
Abstract
Introduction
During the COVID-19 pandemic, nurses have faced various nurse-specific traumas in their workplaces, but there is limited understanding of the resulting outcomes and factors that contribute to them.
Objective
To address this gap, the study employed the middle-range theory of nurses’ psychological trauma (NPT) to examine these relationships among frontline nurses working in critical care areas.
Methods
In a quantitative cross-sectional study, the study compared nurses identified as probable cases of posttraumatic stress disorder (PTSD) with those identified as not probable cases. The study investigated the nurse-specific traumas they experienced, their individual personality traits, and the buffers they possessed. The study also sought to identify specific types of nurse-specific traumas that could be associated with negative outcomes, such as alcohol and drug use.
Results
It was found that PTSD-probable nurses reported higher levels of trauma from disasters and system/medically induced trauma compared to not-probable nurses. They also experienced more nonwork-related humankind traumas and displayed lower resilience. Furthermore, PTSD-probable nurses identified with trait urgency and trait avoidance motivation. Additionally, trauma from disasters was associated with alcohol use.
Conclusion
The study highlights the elevated levels of trauma, lower resilience, and specific psychological traits associated with PTSD-probable nurses, emphasizing the need for targeted interventions and support to mitigate the negative outcomes experienced by frontline nurses.
Introduction
Registered nurses render care for our physical and mental health 24/7, which is tightly linked to our well-being. Paradoxically, the well-being of nurses is frequently overlooked (Bauer-Wu & Fontaine, 2015; Maben & Bridges, 2020). Lower nurse-to-patient ratios are associated with fewer medical errors and deaths, better overall patient treatment, and reduced rates of nurse burnout (Blouin & Podjasek, 2019; Kane et al., 2007). The COVID-19 pandemic has led to an increased awareness of the tight link between a healthy nursing workforce and a healthy nation: The number of healthy nurses translates to the number of lives saved. The COVID-19 pandemic overwhelmed healthcare personnel in significant ways, including a lack of personal protective equipment (PPE), staff, and the ability to test for those who were infected with the virus (Cho et al., 2021). Nurses, as well as other healthcare providers, experienced elevated stress as a result of their working conditions. Moreover, nurses are at risk for experiencing several kinds of psychological trauma often daily, such as insufficient resource trauma (e.g., lack of PPE, training/knowledge, testing kits, etc.), trauma from disasters, and second-victim trauma (Foli, 2022).
Review of Literature
Psychological trauma, although experienced transiently at the workplace, may lead to a wide variety of sustained negative outcomes. Some of the negative outcomes are psychological such as an increased level of anxiety (e.g., risk of infection), depression (Serrano et al., 2021), or posttraumatic stress disorder (PTSD) symptoms (Schuster & Dwyer, 2020), while others are behavioral such as increased alcohol or drug intake or suicide (Reger et al., 2020). Since the start of the global COVID-19 pandemic, there has been repeated mention of nurses feeling guilty, frustrated, and exhausted due to the changes in the care they can provide, lack of PPE, and increase in their workload (Catania et al., 2021; Dohrn et al., 2022; Leng et al., 2021). Furthermore, increasingly, nurses reported increased PTSD symptoms, stress (Greenberg et al., 2021; Leng et al., 2021), and also anxiety due to the inability to properly care for their patients, fear of infecting their families, and lack of consistent COVID-19 protocols (Catania et al., 2021; Leng et al., 2021; Zipf et al., 2022). All these could contribute to their decisions to leave the profession (Mercado et al., 2022). On the other hand, when faced with professional challenges, some nurses have managed to find increased respect and commitment to the profession, a sense of value, professional and public support, and a renewed sense of duty and identity as healthcare providers (Ashley et al., 2021). Even though the factors impacting nurses choosing to leave versus stay are largely unknown, some studies have started to reveal factors affecting resilience and the development of PTSD in nurses (e.g., Levi et al., 2021; Mealer et al., 2017).
According to a recent model called the middle-range theory of nurses’ psychological trauma (NPT) (Foli, 2022), nurses’ lived experiences are more fully understood by understanding humankind/personal and nurse-specific traumas, which may lead to discovering paths to healing and recovery. Developed prepandemic and specific to this theory are seven nurse-specific traumas: (1) insufficient resource trauma, (2) second-victim trauma, (3) workplace violence, (4) trauma from disasters, (5) system/medically induced trauma, (6) historical trauma, and (7) vicarious/secondary trauma. Investigators have provided support for this model and empirical associations between nurses’ psychological trauma and negative outcomes such as substance use (Foli et al., 2020; Foli, Zhang et al., 2021). Within the context of the COVID-19 pandemic, several of these traumas appear to be especially salient, such as insufficient resource trauma, second-victim trauma, trauma in disasters, and system/medically induced trauma. Examples include the shortage of staffing and PPE leading to insufficient resource trauma, nursing errors made that may have been related to insufficient resources (second-victim trauma), and allocation of scarce resources to patients during disasters (trauma from disasters). System/medically induced trauma may also be present as nurses witness the suffering and discomfort of patients tethered to ventilators and being unable to have family present.
