
Abstract
Introduction
The prevalence of cesarean sections (CSs) in both industrialized and developing nations is a significant issue for public health officials, particularly in light of the knowledge of their socioeconomic underlying determinants.
Objective
To ascertain the prevalence of CS delivery among nurses, their predictors, and the effect it has on exclusive breastfeeding practice in Tamale, Ghana.
Methods
This study used a quantitative technique and an analytical cross-sectional design. Data analysis was done using Statistical Package for the Social Sciences, and variable associations and predictions were identified using chi-square and logistics regression analysis.
Results
There were 326 fully completed and returned questionnaires; the majority (40.0%) of respondents were registered general nurses (RGN). The majority of respondents (56.0%) were between the ages of 31 and 40. The prevalence rate of CS delivery was 21.1%. Predictor variables were; Community health nurses/RGN (adjusted odds ratio [AOR] = 3.7, 95% confidence interval [CI] = 1.2–11.0), and second degree/first degree level of educational attainment (AOR = 36.0, 95% CI = 2.4–528.9). The effects of CS delivery on exclusive breastfeeding were; low confidence to exclusively breastfeed, opting to combine both breastfeeding and artificial feeding, and less likely to practice exclusive breastfeeding.
Conclusion
Even though CSs and exclusive breastfeeding practices are both problems facing nurses, CSs seem to compound the problem of exclusive breastfeeding among nurses.
Introduction
Cesarean section (CS) delivery is the process of childbirth by an incision made through the abdominal wall into the uterus in a safe medically acceptable environment. And this is usually done when a vaginal delivery is unsafe or impractical, or when the safety of the unborn child is in jeopardy (Cleveland Clinic, 2022). Big baby (fetal macrosomia), pregnancy-induced hypertension, maternal weight, labor dystocia, and multiple gestations are examples of conditions that may necessitate a CS in clinical practice (Sung & Mahdy, 2023).
Review of Literature
Developed countries have high rates of CS delivery, including 25.9% in China, 32.3% in Australia/New Zealand, and 45.9% in Brazil (Betrán et al., 2016). And in Africa, the prevalence differs among the countries: Uganda (7.0% in 2022), Rwanda (15.6% in 2020), and Nigeria (2.1%) (Adewuyi et al., 2019; Nakinobe et al., 2022; Kibe et al., 2022). In Ghana, a recent national study by Alhassan reported the prevalence to be 15.7%, which is higher as compared to 11.4% in an earlier study by Dankwa et al. (Alhassan, 2022; Dankwah et al., 2019).
Cesarean sections are linked to a variety of maternal and fetal variables. According to a study conducted in Nigeria, socioeconomic characteristics such mother's age, place of residence, weight, prenatal attendance, parity, mother's religion, infant size, and maternal health insurance coverage are all associated with CS delivery (Adewuyi et al., 2019). Also, in Ghana, the predictor factors identified were age, residence type, infant weight, and wealth status (Alhassan, 2022). Additionally, a study on socioeconomic disparities in Ghana concerning CS found a significant correlation between maternal age, parity, education, and wealth quintile. The study also showed that poorer women are unable to receive CS delivery due to indirect costs and/or other factors (Dankwah et al., 2019). Another study in Ghana's northern region also found a link between fetal weight and the likelihood of a cesarean delivery; among pregnant women with a fetal weight of 4 kg or more, the likelihood of a cesarean delivery was raised. The likelihood of a CS delivery was the same for pregnant women who had more than three prenatal consultations (Apanga & Awoonor-Williams, 2018).
Complication chances are somewhat higher with CS deliveries than with vaginal deliveries. These might include infection, hemorrhage, embolism from a blood clot, bowel or bladder injury, anesthesia risk, and fetal injury (Cleveland Clinic, 2022). Women's recovery may turn out to be slower with CS delivery as compared to recovery from vaginal delivery; CS delivery is likely to cause chronic pelvic pain in the woman (Cleveland Clinic, 2022). With the babies, some of the complications associated with CS deliveries are breastfeeding problems and the risk of breathing issues (Cleveland Clinic, 2022). In a study done in Turkey, after adjusting for sociodemographic and delivery-related characteristics, women who underwent CSs had a greater risk of the delayed beginning of breastfeeding and nonexclusive breastfeeding in the three days following birth (Paksoy Erbaydar & Erbaydar, 2020). Delayed breastfeeding and nonexclusive breastfeeding had standardized rate ratios of 1.428 (95% confidence interval [CI]: 1.212–1.683) and 1.468 (95% CI: 1.236–1.762), respectively (Paksoy Erbaydar & Erbaydar, 2020). The early commencement of breastfeeding was negatively impacted by CSs in sub-Saharan Africa (Yisma et al., 2019).
