
Abstract
Introduction
Mental health nurses (MHNs) are categorized as demanding specialists with high levels of stress, and their career is recognized as a high-risk career
Objective
The study aims to assess the relationships between psychological well-being (PWB), mental distress, and resilience among MHNs. Also, it aims to identify the significant predictors of the psychologic well-being of MHNs.
Methods
The study utilized a cross-sectional survey design with a random sample of 250 MHNs who were requested to complete DASS 21, Ryff's scale of PWB and Connor Davidson's resilience scale.
Results
The results revealed that two-thirds of nurses reported either a severe or extreme level of stress (n = 166, 66%), and more than half experienced a severe to extreme level of anxiety (n = 140, 56%). Approximately 25% of MHNs reported a severe to extreme level of depression (n = 62, 25%). The results also indicated that there is a statistically significant negative relationship between PWB subscales and DASS 21. The results indicate that the depression subscale is significantly varied based on the demographic characteristics of nurses. Similarly, this is the case for the anxiety and stress subscales.
Conclusion
The study showed that MHNs’ resilience intervenes with perceived mental distress. Enhancing MHNs resilience would improve PWB and mental health. The study results conclude that MHNs with a high level of resilience reported lower mental distress and a better working environment. Thus, MHNs should be introduced to crisis intervention in order to improve resilience levels.
Introduction
Mental health nurses (MHNs) are categorized as demanding specialists with high levels of stress, and their career is recognized as a high-risk career (Luan et al., 2017), where occupational stress impacts their mental health, job satisfaction, and overall quality of life (Chen et al., 2022). With different stressors, including occupation violence, increased workloads, low staff recognition, poor nurse–patient relationships, and poor professional relationships, they face a high risk of developing psychological problems such as depression and anxiety (Hsieh et al., 2021; Gabrielsson et al., 2016).
Additionally, MHNs have a working environment that is more severe and associated with the nature of disease, working in a closed environment, and the prevalence of frequent violence episodes (Niu et al., 2019; Itzhaki et al., 2018). MHNs face stressors in their work environment that negatively affect their psychological well-being (PWB) and cause mental distress. This can impact their therapeutic work capacity, professional relationships, and work performance (Delgado et al., 2021).
Previous studies have addressed the issue of PWB among mental health nursing professionals. According to Aksu (2020), mental health nursing professionals play significant roles in healthcare services, and therefore they should have better levels of PWB to provide efficient, effective, and quality care. Kameg et al. (2021) examined the PWB of MHNs and related factors. It has been identified that the PWB of MHNs is determined by several factors, including depressive syndromes, burnout, and professional fulfillment (Kameg et al., 2021).
Review of Literaure
Regarding the PWB of MHNs, those MHNs with a postgraduate level of education as well as working in outpatient mental health settings have been found to have high levels of PWB compared to their counterparts (Kameg et al., 2021; Delgado et al., 2021). Studies carried out in China (Lu & Zhong, 2015) and Australia (Maharaj et al., 2018) have reported low levels of PWB among MHNs. Therefore, giving more attention to the PWB of MHNs is an important issue in present healthcare settings.
Challenges in providing quality mental health nursing care due to time constraints, negative team culture, unsupportive leadership, and lack of organizational resources can result in distress and frustration, with some nurses choosing to leave the work setting (Foster et al., 2018). Consistent with the wider field of nursing, MHNs who perceive their work to be stressful report lower work satisfaction (Itzhaki et al., 2018), leading to higher turnover intention and attrition.
Mental healthcare professionals experience psychological problems that affect their psychological status including role conflicts, fear, and anxiety. MHNs face various attacks, abuse, and other occurrences associated with caring for patients with mental health disorders leading to mental distress (Wang et al., 2022). Stress among MHNs is associated with different sources including inadequate resources, role conflicts, poor support, and difficulties in coping with emotions from patients and family members. With such a demanding profession, distress faced by MHNs has a great effect on their psychological state and mental health thus worsening their PWB (Hsieh et al., 2021). MHNs have been associated with having increased mental health problems because of long working durations and stressful work settings. Previous studies showed that MHNs who had a low-stress level had a higher likelihood of having mental distress and poor PWB as well as lower work satisfaction (Niu et al., 2019).