Objective
Aligning with the broader effort in the literature to understand what affects resilience and the development of PTSD, the study's primary objective is to provide initial insights into the connections between various variables that may influence nurses’ self-reported psychological trauma. This study represents an ongoing effort to gain a more nuanced understanding of the determinants affecting resilience and the development of PTSD in nurses.
Methods
Design
This study employed a cross-sectional design, incorporating both quantitative and qualitative components. The qualitative data have been published separately (Foli, Forster et al., 2021), while the quantitative data are presented in this report. The quantitative data had two study components. The first study component was a self-report survey, recorded via Qualtrics. The second component included two cognitive control tasks, administered via scripts programmed with JavaScript and HTML languages. The subsequent sections provide a detailed account of the measures utilized in the study. It is important to acknowledge that due to the limited availability of data in the existing literature pertaining to addressing the research questions, the study chose a comprehensive approach by encompassing a broad range of variables, instead of narrowing it down to a more focused set.
Demographics
Participants’ sociodemographic characteristics (e.g., gender, race/ethnicity, etc.) as well as their work demographics (e.g., the unit most frequently worked, work hours per week, etc.) were surveyed.
Nurse-Specific Trauma
Three investigator-generated statements were used for each of the followings six types of traumas: (1) insufficient resource trauma, (2) second-victim trauma, (3) workplace violence trauma, (4) trauma from disaster, (5) system/medically induced trauma, and (6) historical trauma (Foli, 2022). The seventh type of trauma, vicarious/secondary traumatic, was assessed with the validated 17-item Secondary Trauma Stress Scale (Bride et al., 2004). The scale is organized in three subscales to measure intrusion, avoidance, and arousal symptoms by assessing participants’ agreement with statements that reflect their experiences while working with traumatized clients. The total score is derived by adding together the individual item scores, with a higher score indicating a greater frequency of symptoms.
Humankind Trauma and Psychological Symptoms
The 10-item Adverse Childhood Experiences (ACE) (Felitti et al., 1998) and the 17-item life event checklist (LEC) (Gray et al., 2004) were used to assess humankind trauma. ACE evaluates 10 categories of childhood trauma, encompassing five personal and five familial traumas. The total score is calculated by tallying the number of “yes” responses. LEC is created to identify traumatic events in one's lifetime by counting the statements that have been personally experienced, witnessed, and learned about, are uncertain, or do not apply.
Given that this study was conducted at the beginning of the COVID-19 pandemic, the researchers do not know the specific psychological symptoms nurses might be experiencing. Therefore, the researchers included three different scales: (1) primary care posttraumatic stress disorder (PTSD) screen for DSM 5 (PC-PTSD-5) (Prins et al., 2016), (2) Generalized Anxiety Disorder (GAD)-7 (Spitzer et al., 2006), and (3) Patient Health Questionnaire (PHQ)-9 (Kroenke et al., 2001). The PC-PTSD-5 scale is intended for identifying individuals with probable PTSD, and the total score is the number of “yes” responses to the five statements. Meanwhile, the GAD-7 (comprising seven items) and the PHQ-9 (with nine items) assess the frequency of participants’ distress related to anxiety and depression, respectively. In both cases, the total score is calculated by summing the scores of each item.
Buffers
Buffer was assessed using both the six-item Brief Resiliency Scale (BRS) (Smith et al., 2008) and the eight items of the Survey of Perceived Organization Support (SPOS) (Eisenberger et al., 1986). The BRS survey assessed participants’ resilience in bouncing back from negative events, and the total score is derived by averaging the scores for each item. The SPOS gauged employees’ perceptions of the organization's appreciation for their contributions and concern for their well-being, and the total score is computed by adding up the scores for all the items.
Substance Use
The Drug Abuse Screening Test (DAST-10) (Skinner, 1982) and Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993) were used to assess the substance uses. The DAST-10 requires participants to answer 10 questions about drug use with “yes” or “no” responses. The total score is the number of “yes” responses for items 1–2 and 4–10, as well as counting the “no” response for item 3. The score ranges from 0 to 10, with a higher score indicating a more significant and severe level of issues related to drug use. The AUDIT consists of 10 questions, and the total score assesses alcohol consumption and dependence. Scores from 8 to 14 suggest hazardous or harmful drinking, while a score of 15 or higher indicates potential alcohol dependence (moderate–severe alcohol use disorder).
