
Abstract
Introduction
Operative vaginal deliveries are a method of dealing with issues that arise during the second stage of labor with the use of vacuum device or forceps. The decision to use an instrument to deliver the fetus weighs the maternal, fetal, and neonatal consequences of the procedure against the alternative option of cesarean birth. However, evidence on operative vaginal delivery is limited in Ethiopia in general and in the study area in particular.
Objectives
This study aimed to assess the magnitude, indications, and factors associated with operative vaginal delivery among mothers who gave birth at Adama Hospital Medical College, Ethiopia.
Methods
A facility-based cross-sectional study was conducted among a sample of 440 mothers who gave birth from 1 to 30 June 2022. A systematic random sampling technique was used to select the study participants. Data were collected using an interviewer-administered structured questionnaire. The data were entered into EPI INFO version 7 and exported to SPSS version 25 for analysis. Bivariate logistic regression analysis was used to identify candidate variables at p < .25 and multivariable logistic regression analysis was used to identify the independent predictors of operative vaginal delivery at p < .05 with 95% confidence intervals (CIs).
Results
The magnitude of operative vaginal delivery was 14.8% (95% CI: 10.8, 18.8). Rural residence (adjusted odds ratio (AOR), 2.09; 95% CI: 2.01, 7.41), maternal age 25–34 (AOR, 4.95; 95% CI: 1.62, 9.2), being primigravida (AOR: 3.5, 95% CI: 1.26, 9.98), gestational age ≥42 weeks (3.09; 95% CI: 1.38, 6.9), and antenatal care (ANC) follow-ups <4 times (AOR:3.9; 95% CI: 1.09, 9.45) were significantly associated with operative vaginal delivery.
Conclusion
The magnitude of operative vaginal delivery in the study area was relatively low. Rural residence, maternal age 25 to 34, primigravida, gestational age ≥42 weeks, and ANC follow-ups <4 times were independent determinants of operative vaginal delivery. Thus, health education programs and other multidisciplinary strategies are required to encourage mothers to have regular ANC follow-ups.
Introduction
Operative vaginal delivery (OVD) is an important component of obstetric care, which refers to the use of forceps or a vacuum device to avoid poor birth outcomes and reduce the primary cesarean-section rate (Ali & Norwitz, 2009; Ogunwale et al., 2016). It is carried out by skilled health workers to reduce maternal and neonatal complications (No, 2011). Although OVDs were used as an alternative mode of delivery for centuries, recent trends indicate that OVDs use has reduced as the cesarean delivery rate has risen (Johanson & Menon, 1999; Merriam et al., 2017; Sydsjö et al., 2010). In Ethiopia, the prevalence of OVD ranged from 2.10% to 27.90% among mothers who gave birth (Abdo et al., 2020; Yemaneh et al., 2017).
OVD is recommended in any situation where the mother or fetus could be harmed (Berhan & Abdela, 2004). In the setting of indications such as the second stage of labor being extended, having severe preeclampsia or eclampsia, having labor progress slowly due to maternal weariness or exhaustion, or choosing to shorten the second stage of labor are all examples of maternal indications for OVD. Fetal distress and a fetal heart rate that is unsettling are two of the main fetal indicators of OVD (Alegbeleye et al., 2018; Sjödin et al., 2018).
In OVD applications, the operator must be familiar with the indications, contraindications, application, and use of the specific device to minimize fetal and maternal difficulties. OVDs can cause minor maternal complications, including laceration of the vagina and perineum, as well as major complications, such as traumatic hemorrhage, bladder injury, and pelvic muscle injury, if not done by skilled healthcare practitioners (Biru et al., 2019). A low Apgar score is the most common neonatal complication. Yet, OVDs have the potential to lessen both immediate and long-term second-stage cesarean section complications if they are performed by qualified personnel. Moreover, OVDs have the potential to reduce the healthcare costs related to cesarean sections (CSs; Bailey et al., 2017; Vannevel et al., 2019). However, the problem of declining instrumental use was exacerbated by a decline in the number of physicians with the required skills and training to undertake these procedures, along with the fear of litigation (Bailey, 2005). In Ethiopia, to enhance the knowledge and experience of healthcare professionals, operational vaginal birth is being taught as part of basic emergency obstetric management (Sewunet et al., 2022).