Workplace violence may be classified into many categories, including physical, psychological (emotional), sexual, and racial. Both physical and psychological violence are prevalent; however, psychological violence seems to be more prevalent (Liu et al., 2019). Psychological violence encompasses deliberate actions directed against an individual or group, leading to detrimental effects on their physical, mental, spiritual, moral, and social well-being. This kind of violence encompasses several manifestations, such as insults, threats, assaults, and verbal abuse (Aljohani et al., 2021). The extensive prevalence of violence has significant implications for the provision of healthcare services, hence impacting the overall quality of treatment. Furthermore, the equitable availability of basic healthcare services in developing nations may be compromised if healthcare professionals, who are already in short supply, choose to leave their field due to the risk of violence (Kumari et al., 2022).
Due to challenges and changing environments in the context of healthcare, resilience has been a significant factor in the mental health nursing profession (Hussien, 2022). Resilience is regarded as a dynamic person-environment and interactive process during change and adversity (Delgado et al., 2022). Resilience entails emotional regulation, cognitive processes, and behavioral processes, along with protective interpersonal, personal, and environmental factors. The importance of resilience in mental health nursing has been illustrated by previous studies. For instance, an integrative review conducted by Bui et al. (2023) showed that resilience programs enhanced awareness of personal resilience, the capacity to develop coping skills, self-confidence, and professional relationships. In mental health workplace settings, resilience entails affective, cognitive, and behavioral self-regulation comprised of both internal resources (i.e., positive affect regulation and cognitive appraisal) and external resources (support) that enable nurses to adapt as well as restore their optimal functional ability following adverse events in their workplace (Bui et al., 2023). In a multi-center cross-sectional study conducted, resilience was established as an essential factor for mediating the role of occupational stress and mental health among MHNs (Chen et al., 2022). In another study, Lara-Cabrera et al. (2021) revealed that resilience was significant in mediating the role of occupational stress, depression, anxiety, and mental distress among MHNs. The resilience of MHNs has been less studied compared to resilience among other nursing professionals. The relationships between resilience and PWB remain scanty due to the limited available information, namely in Saudi Arabia. The study aims to assess the relationships between PWB, mental distress, and resilience among MHNs. Also, the study aims to identify the significant predictors of the psychologic well-being of MHNs.
Materials and Methods
Design
The study used a descriptive cross-sectional paper survey design. The study design was selected because it allows for the comparison of many variables at the same time over a short period of time (Grove & Gray, 2018).
Research questions
- What are the relationships between PWB, mental distress, and resilience among MHNs? - What are the significant predictors for the psychologic well-being of MHNs?
Sample
Simple random sampling was used in this study to select the participants. In this study, the sample size was estimated using Raosoft software, with a level of significance of 5% and a confidence level of 95%. Then, the required sample size was 250 participants.
Inclusion and Exclusion Criteria
The study participants included MHNs. The inclusion criteria were all MHNs who worked at Erada Complex For Mental health Hospital and were willing to take part in the study. The main reason for not including years of experience as the main inclusion criteria is because the researchers were interested in understanding this issue generally among MHNs. However, the results of the study were compared according to years of experience. Also, those nurses who worked in administrative positions were excluded. Anyone who did not meet the previous criteria was excluded.
Setting
The study was carried out at Erada Complex For Mental health Hospital because it is the main hospital in Erada Complex For Mental health Hospital. It has been running for 37 years, since 1986. Erada Complex For Mental health Hospital has a 300-bed capacity with 585 MHNs. This is one of the main mental health hospitals in the region, serving the western province of the kingdom. It is a tertiary hospital with many inpatient settings and outpatient clinics. It is a government hospital providing treatment for addiction and all mental health disorders. Offering psychiatric, psychological, and social care
Data Collection Procedure
Upon obtaining ethical approval, the study authors arranged a visit to the hospital and explained the study purpose to potential participants. Then, they received the information sheet and requested to return the signed consent form, as well as being assured about confidentiality. The researcher created a set of random numbers (AH), and participants agreed to take part in the study. They were assigned a random number, and an independent researcher selected 250 random numbers from the pool. The selected study participants received a study package, including a questionnaire, and were asked to return it within 2 weeks. The researcher sent a WhatsApp reminder after 2 weeks to submit the completed questionnaire.
