effect in the association between greater SFD and higher SCD risks, accounting for age, gender, education, and race/ethnicity? Are the odds of SCD higher in older adults with more frequent MUDs, at greater functional difficulties, and at lower income levels?
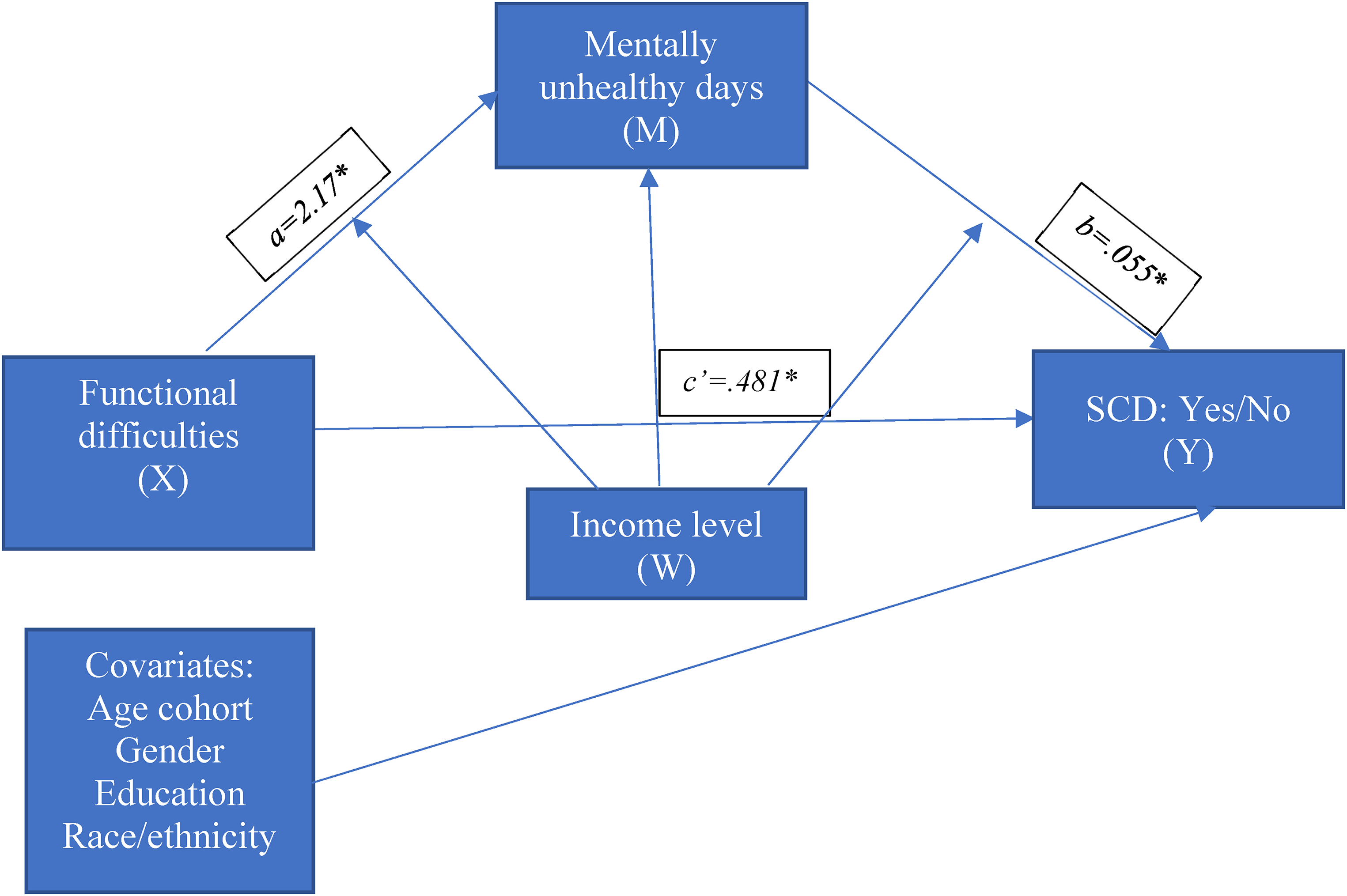
The result of moderated mediational models.
Sample
In this study, we started with 121,099 cases of U.S. older adults living in the community. Of this number, we included 44,778 cases of individuals aged 65 + . We then omitted responses like “Don’t know/not sure” and “Refused.” We treated missing data with mode or mean imputation as the missing cases were lower than 10% for each variable, leaving 13,160 cases for analysis.