Currently, nonemergent CS deliveries are performed far too frequently. The majority of study on CS overuse emphasizes the role of the physician, areas with a high incidence, hospital policy, and the purpose of the CS (Alhassan, 2022; Adewuyi et al., 2019; Dankwah et al., 2019; Apanga & Awoonor-Williams, 2018). Nurses spend the most time with patients and play a very important role in deciding the need for a patient to go for CS delivery. Understanding how the nurse may assist in avoiding needless CS treatments is crucial because she is the patient's principal advocate. Meanwhile, little study has been done to unveil their personal experience with CS delivery. Also, the low practice of exclusive breastfeeding practice has been established to be compounded by CS delivery (Paksoy Erbaydar & Erbaydar, 2020; Yisma et al., 2019). So there is a need to further assess the impact of CS delivery on exclusive breastfeeding among nurses since the prevalence (66.0%) of exclusive breastfeeding practice among nurses is not encouraging in Tamale (Iddi et al., 2020). This current study therefore seeks to ascertain the prevalence of CS delivery among nurses, their predictors, and the effect it has on exclusive breastfeeding practice in Tamale of Ghana.
Methods
Study Design
This study used a quantitative technique and an analytical cross-sectional design. A semistructured questionnaire was used to gather the information. The questionnaire was developed in line with the goals of the study and was based on existing literature (Iddi et al., 2020). The questionnaire consisted of two sections. Section A for the demographic characteristics of the study participants and section B for respondent obstetric and breastfeeding history for recent birth. English was used for the research. The questionnaire was pretested on 40 nurses and midwives at the Savelugu Municipal Hospital before the real data were collected, but they were excluded from the final data analysis. Later, the instrument was self-administered under the close supervision of data gatherers. Each participant's data collection process took roughly 8 minutes, and the full exercise ran for three weeks. Validity and completeness checks were performed on each returned questionnaire.
Research Question
What is the prevalence of CS delivery among nurses in Tamale, Ghana?
What socioeconomic factors predict CS delivery among nurses in Tamale, Ghana?
What is the effect of CS delivery on exclusive breastfeeding practice among nurses in Tamale, Ghana?
Study Setting
The four hospitals used for the experiment were selected by deliberate sampling. The idea behind choosing these hospitals was that they had a larger percentage of female nurses and midwives. They were: Tamale Teaching Hospital, Tamale Central Hospital, Tamale West Hospital, and Tamale Seventh-Day Adventist Hospital participated in the study. These are the four main hospitals in the Tamale Metropolis. Tamale Teaching Hospital serves as a referral Center for the five Regions in the Northern part of the country and the neighboring countries. West Hospital Tamale and Tamale Central Hospital are secondary levels for care. Each of the hospitals provides neonatal and maternal care that supports the study objectives.
Inclusion/Exclusion Criteria
This study population included general nurses and midwives, psychiatric nurses, community health nurses, health assistant clinicians, and specialist nurses. Female nurses and midwives with children ages 0–24 months and consent to participate were recruited from the four major public hospitals in Tamale. Students or nurses on rotation were excluded from the study. Also, nurses on long leave including study or maternity leave were excluded.
Sample Size and Sampling
Using 66.0% prevalence (Iddi et al., 2020), the sample size for this study was arrived at using the Cochran formula:

Ethical Considerations
The Kwame Nkrumah University of Science and Technology's ethics committee extended its support (ref. CHRPE/AP/042/21). The participating hospitals and the regional health directorate also gave their administrative clearance. All participants gave written informed consent to participate in this study. Participation was voluntary and anonymous; their psychological and physical health was taken into account throughout the study.