Research Instruments
Demographic Questionnaire
The demographic questionnaire includes age, gender, marital status, level of education, and year of experience.
Ryff's Scales of Psychological Well-Being (PWS) 18
Ryff and Keyes- short form- 10, designed an instrument to assess six aspects of PWB. The short form of the Ryff Psychological Well-being (Ryff & Keyes, 1995). The questionnaire has 18 questions and includes six dimensions: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and the Self-acceptance. To measure these six dimensions. There are three questions for each dimension. The subject is asked to read the questions and answer questions using a 7-point Likert rating scale, with the following responses: strongly agree (1), somewhat agree (2), a little agree (3), neither agree nor disagree (4), a little disagree (5), somewhat disagree (6), strongly disagree (7). Higher scores reflect higher levels of PWB. The internal consistency reliability is 0.85 (Ryffel & Wirth, 2016). In the current study, the internal consistency reliability coefficient was 0.85.
Depression, Anxiety, and Stress Scale (DASS −21)
The psychological state is assessed by DASS 21. Each item is scored on a 4-point Likert scale from 0 to 4. The scale assesses anxiety, stress, and depression. Each division has severe questions. The highest score indicates a higher level of distress. The severity of the depression potential score is normal (0–9), mild depression (10–12), moderate depression (13–20), severe depression (21–27), and extremely severe depression (28–42). As regards anxiety, normal (0–6), mild anxiety (7–9), moderate anxiety (10–14), severe anxiety (15–19), and extremely severe anxiety (20–42) (Lovibond & Lovibond, 1996). Anxiety subscale: normal (0–10), mild stress (11–18), moderate stress (19–26), severe stress (27–34), and extremely severe stress (35–42). The scale has a good internal consistency reliability of 0.87 (Jiang et al., 2020). In the current study, the internal consistency reliability coefficient was 0.88.
The Connor Davidson Resilience Scale
The CD-RISC has 25 questions. Each question is rated on a Likert scale. The potential score ranges from 0 to 100, with higher scores reflecting greater resilience. The Cronbach alpha of the scale is 0.84 (Cusack et al., 2016). In the current study, the internal consistency reliability coefficient was 0.87
Statistical Analysis
Data were analyzed using (SPSS) version 26. Descriptive analysis: frequency, percentage, mean, and standard deviation (SD) were used to describe the distribution of the study participants’ sociodemographic variables. Continuous data such as age. Categorical variables such as gender were presented as proportions or percentages. Independent sampling t-test and one-way ANOVA were used to find the difference in the range of study participants according to demographic data and the Pearson correlation test was used to examine the relationship of the study. The level of significance was set at 0.05.
Ethical Considerations
The study was approved by the Fakeeh College for Medical Sciences (440/IRB/2023) and the Ministry of Health (R203/2023). Written informed consent was obtained from all MHNs who agreed to participate in the study, afterexplaining the aim of the study.
Results
Sample Characteristics
There were 400 MHNs assigned to random numbers. Two hundred and fifty participants completed the questionnaire (response rate: 63%). The majority of the participants were males, 139 (55.6%), while the rest were females, 111 (44.4%). 52.8% (132) of them were aged between 20 and 30 years, and 47.2% were aged more than 31 years. 85.2% had attained at least a bachelor's degree, and 14.2% had a diploma's degree. The two-thirds of the participants, 181 (72.4%), had clinical experience lasting more than 2 years, while 27.6% had clinical experience lasting less than 1 year, as described in Table 1.
Characteristics of the Study Participants (n = 250).