Personality Traits
To complement the task-based assessment of cognitive control, the study included two sets of questionnaires assessing personality traits relevant to cognitive control functioning, the trait avoidance/approach motivation using the Behavioral Inhibition System/Behavioral Activation System (BIS/BAS) scales (Carver & White, 1994) and the trait impulsivity using the short UPPS-P (i.e., urgency, premeditation, perseverance, sensation seeking, and positive urgency) Impulsive Behavior Scale (Cyders et al., 2014). The BIS/BAS scale consists of 24 items, divided into four subscales: BAS drive, BAS fun-seeking, BAS reward responsiveness, and BIS. The short UPPS-P comprises 20 items, extracted from the original UPPS-P scale, which evaluates five aspects of impulsivity. In both scales, the total score is calculated by summing the scores of individual items.
Cognitive Control
Using their computer keyboard, the nurses’ first task was a stop-signal task, designed to assess an individual's inhibitory control function, and the second was a rule-switching task, designed to assess attention control (Friedman & Miyake, 2017). In the stop-signal task, participants were instructed to make a response to “Go” targets and withhold a response to “Stop” targets (Figure 1a). In the rule-switching task, participants were asked to switch between categorizing images of objects as living or nonliving and as larger or smaller than a shoebox (Figure 1b). Participants were told to use the color of the surrounding frame to know which categorization task would be relevant on the current trial, requiring them to either “repeat” the same task they had just performed on the previous trial or “switch” to the other task. In both tasks, participants’ response times and errors (i.e., wrong key pressed or no response) were recorded. Behavioral indexes of each participant's inhibitory control and rule-switching/attention control were calculated.

Examples trails. (a) In the stop-signal task, participants were instructed to categorize faces according to their gender. On “go” trails, participants would respond by pressing a key. On “stop” trails, after a variable “SSD” (i.e., the stop-signal delay), a red frame (i.e., the stop signal) would be presented, instructing participants to cancel any response they may be prepared. If participants failed to cancel their responses, this trail would be a “failed-stop” trail, but otherwise a successful stop trail. Face images were drawn from Ebner et al. (2010). (b) In the rule-switching task, participants first learned about the two rules to categorize images (i.e., Rule #1: whether the picture consists of a living or a nonliving object. Rule #2: whether it consists of an object bigger or smaller than a shoebox). They were told that the color of the surrounding frame indicates which categorization task is relevant on the current trial, requiring them to either repeat the same task they had just performed on the previous trial or switch on the other task. Object images were drawn from Moreno-Martinez and Montoro (2012).
Research Questions
To meet the objective, the study surveyed nurses’ self-reported psychological trauma, the relevant psychological and behavioral outcomes, and assessed individual differences in cognitive control to explore the relationships between these variables. The study employed the NPT framework because it offers a comprehensive perspective on the nurse-specific traumas that are encountered within various nursing specialties and throughout different stages of a nursing career. This framework allows for a more holistic understanding of the potential outcomes of psychological trauma to practicing nurses. The study purposefully sought to gather information for each of the seven types of nurse psychological trauma as well as indicators of humankind/personal trauma to answer the first research question: Which type of nurse-specific trauma is associated with a higher level of stress, anxiety, and depressive symptoms?
In addition to psychological distress, within the NPT framework, one of the targeted outcomes was the use of substances (e.g., drugs and alcohol) by nurses. This led to the second research question: Does a higher level of nurse-specific trauma load lead to substance uses? However, the researchers reasoned that because not all nurses resort to maladaptive coping strategies (e.g., substance use) due to experienced traumas, mediating individual difference factors must exist. Despite greater awareness, understanding, and discourse being introduced in the NPT framework, it does not take into account cognitive control.
As a psychological construct and often objectively measured in cognitive tasks, cognitive control explains how individuals produce goal-directed behavior (Friedman & Miyake, 2017). For example, to implement a new, context-appropriate action plan, such as wearing additional PPE, cognitive control is required to inhibit habitual actions and adapt to new environmental demands. Poor cognitive control has been linked to mental illnesses, including depression, anxiety, PTSD, and substance use (Jagger-Rickels et al., 2021; Polak et al., 2012; J. L. Smith et al., 2014), but the exact relationship remains to be understood. On the one hand, as implicated in the substance use literature, patients suffering from depression and substance use are marked by impaired cognitive control, resulting in their maladaptive decisions and actions (Gustavson et al., 2017; Verdejo-García et al., 2006). On the other hand, trauma experiences or substance use can have long-term cognitive effects (Arble et al., 2023; Brockett et al., 2018).