Variables and Measurement
The following covariates were included in the moderated mediation model in this study: age cohorts (65–69, 70–74, 75–79, ≥ 80), gender (males and females), education (i.e., completed high school, completed college or technical school, attended college or technical school, and did not complete high school) and race/ethnicity (i.e., White, Black or African American, American Indian or Alaskan Native, Asian, and no preferred race). We accounted for the sociodemographic factors following previous evidence that age (i.e., age 60 + [Jessen et al., 2020], gender [Edwards et al., 2016], education attainment [Gupta, 2021], and race/ethnicity [Gupta, 2021]) were associated with SCD.
SCD was a binary variable of yes or no response, operationalized by the question, “During the past twelve months, have you experienced confusion or memory loss that is more often or getting worse?” (Centers for Disease Control and Prevention (CDC), 2019).
SFDs were assessed by three yes/no questions: (1) “Do you have serious difficulty walking or climbing stairs,” (2) “Do you have difficulty dressing or bathing,” and (3) “Because of a physical, mental, or emotional condition, do you have difficulties doing errands alone such as visiting a doctor's office or shopping?” (CDC, 2019). The overall scores of these three yes/no questions were summed up. We created two levels of functional difficulties: a total score of 0–1 denoted fewer functional difficulties, and scores of 2–3 indicated more functional difficulties.
The MUDs variable was operationalized by the following question, “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” (CDC, 2019). The MUD is a continuous variable with scores ranging from 0 to 30; fewer reported days represent better mental health. The measure's soundness has been confirmed in the literature (Moriarty et al., 2003).
Income levels refer to the annual household income (CDC, 2019), consisting of five levels in this study: (1) < $15,000, (2) $15,000 to < $25,000, (3) $25,000 to < $35,000, (4) $35,000 to < $50,000, and (5) ≥ $50,000.
Inclusion Criteria
The inclusion criteria are individuals aged 65 to ≥80 years old.
Institutional Review Board Approval
Our study is a secondary analysis of the BRFSS, publicly available data from the Centers for Disease Prevention and Control. We did not preregister the study for our scientific writing, perceiving no conflict of interest or consent for publication.
Data analysis
The study population was characterized by employing descriptive statistics (i.e., frequency and percentage for categorical variables). We used mean and standard deviation for numerical variables. The association between each categorical independent variable (i.e., SFD and income levels) with SCD was examined using the Chi-square test. A t-test was used to assess the correlation between continuous independent variables (MUDs) and SCD. After, we performed a multiple logistic regression analysis to ascertain their associations (see Table 1). We included demographic variables (i.e., age cohort, education, education, and race/ethnicity) to check if the association changes (Table 2, adjusted model). The final model reported both unadjusted (OR) and adjusted odds ratios (AOR) and corresponding 95% confidence intervals (CI). All statistical analyses were performed using Statistical Package for Social Science version 28.0 (IBM Corp, Armonk, NY, USA). The statistical significance was assessed at the 0.05 level.
The Characteristics of the Study Participants (N = 13,160).

SFDs=subjective functional difficulties; SCD=subjective cognitive decline; MUDs=mentally unhealthy days.
Independent Unadjusted and Adjusted Effects of the Study Observed Variables on the Odds of SCD in the U.S. Older Adult Sample in 2019 (N = 13,160).

Statistically significant 95% confidence interval.
Separated models for each determinant, adjusting by age, gender, education, and race/ethnicity.
With the exception of MUDs, all other predictor variables were on a categorical measurement scale.
SFDs=subjective functional difficulties; SCD=subjective cognitive decline; MUDs=mentally unhealthy days.
Mediational Analysis
The mediation effect was tested with Model 4 of the PROCESS V.4.0 macro for SPSS (Statistical Package for Social Sciences) (Hayes & Andrew, 2014) with the dichotomous outcome (Y: SCD) (Vanderweele & Vansteelandt, 2010). We evaluated the 95% CI for mediation effects with 5,000 bootstrap samples to test the theoretical model. If 95% CI did not include 0, the statistics were considered statistically significant (Hayes & Andrew, 2014; Hayes, 2018), suggesting that MUDs indirectly impact the association between SFD and SCD.
Moderated Mediation Analysis
The moderation variable (income levels) had five categories: income level 1 (<$15,000), income level 2 ($15,000 to <$25,000), income level 3 ($25,000 to <$35,000), income level 4 ($35,000 to <$50,000), and income level 5 (≥$50,000) to explain the income level moderation effect (Preacher & Hayes, 2004). We utilized Model 59 of the PROCESS V.4.0 macro for SPSS to test if income levels had a moderating impact (Hayes & Andrew, 2014).