Data Analysis
Data entry and cleaning were done using Microsoft Office Excel and later converted to Statistical Package for the Social Sciences (SPSS) SAV file analysis. Responses to categorical variables were coded to allow for quantitative analysis. The data analysis was done using SPSS version 20. The descriptive analysis was done using frequencies with percentages. Chi-square analysis was used for significant association between participants’ sociodemographic characteristics and CS delivery. Variables with statistical significance at the chi-square analysis were further modeled in binary multiple logistics analysis for predictors of CS delivery. Meanwhile, univariate logistics regression was used to establish a relationship between CS delivery and exclusive breastfeeding variables; preferred baby feeding option, confidence to exclusively breastfeed after delivery, and exclusive breastfeeding practice. The level of significance for this study was set at 95%.
Results
Characteristics of the Study Participants
There were 326 fully completed and returned questionnaires; the majority (40.0%) of respondents were registered general nurses (RGN), while nursing specialists made up the least (0.6%) of the participating categories of nurses. In terms of educational attainment, diploma holders made up the most (43.7%) while second-degree holders made up the least (1.2%). The majority of respondents (56.0%) were between the ages of 31 and 40, and the majority (53.5%) had monthly incomes between 1000 and 2000 Ghana cedis. Also, the majority of the study participants (92.8%) were married. Again, the majority (56.1%) identified as Muslim, and most (45.8%) were identified as Dagombas. Finally, the majority of respondents (69.1%) reported living in nuclear families (Table 1).
Characteristics of the Study Participants.

Participants’ Response to Exclusive Breastfeeding Variable and Mode Delivery