Some studies focused on nurses have hinted at links between the experienced trauma and its psychological impact (e.g., secondary traumatic stress, burnout, compassion fatigue), but very few have investigated in detail how they are linked. The study, therefore, hypothesize that individual nurses’ cognitive control might play a key role in determining how they respond to the unique stressors and psychological trauma induced by the COVID-19 pandemic. As the first step to explore this relationship, the study's third research question was the following: How does nurse-specific trauma relate to individual differences in cognitive control? To answer this, the study focused on assessing two cognitive control functions in nurses: attention switching and response inhibition. The researchers reason that given nurses’ daily duties involving administering appropriate medications and treatments and collaborating with physicians in implementing patient care plans, their success relies on cognitive control toward (a) implementing new, context-appropriate actions (i.e., rule switching) and (b) inhibiting the inappropriate ones (i.e., response inhibition) in response to changing demands.
Sample
This study was conducted within a specific timeframe, with participant recruitment taking place between June and September of 2020. Throughout the data collection phase, recruitment text was posted through the American Association of Critical Care Nurses (AACN) research webpage as well as sent via email to an alumni list from a public Midwest university. Subsequently, we proceeded to analyze and work with the obtained sample. One hundred and thirty-seven nurses entered the online survey. However, some did not finish and exited in the middle of the survey. The final sample was 110 nurses.
Inclusion/Exclusion Criteria
The study protocol included the following inclusion criteria: (1) nurses who were presently working in critical care areas during the pandemic or had recent experience in such areas, and (2) participants were required to demonstrate proficiency in reading and comprehending English. The study protocol did not specify any exclusion criteria.
Statistical Analysis
Cognitive Control Task
For nurses that also contributed to the cognitive control task component, each nurse's task performance was summarized using mean response time (RT, in millisecond/ms) and mean error rate (ER in percentages/%) for each task. Specifically, for the stop-signal task, the following means were calculated: go ER (%), go RT (ms), stop ER (%), failed-stop RT (ms), and stop-signal delay (SSD). The stop-signal reaction time (SSRT) was calculated using the integration method with the replacement of omission-trial response time. In brief, by estimating the speed of going (i.e., RT on go trials) according to the probability of responding on stop trials (i.e., stop ER) as a function of stop-signal delay, the integration method derives an estimate of the covert speed of stopping (i.e., SSRT) in each subject.
Similarly, in the rule-switching task, the mean ER and RT on rule-switch and rule-repeat trials were calculated in each subject. The “switch cost” variable was derived by calculating the difference between rule-switch and rule-repeat trials in each subject. This provided an estimate of how efficient a participant is with switching between different task sets—i.e., an important cognitive control function. All these variables are continuous. When examining bivariate associations, Pearson correlation was conducted, and the correlation coefficient was tested to see whether the correlation significantly differed from 0.
Ethical Considerations
This study was approved by the Purdue University Institutional Review Board and collected both qualitative and quantitative data online. All participants have provided written informed consent prior to the beginning of the online survey. For completion of the study, participants were compensated with an electronic gift card of $30.00.
Results
Sample Characteristics
Tables 1 and 2 report the response distribution (%) of socio- and work demographics in the entire sample (N = 110). Most of them are female (93.64%), live in an urban area (95.45%), are Caucasian (81.82%), not Hispanic/Latino (93.64%), are married or living as if married (60.00%), earned a bachelor's degree or BSN (74.64%), and have an annual income of $51,000–$100,000 (65.54%). Most nurses were staff nurse/frontline workers (83.64%), worked most frequently in the critical care/critical care step-down units (41.21%), worked for 33–40 hr per week (68.18%), worked in a 12-hr day shift (53.64%), and had cared for COVID-19 patients for at least 4–6 months (62.73%).
Socio-demographics (N = 110).

Note. BSN = Bachelor of Science in Nursing; MSN = Master of Science in Nursing; PhD = Doctor of Philosophy.
Other individuals” includes extended family, young adults, and all ages. Total responses are 114.
Work Demographics (N = 110).

Note. ICU = intensive care unit; PACU = postanesthesia care unit; PICU = pediatric intensive care unit. “Other” category under “units most frequently worked” includes anesthesia, med-surg, resource nurse, telesepsis, COVID-19 unit, and quality.
Select all that apply, N = 199.
“Advanced practice nurse” includes nurse practitioners, certified registered nurse anesthetists, and clinical nurse specialists. “Other” includes clinical educator and clinical resource nurse.
Research Question Results
Comparisons Between Nurses Completing the Survey and Cognitive Control Tasks and Nurses Completing the Survey Only
Due to having two data components, some participants completed both (N = 46, after excluding 3 due to poor performance), while others completed only the survey component (N = 64). To ensure representativeness in the two samples, the researchers compared the characteristics between them. As shown in the last column of Supplementary Table S1, none of the main variables of interest differed between the two groups, except for one: trauma from disaster. This variable was significantly higher for nurses only completing the survey than for those completing both components (P = 0.009). There were no significant differences between the two groups in any of the demographic variables.