Research Question Results
Descriptive Study Outcome
Psychological Well-being
The study results indicate that the overall average PWB of MHNs is 90.46. Also, the findings demonstrated a high level of PWB among nurses, which was related to personal growth (average 17.65), followed by self-acceptance (16.56). However, the lowest average was found in the autonomy subscale (mean = 12.65), followed by the environmental mastery subscale (average = 13.45). Additionally, around 45% (n = 112) of MHNs had a higher level of PWB (scores above the average).
Mental Distress
The results showed that the average of overall distress is 62.56. The highest average of the DASS subscale related to stress (mean = 22.08), followed by anxiety (average = 21.22), and the least emotional distress reported is depression, as the average is (19.26). Further analysis showed that two-thirds of nurses reported either a severe or extreme level of stress (n = 166, 66%), and more than half experienced a severe to extreme level of anxiety (n = 140, 56%). Approximately 25% of MHNs reported a severe to extreme level of depression (n = 62, 25%).
Resilience
The study results highlighted the highest subscale of resilience derived from trust (average 14.59). However, the least source of resilience derived from the personal competence subscale (11.25). The results showed that one-third of the study participants scored above the average. The results showed that they can manage work pressure by establishing trusting relationships with others, but they have a lower capability to solve issues or difficulties or use self-control to overcome challenges (Table 2).
The Results of Descriptive Statistics of the Mian Study Outcomes.

SD= standard deviation.
The results indicated that there is a statistically significant negative relationship between PWB subscales and DASS 21. The strongest significant correlation was found between autonomy and DASS 21 (stress) (r = -0.58; p=0.05), followed by relationships with others and DASS-stress (r = -0.57; p=0.05), and purpose of life and depression (r = -0.56; p=0.05). This suggests that MHNs with poor PWB were more likely to report psychological problems.
The results showed that there is a statistically significant positive relationship between PWB and the resilience subscale. The strongest relationship reported between autonomy and the personal competence subscale of resilience (r = 0.67; p=0.05) However, a non-significant relationship was found between self-acceptance and all dimensions of the resolution scale (r = 0.07; p > 0.05). This reflects that nurse with positive resilience have higher PWB. The results also demonstrate that there is a statistically significant and negative relationship between DASS subscales and resilience, which suggests that nurses who had poor psychological status showed less resilience with their working environment, as described in Table 3.
Bivariate Correlation Between Psychological Well-Being, Resilience and DASS 21 (Pearson, Spearman Coefficient) (n = 250).

The results indicate that the depression subscale is significantly varied based on the demographic characteristics of nurses. Similarly, this is the case for the anxiety and stress subscales. For instance, female nurses reported higher levels of depression, anxiety, and stress compared to male nurses (p=0.05). In terms of resilience, the positive acceptance dimension is significantly higher among males and those aged more than 40 years compared to their counterparts. However, the PWB of nurses did not differ significantly according to sociodemographic characteristics, as reported in Table 4.
The Results of Comparison Between the Main Study Outcomes and the Study Participants Characteristics (n = 250).