Results
Sample Characteristics
In total, 13,160 older adults were included in the analysis (5,790 males [44%], 7,370 females [56%]), with ages ranging from 65 to ≥ 80. Table 1 shows that most participants had SCD (11,614 or 88.3%) and fewer SFDs (n = 12,034, 91.4%). Those with SCD experienced more frequent psychological distress (MMUDs = 4.18, 95% CI ± .256) than those reporting no SCD (MMUDs = 1.89 (95% CI ± 5.85, p < .001) and earned less than those reporting no SCD for each income category. Those with higher functional difficulties reported more frequent psychological distress than those in the lower SFD group (Mdifference in MUDs = 4.38 (95% CI ± 0.310, p < 0.001). Most of the participants were White (12,203 or 92.7%), completed at least high school (9,092 or 69.1%), and had an income of ≥ $50,000 (5,570 or 42.3%).
Research Question Results
RQ1: Higher Subjective Functional Difficulties are associated with higher odds of SCD
Using Model 4 in the SPSS macro by Hayes and Andrew (2014), we examined whether MUDs mediated the relationship between SFD and the odds of SCD. Greater SFDs were associated with higher odds of SCD (β = 0.481, z = 17.41, p < .001), and the direct predictive effect of SFD on SCD was still significant when MUDs (the mediating variables) was added (see Table 3). RQ 2: Mentally unhealthy days mediated Subjective Functional Difficulties and SCD
Testing the Mediation Effect of MUDs Between SFD and SCD Among Older Adults in the U.S., 2019.

CI=confidence interval; LL=lower limit; UL=upper limit; SFDs=subjective functional difficulties; SCD=subjective cognitive decline; MUDs=mentally unhealthy days.
*p < .001; **p < .05
MUDs were also positively associated with SCD, β = 0.055, z = 17.41, p < .001 (see Table 3). Therefore, SFD was associated with SCD via the MUDs, B = 0.119, SE = 0.009, 95%CI 0.102, 0.147, indicating that MUDs mediated the association between SFD and SCD. RQ 3: Income levels moderated the MUD's conditional effects in the Subjective Functional Difficulties-SCD relationship, with the most substantial impact on the lower income levels.
Model 59 of the PROCESS macro method was used to test the moderated mediation model by income levels. We created dummy variables for five income levels as a moderator, where income level 1 was used as a reference. Moderator 1 (W1) represented income level 2 ($15,000 to <$25,000) versus 1 (< $15,000), moderator 2 (W2) defined income level 3 ($25,000 to < $50,0000) versus 1 (< $15,000), moderator 3 (W3) represented income level 4 ($35,000 to < $50,0000) versus 1 (<$15,000), and moderator 4 (W4) defined income level 5 (≥ $50,000) versus 1 (< $15,000) (see Table 4).
Testing the Moderated Mediation Effect of Income Levels on SCD Among Older Adults in the U.S., 2019.

*p < .001; **p < .05; ***p > .05.
Income levels: (1) < $15,000, (2) $15,000– < $25,000, (3) $25,000– < $35,000, (4) $35,000– < $50,000, and (5) ≥ $50,000.
W1 (Income level 2 vs. 1), W2 (Income level 3 vs. 1), W3 (Income level 4 vs. 1).
SFDs=subjective functional difficulties; SCD=subjective cognitive decline; MUDs=mentally unhealthy days; LL=lower-level confidence interval; UL=upper-level confidence interval.
After the income levels were added to the model, only the interaction term between MUDs and W2 (income levels $35,000 to < $50,000 vs. <$15,000) was statistically significant in predicting MUDs (bsimple = −1.08, 95% CI −1.66, −4.50) (Table 4, Model 1). The interaction terms of MUDs and W1, W2, W3, and W4, respectively, were statistically significant in predicting the odds of SCD (bsimple = −0.041, 95% CI −0.062, −0.020), (bsimple = −0.041, 95% CI −0.065, −0.017), (bsimple = −0.030, 95% CI −0.054, −0.006), (bsimple = −0.036, 95% CI −0.057, −0.015) (Table 4, Model 2). Additionally, the indirect effect value of MUDs on the association of SFD and SCD was statistically significant for all income levels, with income level 1 (< $15,000) showing the strongest effects, signifying a moderated mediation effect (bsimple = 0.216, 95% CI 0.152, 0.289) (see Table 5). RQ 4: The odds of SCD reporting are higher among older adults with more frequent MUDs, higher functional difficulties, and lower income levels
Mediating Effect Values at Different Levels of Income Levels Among Older Adults in the U.S., 2019.

CI=confidence interval; LL=lower limit; UL=upper limit.
Logistic regression models are presented in Table 2 for each determinant. The association between SFD and MUDs, respectively, and SCD was still significant after accounting for the sociodemographic covariates (i.e., age, gender, education, and race/ethnicity). The effects of SFD on SCD were mediated through MUDs (b = 0.235, 95% CI 0.915, 0.279). Greater difficulties in functioning were associated with 2.5 times the odds of SCD reporting in older adults (AOR = 2.50; 95% CI: 2.14, 2.91). Increased MUDs were associated with 1.06 times the odds of reporting SCD (AOR = 1.06; 95% CI: 1.05, 1.07). The logistic regression analysis used an income level of < $15,000 as a reference group. Those earning ≥ $50,000 had lower odds of SCD reporting than those earning < $15,000 (AOR = 1.24; 95% CI: 1.18, 1.31).