Research Question #1: Comparisons Between PTSD-Probable Nurses and PTSD-Not-Probable Nurses
Research question 1 asked which type of nurse-specific trauma is associated with higher levels of psychological symptoms (i.e., stress, anxiety, depression). Since the researchers are interested in nurse-specific trauma, the PC-PTSD-5 was used to identify nurses with a higher level of stress due to traumatic events exposure. According to the PC-PTSD-5 manual (Prins et al., 2016), a score equal and greater than 3 is considered as indicative of PTSD-probable, while a score less than 3 is considered as indicative of PTSD-not-probable. In the sample (N = 109, after excluding one nurse skipping the PC-PTSD-5 items), about half of the nurses were categorized as PTSD-probable (i.e., PC-PTSD-5 score ≥ 3; N = 56), and the other half (49%) were categorized as PTSD-not-probable (i.e., PC-PTSD-5 score < 3; N = 53). The researchers then compared the PTSD-probable nurses and PTSD-not-probable nurses in terms of both nurse-specific psychological traumas as well as “humankind traumas” that are not nurse-specific.
Psychological Symptoms
Means and Standard Deviations of Main Variables of Interest and P-Values (Standard Errors or SE) for Their Differences Between PTSD-Probable Nurses (N = 56) and PTSD-Not-Probable Nurses (N = 53).

Note. ACE = Adverse Childhood Experiences; AUDIT = Alcohol Use Disorder Identification Test; BAS = Behavioral Activation System; BIS = Behavioral Inhibition System; BRS = Brief Resilience Scale; DAST-10 = Drug Abuse Screening Test-10; GAD-7 = Generalized Anxiety Disorder-7; LEC = Life Events Checklist; PHQ-9 = Patient Health Questionnaire-9; PC-PTSD-5 = Primary Care Posttraumatic Stress Disorder (PTSD) screen for DSM 5; POS = Perceived Organizational Support; STSS = Secondary Traumatic Stress Scale; Short UPPS-P = The Short UPPS-P Impulsive Behavior Scale (U = Urgency, P = Premeditation (lack of), P = Perseverance (lack of), S = Sensation Seeking, P = Positive Urgency). The “N” in the parentheses reflected the actual sample size for a particular variable due to some participants skipping questions.
Nurse-Specific and Humankind Trauma
When comparing the two groups in terms of the six types of nurse-specific trauma (except for the secondary trauma), “trauma from disasters” was significantly different between PTSD-probable nurses and nurses who were PTSD-not-probable (t(96.61) = 2.66, P = 0.009). “System/medically induced trauma” showed a trend toward significance (P = 0.065), whereas the other four types of traumas were not significantly different between the two groups of nurses. The seventh type of trauma, secondary trauma, was assessed using Bride et al.’ (2004) Secondary Traumatic Stress Scale (STSS). As this scale focuses on the stress symptoms due to their work with patients (e.g., it seemed as if I was reliving the trauma(s) experienced by my client(s)), PTSD-probable nurses scored significantly higher than those who were PTSD-not-probable on the entire scale (t(98.95) = 8.27, P < .001) as well as on the subscales measuring intrusion (t(98.09) = 6.61, P < .001), avoidance (t(98.18) = 7.72, P < .001), and arousal (t(101.41) = 8.22, P < .001). In terms of humankind trauma that was not nurse-specific, PTSD-probable nurses had more “happened to me” events (LEC) than those who were PTSD-not-probable (t(103.93) = 2.19, P = 0.031). The two groups of nurses did not differ in terms of “witnessed it” events (LEC). Nor did they differ in terms of the ACE score.
Buffers and Work Demographics
Next, the study assessed whether there were other aspects of nurses’ lives (e.g., buffers, personality traits, socio-/work demographics) that differentiates the PTSD-probable group from the PTSD-not-probable group. These comparisons were conducted with two-sample t-tests and are shown in the bottom half of Table 3. Although the two groups did not differ in their SPOS scores, the BRS scores were significantly lower in PTSD-probable nurses than in the PTSD-not-probable nurses (t(99.80) = 4.18, P < .001). Related to this finding was a significant difference in the marital status between the two groups (Χ2(4, N = 109) = 11.08, P = 0.026): More PTSD-probable nurses fell into the broad category of being single (i.e., never married, divorced, widowed) than PTSD-not-probable nurses (note that this result was based on a Chi-square test and there was no standard error associated with it). No other demographic variables significantly differed between the two groups, including variables such as work hours per week, shifts worked, months caring for COVID-19 patients, etc.