The majority (98.8%) of the study participants indicated that after the birth of their baby, they were confident to exclusively breastfeed. The preferred feeding option by most (77.7%) of the study participants was exclusive breastfeeding only, then breastfeeding and artificial feeding (21.3%). A significant proportion (14.8%) of the study participants did not practice exclusive breastfeeding for six months. A significant (21.1%) number of them had their mode of recent delivery by CS, representing a prevalence rate of 21.1% (Table 2).
Participants’ Response to Exclusive Breastfeeding Variables and Mode of Delivery.

Socioeconomic Predictor Factors of CS Deliveries Among Nurses
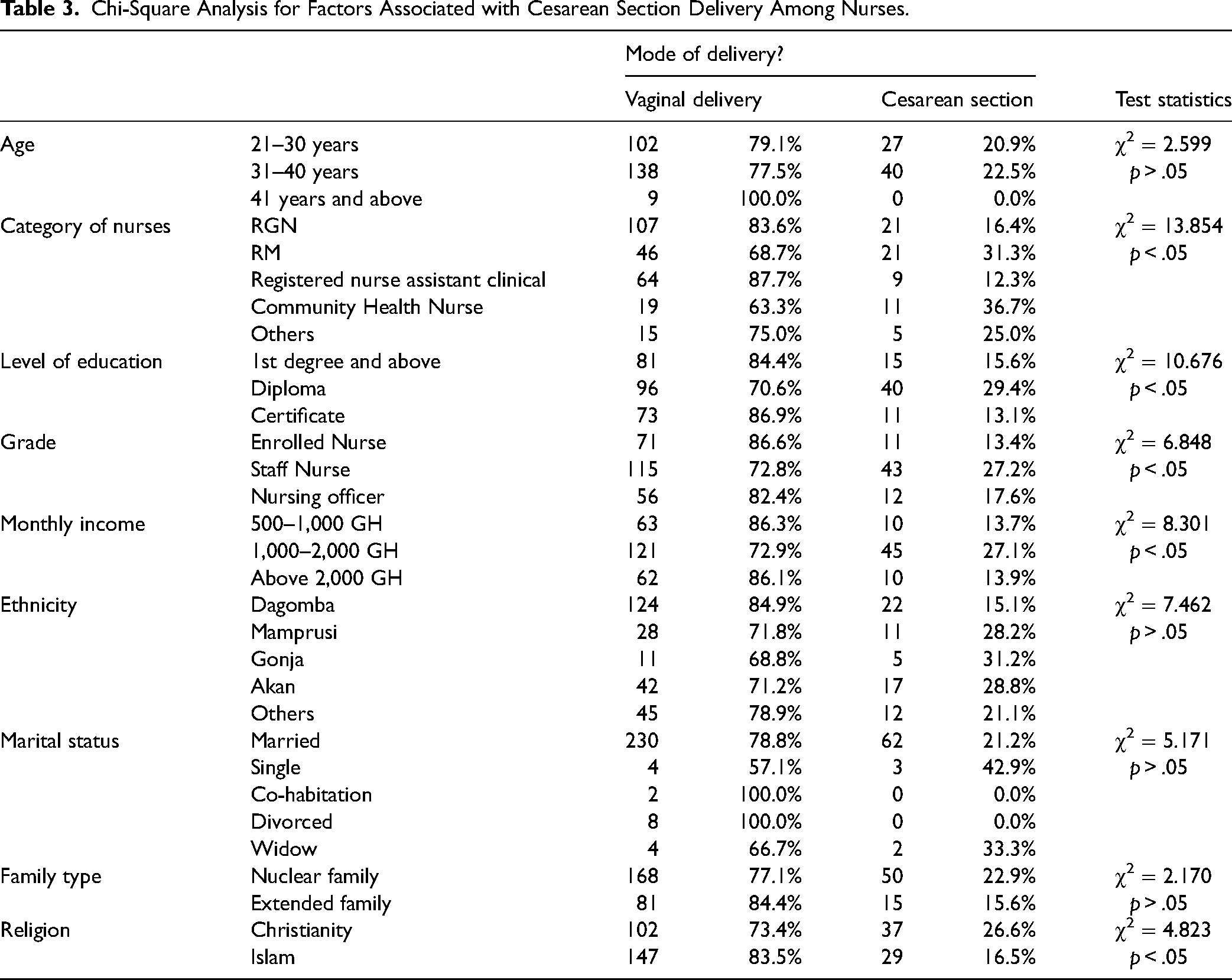
From the chi-square analysis, participants’ characteristics such as nursing category, level of education, grade, monthly income, and religion were significantly associated with their mode of delivery (p < .05) (Table 3). These variables were further modeled with binary logistics regression for predictor factors of CS deliveries among nurses. The model indicated that the category of nursing the people belong to predicts their mode of child delivery. Community health nurses were 2.7 times more likely to have CS delivery when compared to RGN nurses (adjusted odds ratio [AOR] = 3.7, 95% CI = 1.2–11.0). Also, from the model participant level of educational attainment predicted CS as a mode of delivery among nurses. Those with 2nd-degree level of education were 35.0 times more likely to have CS delivery when compared to those with 1st-degree level of educational attainment (AOR = 36.0, 95% CI = 2.4–528.9) (Table 4).
Chi-Square Analysis for Factors Associated with Cesarean Section Delivery Among Nurses.
Binary Logistics Regression for Predictor Factors Cesarean Section Delivery Among Nurses.

The model predicted for cesarean section delivery.
Effect of Mode Delivery on Exclusive Breastfeeding Among Nurses