Discussion
Our study findings indicated that SFD is associated with the odds of SCD through mediation by MUDs. Specifically, greater SFDs were associated with higher SCD reporting, consistent with previous research findings among older adults in cross-sectional (authors) and prospective studies (Roehr et al., 2019). That MUDs mediated the association between SFD and SCD (authors) was confirmed in this study; however, in the current study, we included the cases of people with and without SCD in the model, represented by dichotomous SCD variables, to examine the odds of SCD. Our study results also showed that more frequent MUDs were associated with a slightly higher risk of reporting SCD. However, although the effect of MUDs on SCD is statistically significant, it was not as substantial. Therefore, the interpretation of this finding needs to be taken carefully. Nonetheless, using MUDs in the psychological distress assessment is timely as it effectively indicates health needs, outcomes, and perceived psychological symptoms (CDC, 2000; Mullahy et al., 2011).
This study showed that the indirect effect of MUD in the SFD-SCD relationship was moderated by income levels, with < $15,000 per annum earnings having the most prominent effects than those with an income level of ≥ $50,000 per annum. Specifically, higher income attenuated the effect of SFD on SCD reporting than lower income after accounting for age, gender, education, and race/ethnicity. These findings aligned with previous findings from a cross-sectional study using the 2015 and 2016 BRFSS dataset on cases of adults aged 45 + examining state income inequality (Peterson et al., 2019). The study revealed that those with an annual household income of less than $10,000 were five times more likely to report SCD than those earning $75,000 (Peterson et al., 2019).
Income levels also moderated the association between psychological distress and SCD reporting. That income levels were associated with mental health has been reported in an Australian prospective cohort study among adults 45 years old and over, such that those with shorter educational years tended to have poorer mental health at lower income levels (Sperandei et al., 2023). It may be that older adults from lower-income households cannot afford formal caregiving or social support to meet their daily activity needs (Bouldin et al., 2021), accentuating the SCD reporting.
Limitations and Implications
There are limitations to this study. First, this study utilized self-report data from the secondary dataset (i.e., the 2019 BRFSS dataset). As suggested by Krohn et al. (2013), the use of self-report data could result in underestimating or overestimating the true association among the observed variables from underreporting or overreporting. This study is cross-sectional; thus, the temporal sequence cannot be established (Brown et al., 2022) between having greater functional difficulties, mental distress, and SCD. To enhance the validity of future studies, researchers could use different methods to measure variables, such as using actigraphy or sensors to record daily steps, movements, and daily activities (Yakhia et al., 2014; authors). Also, longitudinal research would generate more valid findings, and practitioners who work with clinical aging populations should be cautious when applying these results according to our nonclinical samples. SCD is often comorbid with depressive symptoms (Stogmann et al., 2016; Zullo et al., 2021), which was not accounted for in this study, potentially overestimating the frequency of older adults being mentally unhealthy and the likelihood of SCD. Future studies should consider depressive symptoms and other potential psychological confounders influencing SCD in the study model.
Implications for Practice
As person-centric interventions are needed, it is becoming increasingly important to understand how frequent MUDs affect the relationship between greater SFDs leading to SCD among the aging population. Knowledge of the significant role that psychological distress and functional difficulties may play in contributing to SCD could help nurses and gerontologists in intervention designs and healthcare delivery. Specifically, nurses working in general and geriatric practice settings may integrate early recognition of cognitive changes for better care management and health outcomes (Roehr et al., 2019). Although ADLs are commonly preserved in people with SCD, discussions about subtle changes in everyday activities may be a cost-effective way to protect them from further neurodegenerative disease (Roehr et al., 2019) as subjective changes in cognition can start years before a diagnosis can be established (Jessen et al., 2020; Stogmann et al., 2016). Nurses working in the community can provide or refer older adults and their families to utilize in-home or community services to help with their daily functioning, thus improving their mental well-being (Lam et al., 2014).
Conclusions
Our study analyzed how SFD are associated with SCD reporting via the potential indirect pathway of psychological distress in a sample of older adults in the U.S. Greater significant SFDs and more frequent MUDs are associated with higher SCD reporting in older cohorts of adults with lower income levels (< $15,000 per annum). Our study extends previous findings by demonstrating that greater SFDs are associated with higher odds of SCD through more frequent MUDs, with higher income levels being associated with more SCD reporting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Thiamwong has received funding from the National Institute on Minority Health and Health Disparities (NIMHD) (R01MD018025; PI Thiamwong) of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.