Personality Traits
In terms of personality traits, PTSD-probable nurses appeared to score significantly higher on the BIS scale than their counterparts (t(96.79) = 2.81, P = 0.006). The BIS/BAS scale (Carver & White, 1994) was designed to measure the two opposing motivational systems; that is, motivation to move away from something unpleasant/aversive and motivation to approach something desirable, respectively. The higher BIS (but not BAS) in PTSD-probable nurses might indicate certain risk factors in individuals related to avoidance (as opposed to approach) motivation, leading to the type of actions they would take after experiencing traumatic and/or stressful situations.
Similar to the BIS/BAS results, PTSD-probable nurses scored significantly higher on both the negative (t(99.73) = 2.98, P = 0.003) and positive (t(87.36) = 2.56, P = 0.012) urgency subscales of the short UPPS-P Impulsive Behavior Scale (Cyders et al., 2014). Both subscales were designed to measure individuals’ tendency to engage in risky behavior while experiencing extreme affect (i.e., positive affect for positive urgency and negative affect for negative urgency). The two groups did not differ on the other subscales that measured other impulsivity characteristics (e.g., tendency to act without thinking, inability to remain focused, and sensation seeking). In summary, the two groups of nurses appeared to be different on measures of the trait behavioral avoidance system as well as measures of positive/negative urgency aspects of trait impulsivity.
Research Question #2: Associations Between Nurse-Specific Trauma and Negative Outcomes
The second research question asked whether a higher level of nurse-specific trauma was associated with substance use (e.g., alcohol or drugs) as a coping strategy. To address this question, correlations between seven types of nurse-specific trauma and two measured negative outcomes (i.e., AUDIT and DAST-10) was performed. This analysis includes 71 nurses, which was a subset of participants that contributed responses to all of these variables of interest. The results show that “trauma from disasters” was significantly correlated with AUDIT scores (r = 0.268 [CI: −0.097,0.534], P = 0.024). Although the DAST-10 and AUDIT scores were significantly correlated with each other (r = 0.433 [CI: 0.222, 0.605], P < 0.001), none of the nurse-specific trauma variables were correlated with the DAST-10. Note that the overall level of alcohol/drug use in this sample was relatively low (see Table 4).

Note. AUDIT = Alcohol Use Disorder Identification Test; DAST-10 = Drug Abuse Screening Test-10; STSS = Secondary Traumatic Stress Scale. * p < 0.05.
Research Question #3: Relationships Between Nurse-Specific Trauma and Cognitive Control
The third research question inquired about the relationship between nurse-specific trauma and individual differences in cognitive control. Thus, two aspects of cognitive control were assessed, i.e., response inhibition and attention switching, using cognitive tasks. Correlations between the seven nurse-specific traumas and cognitive control task variables were then conducted. However, to ensure that these task variables were reasonable for other across-subject correlational analyses, t-tests were performed between conditions to check for basic within-subject effects, such as whether “switch cost” was reliably greater than 0 and whether participants failed to stop due to responding too fast (i.e., failed-stop RT > go RT). These results were reported in Supplementary Materials.
Response Inhibition
Correlation Coefficients and 95% Confidence Intervals (Bonett & Wright, 2000; Fisher, 1992) Between Nurse Specific Trauma Variables and Cognitive Control Task Variables (N = 35).
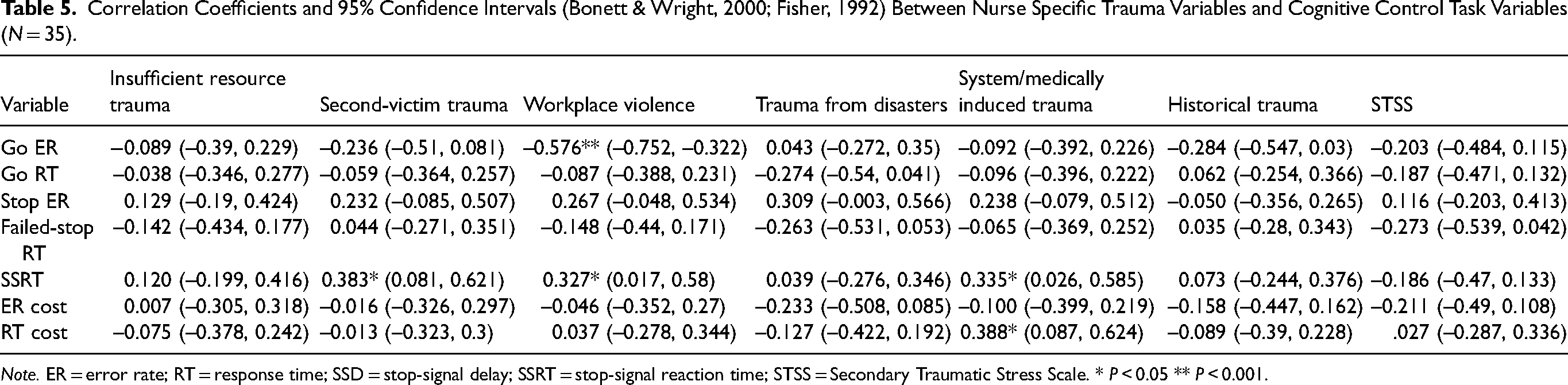
Note. ER = error rate; RT = response time; SSD = stop-signal delay; SSRT = stop-signal reaction time; STSS = Secondary Traumatic Stress Scale. * P < 0.05 ** P < 0.001.