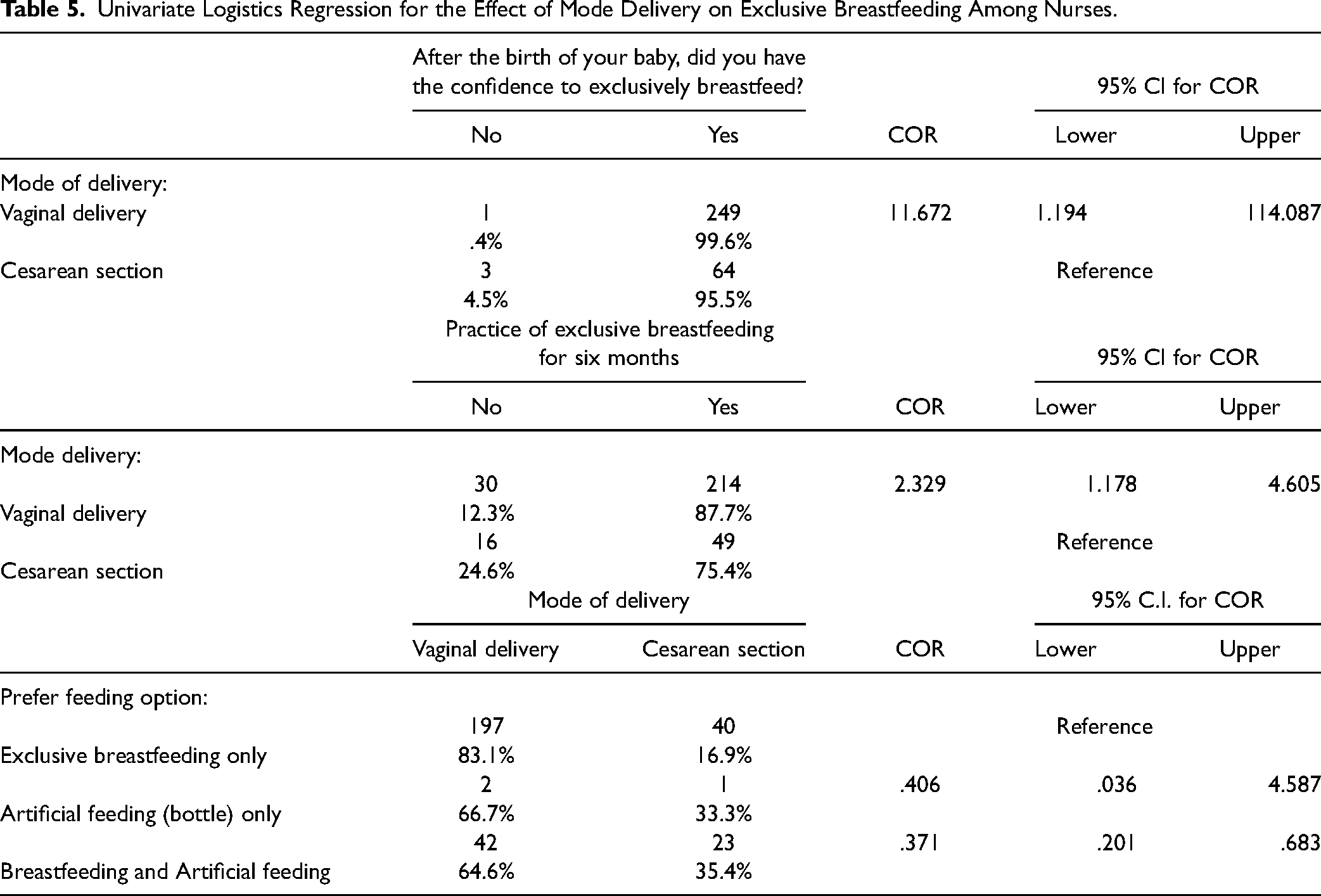
To assess the effects of CS delivery on exclusive breastfeeding, univariate logistics regression analysis was done. After the birth of a baby, nurses with vaginal delivery were 10.7 times more likely to have the confidence to exclusively breastfeed when compared to nurses with CS delivery (odds ratio [OR] = 11.7, 95% CI = 1.2–114.1). Also, nurses with vaginal delivery methods were 0.63 times less likely to opt for breastfeeding and artificial feeding for their babies than exclusive breastfeeding only as compared to nurses with CS delivery (OR = 0.37, 95% CI = 0.20–0.68). Finally, the method of child delivery predicted the practice of exclusive breastfeeding. Nurses with vaginal delivery methods were 1.3 times more likely to practice exclusive breastfeeding as compared to those with CS deliveries (OR = 2.3, 95% CI = 1.2–4.6) (Table 5).
Univariate Logistics Regression for the Effect of Mode Delivery on Exclusive Breastfeeding Among Nurses.
Discussion
Compared to vaginal deliveries, CS deliveries have a slightly higher risk of complications. These include the potential for fetal harm, infection, hemorrhage, blood clot embolism, bowel or bladder injury, and anesthesia risk (Cleveland Clinic, 2022). Nurses spend the most time with patients and play a very important role in promoting safe vaginal delivery as much as possible because of the fewer complications associated with it. Yet in this present study, the prevalence of CS delivery among nurses in Tamale was 21.1%. And this is higher compared to 15.7% of the Ghanaian general population (Alhassan, 2022). And this is even higher compared to results from other African countries (Adewuyi et al., 2019; Nakinobe et al., 2022; Kibe et al., 2022). However, this is low compared with results from developed countries including 25.9% in China, 32.3% in Australia/New Zealand, and 45.9% in Brazil (Betrán et al., 2016).