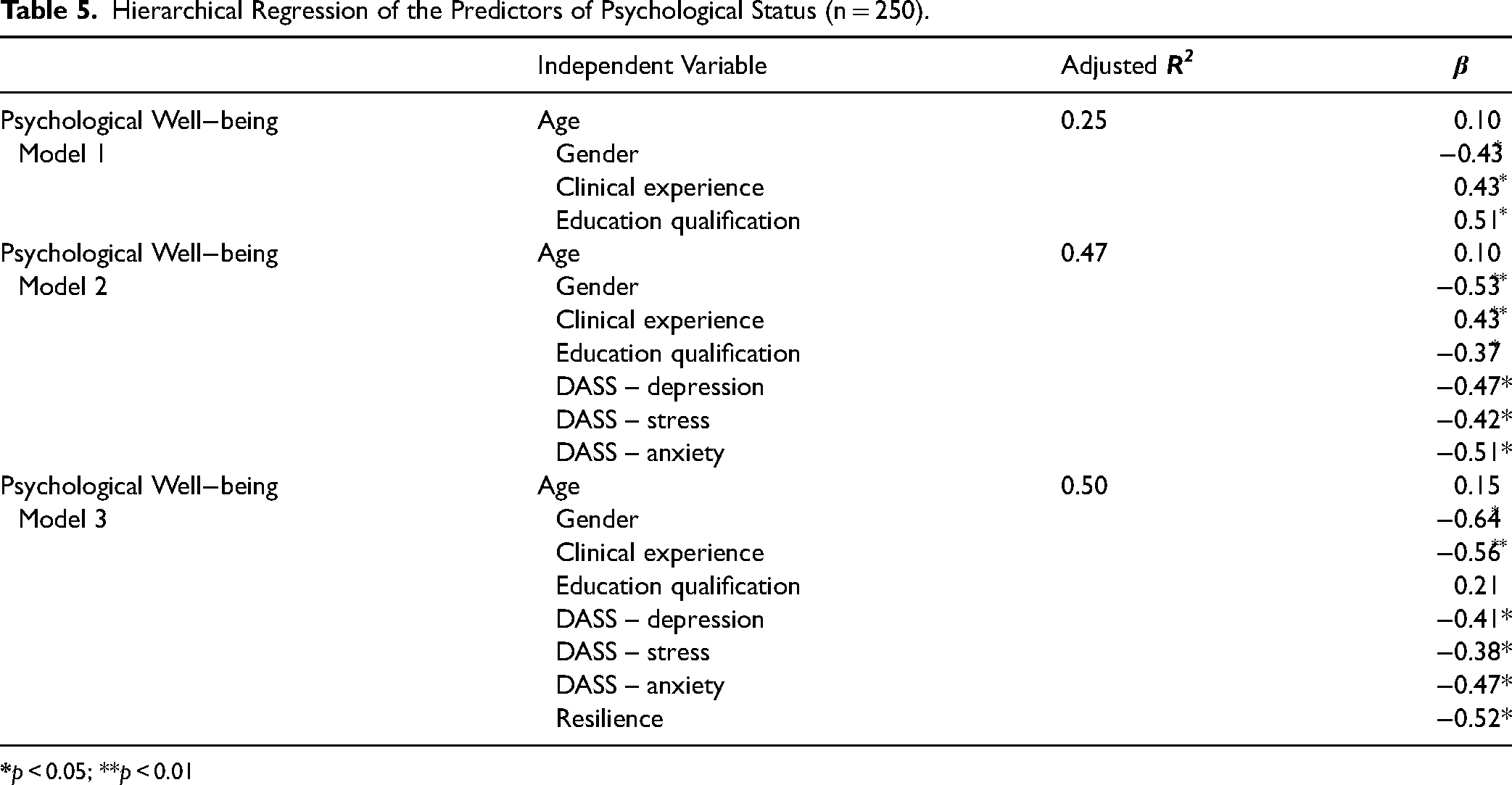
The results of hierarchical regression analysis on the study outcomes and subdomains are summarized in Table 5. In Model 1, the used sociodemographic data explained about 25% of the variance in PWB. The majority of variables showing a significant relationship were entered into the regression equation. The findings revealed that clinical experience, and educational qualification were significant predictors of the PWB of nurses. In model 2, the results showed that 47% of the variance in PWB is explained by the variable entered in regression model 2. For instance, the results showed that PWB is significantly predicted by the demographic data of the study participants (R2 = 0.45, adjusted R2 = 0.20, F = 5.4, p < 0.05), DASS-anxiety (p < 0.05), and DASS-stress (p < 0.05). In Model 3, the results revealed that 50% of the variance in PWB is explained by the enlisted variables. For instance, resilience (R2 = 0.51, adjusted R2 = 0.26, F = 4.9, p < 0.05).
Hierarchical Regression of the Predictors of Psychological Status (n = 250).
Discussion
The present study assessed the relationships between PWB, psychological status, and resilience among MHNs. The overall average PWB of MHNs reported in this study was 90.46. Similarly, Delgado et al. (2021), investigated the levels of PWB, mental distress, and resilience among MHNs in Australia and reported above the average mean level of 85.38 for PWB. A study conducted by Kermen et al. (2016) established a mean score of 38.69 for the PWB scores of the nurses. The PWB of nursing professionals means individualized positive self-perception, knowing oneself, being aware of strengths and limitations, developing quality relationships, and managing challenging situations (Şensoy et al., 2020).