Attention Switching
As for the rule-switching task used to assess attentions switching, RT switch cost was significantly correlated with system/medically induced trauma (r = 0.388 [CI: 0.087, 0.624], P = 0.013). Participants who reported a higher level of system/medically induced trauma exhibited a lower level of attention control. Among the seven types of traumas, system/medically induced trauma seemed to be the most sensitive to nurses’ individual differences in cognitive control task variables.
Discussion
The current study employed the middle-range theory of nurses’ psychological trauma (Foli, 2022) to stratify trauma experienced by nurses. The approach allowed for an analysis of the different nurse-specific types of traumas experienced at their workplace and the impact of trauma beyond the workplace. The analysis revealed that significantly higher amounts of trauma from disasters and system/medically induced trauma were associated with several negative psychological symptoms, including increased stress, anxiety, and depression. Furthermore, greater amounts of trauma from disasters appeared to be somewhat predictive of alcohol use. When looking at individual differences in cognitive control, the data showed that a high amount of second-victim trauma, workplace violence trauma, and system/medially induced trauma are associated with lower inhibitory control. System/medically induced trauma was the only type of trauma that was also correlated with cognitive control for task-switching. Together, these findings, though correlational, suggest that each type of trauma experienced by nurses at work is associated with unique consequences and should not be overlooked as one broad category.
One finding worth further elaboration was the differences in personality traits between PTSD-probable and PTSD-not-probable nurses. Specifically, PTSD-probable nurses were higher in trait BIS (but not in trait BAS) and trait positive/negative urgency (i.e., two aspects of impulsivity). The BIS versus BAS scale measures behavioral avoidance versus approach system, respectively, or how motivated an individual is to avoid negative outcomes versus approach positive outcomes (Carver & White, 1994). Positive/negative urgency measured in the short UPPS-P Impulsive Behavior Scale corresponds to the tendency to engage in rash action under extreme positive/negative affect (Cyders et al., 2014). Therefore, the higher scores in the PTSD-probable nurses indicated that these nurses might be more sensitive to aversive stimuli or outcomes and have a tendency to engage in unplanned actions that do not have specific goals (i.e., impulsive actions). This interpretation is consistent with a general hypothesis that the behavioral approach system drives goal-directed behavior and is associated with deliberate, planned actions (Amodio et al., 2008), whereas the behavioral avoidance system generates “reactions” to aversive stimuli, which often do not have specific goals (Threadgill & Gable, 2018). This finding also fits well with the experimental findings demonstrating that positive stimuli invigorates planned motor actions, while negative stimuli promote a lack of action or inappropriate ones (Chiu et al., 2014). It should also be noted that the finding of higher impulsivity in the PTSD-probable group was consistent with the correlation between system/medically induced trauma and cognitive control in the sub-sample. Future investigators could employ a larger sample to investigate how these variables (i.e., system/medically induced trauma, cognitive control, trait motivation, and trait impulsivity) relate to each other.
Another finding worth discussing was the difference between PTSD-probable and PTSD-not-probable nurses in terms of buffers. While they differed on the BRS, which measured how individuals perceived themselves as someone who can/cannot bounce back or recover from stress, they did not differ on the SPOS scale. The lack of difference in the SPOS scale might not be too surprising given that neither the insufficient resource trauma nor the workplace violence (which happened in the context of an organization or work environment) differed between the two nurse groups. This could be due to the method for group comparisons that was not sensitive enough to address the relationship between organizational support and the two organization/work environment-related traumas. Future studies could focus on directly comparing organizations with high versus low resources and support to evaluate the positive/negative impacts they may have on nurses’ physical and mental health. In contrast, the difference in resiliency is interesting, given that the PTSD-probable nurses also appeared to have more humankind traumas that had “happened to me.” This indicated that PTSD-probable nurses might have a history of personal trauma and unsuccessful experiences of bouncing back from those stressful events. It is therefore important for nurse leaders to acknowledge how nurses’ past trauma experiences could play a role in how they can handle stressors in their current practice. For example, a recent study (Labrague & De Los Santos, 2020) showed that social support, personal resilience, and organizational support together predicted anxiety specifically related to COVID-19 using Lee's (2020) COVID-19 five-item anxiety scale.