This study realized that the category of nursing the person belongs to predict their mode of child delivery. Community health nurses were 2.7 times more likely to have CS delivery when compared to RGN. In daily practice, community health nurses work to advance health while also maintaining a certain level of balance in illness prevention, early disease identification, and care evaluation while RGN focus on the treatment and care of the sick and on restoring the individual's balance toward health (Mona, 2016). So it is expected that community health nurses who are focused on prevention could do their best to prevent themselves from CS delivery. Meanwhile, the outcome for the RGN can be explained by the health belief model that a person's belief in a threat of an illness or disease together with a person's belief in the effectiveness of the recommended health behavior will predict the likelihood the person will adopt that behavior (Rosenstock, 1974). In the study setting, the RGN are involved with CS patients from the operation room to the recovery room till discharge and stand the chance to notice what the suffering patients go through after CS as compared to community health nurses.
Also, the participant's level of educational attainment predicted CS as a mode of delivery among nurses. Those with 2nd-degree level of education were 35.0 times more likely to have CS delivery when compared to those with 1st-degree level of educational attainment. This is consistent with a meta-analysis study done for Sub-Saharan Africa, which has a higher likelihood of CS deliveries for women with higher than those with lower education (Islam et al., 2022). Also, consistent with another Sub-Saharan study involving 34 datasets from different countries reported the same (Arendt et al., 2018). Some earlier studies reported reasons for the higher odds of CS deliveries among the more educated women to be that is less painful than a vaginal delivery, it is safer, less disruptive to their professional and personal lives, and more prestigious in society (Azami-Aghdash et al., 2014; Nababan et al., 2018). Maybe that explains why higher income status predicted CS deliveries even in Ghana (Alhassan, 2022; Manyeh et al., 2018). Although in this study results respondents’ income level and occupational grade did not predict CS deliveries but there were significant associations at the bivariate analysis stage.
The CS does not put only the mother at a disadvantage but also the baby, one of the complications associated with CS deliveries is breastfeeding (Cleveland Clinic, 2022). In this current study, after the birth of a baby, nurses with vaginal delivery were 10.7 times more likely to have the confidence to exclusively breastfeed when compared to nurses with CS delivery. Also in a study of 33 Sub-Saharan African countries, early commencement of breastfeeding was less likely among women with CS deliveries (Yisma et al., 2019). Again in this present study, nurses with vaginal delivery methods were 0.63 times less likely to opt for additional artificial feeding for their babies than exclusive breastfeeding only. They were 1.3 times more likely to practice exclusive breastfeeding as compared to those with CS deliveries. Also in a study that was done in Turkey women who underwent CSs had a greater risk of the delayed beginning of breastfeeding and nonexclusive breastfeeding. Delayed breastfeeding and nonexclusive breastfeeding had standardized rate ratios of 1.428 (95% CI: 1.212–1.683) and 1.468 (95% CI: 1.236–1.762), respectively (Paksoy Erbaydar & Erbaydar, 2020).
According to studies, breastfeeding advantages are dose-dependent, meaning that as nursing time increases, so do the benefits to the infant's health (Krol & Grossmann, 2018; WHO, 2021). Given that breastfeeding has been shown to have numerous long-term advantages for both mothers and babies, it is crucial to comprehend how cesarean-section deliveries affect both the start and continuation of breastfeeding.
This study is not without limitation as the study data were deprived of the distinction between emergency and elective CS deliveries, and the medical reasons why they were done. Also, the study was limited to providing information on whether there were complications associated with the CS deliveries and how they impacted exclusive breastfeeding. Finally, this study did not assess how CS delivery impacted their nursing practice.
Conclusion
The prevalence of CSs among the studied nurses was high with most odds of it among community health nurses and those with higher educational attainment. Cesarean section deliveries showed a negative impact on child breastfeeding. This is because cesarean-section delivery can lead to complications that make it difficult for mothers to breastfeed, such as pain, fatigue, and difficulty bonding with the baby (Moore et al., 2012).
Recommendation
In Ghana to achieve the full six months of exclusive breastfeeding among employed workers, especially healthcare workers including nurses, their maternity leave should be expanded from the current three months to six months. Further studies are recommended to examine why CS deliveries are among community health nurses as compared to RGN.
Footnotes
Acknowledgment
A deep sense of gratitude and sincere appreciation goes to all participants involved in the research.
Data Availability
This study data are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The Kwame Nkrumah University of Science and Technology's ethics committee extended its support (ref. CHRPE/AP/042/21). The participating hospitals and the regional health directorate also gave their administrative clearance. Following a thorough explanation of the study, participants’ informed consent was requested.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The cost of data analysis was sponsored by the Ghana Organization for Maternal and Child Health (GOMaCH).