The present study findings identified a weak to strong (r = 0.30 to r = 0.80) positive relationship between resilience and PWB across all stressor categories (consumer/carer; colleague; organizational role; and organizational service). Based on the findings, weak to moderate (r = 0.31 to r = 0.55) positive relationships between resilience and PWB were observed. In support of these findings, a descriptive cross-sectional study carried out by Foster et al. (2020) also revealed weak to strong (r = 0.301 to r = 0.750) positive relationships between resilience and PWB across Foster et al. (2020) also identified weak to moderate (r = 0.306 to r = 0.549) positive relationships between resilience and PWB. Similarly, Delgado et al. (2021), investigated the levels of and relationships between PWB, mental distress, and resilience in MHNs in Australia and reported that PWB showed strong positive and negative relationships, respectively, with resilience (r = 0.571, p < 0.01) and depression (r = -0.563, p < 0.01).
In terms of psychological status, the results of the current study showed that MHNs reported high levels of stress, anxiety, and depression. Thus, poor psychological status is negatively correlated with resilience and PWB. This result is in line with the study of Foster et al. (2019), who documented that MHNs had a high level of workplace stress, and the effects on their health and quality of life were negatively influenced by turnover intention. Also, it has been shown that high levels of occupational stress were linked to “client-related difficulties,” “lack of resources,” and “workload, which caused feelings of emotional challenges (Kunzler et al., 2020; Jarden et al., 2021).
The PWB of nurses included in the study was significantly predicted by gender, clinical experience, and educational qualification. Delgado et al. (2021) identified that PWB was high among MHNs with a postgraduate specialist qualification indicating postgraduate education level is an essential component in enhancing the PWB of MHNs. The findings of the present study on mental distress of MHNs showed that they experienced average distress levels with high distress coming from stress, anxiety, and least depression.
Regarding resilience, the results indicated that nurses managed work pressure by developing trusting relationships with others. A study by Delgado et al. (2022), also identified that MHNs employed relational self-care strategies when building and maintaining their well-being. This included establishing trusted relationships with friends, colleagues, and family members. Trusted relationships act as a social connection for resilience among MHNs and well-being. Through engagement with others, MHNs can shift their focus from stressors in the workplace to other life areas, thus keeping boundaries between work and themselves. Professional, trusted relationships essentially help MHNs seek strength, support, and learn from colleagues.
Strengths and Limitations
The main study strength is that the sampling technique is randomized. Therefore, it enhances the likelihood of generalization. Moreover, the study has adopted scales with established psychometric properties. However, the study suffers from some limitations, such as that it has been conducted at one site and the research design used posited a limit control over confounding variables.
Implication to Practice
The findings of this study provide information to various bodies in healthcare, including nursing educators, nursing leadership, nursing professionals, and other healthcare professionals, about the importance of resilience and PWB among healthcare professionals. The concept of resilience not only among MHNs but also among nurses working in various departments and other healthcare professionals has been linked to reduced stress among healthcare professionals, better adaptation to the situations, and also improved and maintained PWB of the nurses. Studies have indicated that reduced levels of burnout, depression, and anxiety among healthcare professionals are due to the high levels of resilience shown by healthcare professionals (Arrogante & Aparicio-Zaldivar, 2017)
Conclusion
The study results conclude that MHNs have high resilience levels in their respective working environments and therefore have the self-competence to deal with challenges. Improving the levels of resilience among MHNs is an important intervention in enhancing PWB among MHNs.
Footnotes
Acknowledgements
The study authors acknowledged nurses who participated in the study
Author Contribution Statements
AH and NS designed the study. AH and NS collected and analyzed data. AH and NS wrote initial draft and final paper.
Tracked Changes or Comments where the poster's name is listed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Institutional Review Board of Fakeeh College for Medical Sciences (440/IRB/2023) and MOH (R203/2023)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.