Strengths and Limitations
Although these findings are intriguing, it should be emphasized that the sample size was relatively small considering the extensive range of variables included in this investigation. However, it's important to note that this was a time-limited study conducted amidst the COVID-19 pandemic. The researchers faced constraints in planning and estimating the sample size due to the rapidly changing circumstances. Secondly, there was a lack of existing studies that could have served as a reference for an accurate sample size estimation. Thirdly, the study budget limitations restricted our ability to collect a larger dataset. Lastly, despite the relatively small sample size, it did yield meaningful results that can offer valuable insights for researchers in shaping future studies. For instance, based on these initial findings, it would be beneficial for future studies to replicate and/or customize the study design to gain a deeper understanding. Additionally, future studies could enhance participation by offering more flexible completion times. The current study required participants to finish the survey and tasks in one session, without considering that some individuals may need to return to complete it the following day or within a few days.
Regarding the issue of stressors, while the study did not identify differences in work-related characteristics (such as work hours per week or shifts worked) between nurses who were probable for PTSD and those who were not, it is important to recognize that the typical 12-hr shifts that nurses endure on a regular basis can be inherently stressful in their daily lives. This stress can be further compounded during a crisis like the COVID-19 pandemic. The pandemic serves as an opportunity for the nursing profession, prompting discussions about alternative strategies that could benefit both patients and nurses alike. In future studies, a sample that represents nurses who work 12-hr and 8-hr shifts with a focus on the nurse-specific traumas may illuminate differences and relationships between the length of shifts and traumas. This analysis would provide insights into the potential advantages and drawbacks associated with different shift durations. The profession of nursing must continue to provide wellness resources, adequate training in disaster-emergency preparedness, and psychological support to improve the physical and mental well-being of all nurses (Hofmeyer & Taylor, 2021).
Implications for Practice
The study results, though preliminary, have provided some insights into ways in which the work environment and support systems could be improved. The researchers, therefore, recommend future studies and/or nursing management to pay attention to various types of existing nurse-specific traumas and provide more targeted remediation and individualized support. The NPT framework would greatly benefit from a formal psychometric study that would enable its translation into a scale with established validity and reliability information. Conducting such a study would enhance the usefulness and applicability of the framework in assessing and measuring nursing-related traumatic experiences. A lesson taught by the COVID-19 pandemic is that nurse leaders and healthcare organizations might be able to build a healthy, resilient nursing workforce by investing in frontline nurses’ workplace safety and mental health. Engaging nurses by soliciting perceptions of mental health needs and fostering an environment that promotes psychological safety could be strategies to consider. Organizations could examine what types of nurse-specific traumas are avoidable and take steps toward reducing them, such as providing necessary staffing, supplies, and available non-nursing staff. Training and awareness of workplace violence enacted by patients and families could decrease such incidents. Debriefing after witnessing negative outcomes of medical interventions (system/medically induced trauma), verbal assaults (workplace violence), and medical errors (second-victim trauma) could also be ways to improve occupational health for nurses.
Conclusions
The current study is a work in progress. It investigated how various types of nurse-specific traumas contribute to nurses’ mental health. By stratifying traumas experienced by nurses, the study found trauma from disasters and system/medically likely induced trauma associated with increased stress, anxiety, and depression. Furthermore, experiencing “trauma from disaster” might lead to subsequent alcohol use. Lastly, second-victim trauma, workplace violence trauma, and system/medially induced trauma may be associated with lower inhibitory control. However, it is crucial to emphasize that the findings presented in this study are preliminary in nature. While they offer valuable insights into the topic at hand, it is essential to recognize that further research with larger sample sizes is required to conduct a more comprehensive and in-depth investigation. Future studies should consider a thorough examination of the study's assumptions (e.g., adopting the NPT framework) and the testing of hypothesized relationships in a more rigorous and robust manner. Given the global nursing shortage, nursing leaders and healthcare administrators should start treating nurse-specific traumas as an occupational health and safety issue and take steps to improve the current conditions.
Supplemental Material
sj-docx-1-son-10.1177_23779608231214601 - Supplemental material for Nurses’ Psychological Trauma and Cognitive Control in the COVID-19 Pandemic
Supplemental material, sj-docx-1-son-10.1177_23779608231214601 for Nurses’ Psychological Trauma and Cognitive Control in the COVID-19 Pandemic by Chiu Yu-Chin, Anna K. Forster, Lingsong Zhang and Karen J. Foli in SAGE Open Nursing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Health and Human Sciences (HHS) COVID-19 Rapid Response Grant Program sponsored by Purdue University College of Health and Human Sciences, West Lafayette campus.
Author Contributions
All authors have agreed on the final version and meet at least one of the following criteria: (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data and (2) drafting the article or revising it critically for important intellectual content.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.