Review of Literature
Globally, 10% to 20% of all deliveries require some kind of intervention at the time of delivery, and 6% to 12% of these interventions involve OVDs (Lamichhane, 2018; Yeshialem et al., 2019). The global incidence of OVD rates varies greatly between 1% and 15% (Dutywa et al., 2022). In developed countries, the rates vary: from 10% to 15% in the United Kingdom to around 4.5% in the United States of America where the rate has halved in the last 20 years (Vannevel et al., 2019); lower rates are observed in low- and middle-income countries such as South Africa (1% to 3%; Dutywa et al., 2022), and Nigeria (3.6%; Vannevel et al., 2019). These studies indicated that there is a trend toward fewer instrumental deliveries, which is of great worry to the global healthcare system (Sonawane et al., 2021). In developing countries such as Ethiopia, there is a scarcity of evidence demonstrating the magnitude and factors associated with OVD (Shimalis et al., 2022). To lower the rate of CSs and the issues they cause; it would be helpful to evaluate the magnitude of instrumental births and their key indicators. Thus, this study aimed to assess the magnitude, indications, and associated factors of OVD among mothers who gave birth at Adama Hospital Medical College (AHMC), in Ethiopia, 2022
Methods
Design
An institution-based cross-sectional study was conducted from June 1 to 30, 2022, at AHMC found in Adama town. Adama town is located approximately 99 km Southeast of the capital, Addis Ababa. According to the Ethiopian Central statistical agency's 2007 census figures, there are approximately 86,069 women of reproductive age out of a total female population of 192,518 (Population & Commission, 2008).
As per AHMC's annual report for 2021, there were 15,951 documented deliveries, with 1,122 (7.03%) of been induced and the rest 14,829 (92.97%) being spontaneous labor. In terms of method of delivery, a large percentage of deliveries, 11,510 (70.5%), were vaginal, preceded by cesarean section (3836; 23.5%), and assisted instrumental delivery (978; 6%; Authority, 2001).
Research Questions
What is the magnitude of OVD among mothers who gave birth at AHMC, Ethiopia?
What are the indications for OVD among mothers who gave birth at AHMC, Ethiopia?
What are the factors that are associated with OVD among mothers who gave birth at AHMC, Ethiopia?
Sample
The sample size for this study was determined by using the single population proportion formula by considering the following assumptions. The proportion of OVD (p = 10.3%) that was taken from a previous study conducted among mothers who gave birth at Jimma University Medical Center (Hubena et al., 2018), a 95% confidence level (CI; Z = 1.96), 3% margin of error (d = 0.03), and by adding 10% for nonresponse rate, the final sample size of the study was 440.
According to the preassessment, the two-month average total deliveries obtained from the hospital's delivery and discharge registration logbooks revealed that there were 1,300 total deliveries. Based on the above information, after K was calculated, the study subjects were selected using a systematic random sampling technique. To determine the sampling fraction, the total number of deliveries was divided by the total sample size of 440, which were approximately 3. Then the lottery method was used to choose a random number from the numbers 1 up to 3. As a result, the selected number was 2, and this number was the first study participant to be included in the sample; their card was then reviewed, as well as every third mother was recruited in the sample until the total sample size of 440 for this study was obtained.
Inclusion/Exclusion Criteria
All mothers who gave birth at AHMC were the source population (which included both normal and assisted vaginal deliveries), and all selected mothers who gave birth at AHMC during the study period were the study population. Mothers who gave birth during the data collection period and agreed to participate in the study were included in the study, whereas those who gave birth with CS, were critically ill, and were unable to communicate during the data collection period were excluded.
Data Collection
A data collection tool was developed after reviewing different literature (Gei, 2012; No, 2011). A structured interviewer-administered questionnaire that includes sociodemographic factors (age, residence, occupation, religion, educational status, marital status, and monthly income) was used to interview mothers at the exit. The interview was conducted at the exit and the objective and benefit of the study were described for every participant and written informed consent was obtained to assure their choice of participation or refusal.
The questionnaire was initially prepared in English and then translated into Afaan Oromo and Amharic languages before being returned to English to keep the consistency of the tool. A checklist was used to extract data from patient charts, such as the mothers’ and their neonates’ charts, labor ward reporting logbooks, and instrumental delivery formats. The first part required information about the patient's gravidity, parity, history of stillbirth, antenatal care (ANC) follow-up, number of ANC follow-ups, and gestational age. The second part required the parameters of labor which were nonreassuring fetal heart rate (NRFHR), prolonged second stage of labor (PSSOL), poor maternal exertions fetal distress, and maternal blood pressure. One supervisor and three BSc midwives were trained on how to interview eligible mothers and abstract information from respective charts.
Variables
Dependent Variable
Operative vaginal delivery.
Independent Variables
Operational Definitions
Data Quality Assurance
From tool development to result analysis, data quality was monitored closely. For two days, the principal investigator trained data collectors and supervisors on sampling methods, interview techniques, as well as the data collection process, and the overall objective of the study.
To ensure the quality and consistency of the checklist and the questionnaire with the objective of the study, a pretest was done on 5% of the total sample size at Bishoftu General Hospital, which was not selected for the study. Questions that were identified to be unclear or understandable were modified accordingly. Completeness and logical consistency were checked during data collection in a setting with close day-to-day supervision.
Statistical Analysis
Following manual verification of data completeness, data were coded, entered, and cleaned by EPI INFO version 7 before exporting to SPSS version 25 for statistical analysis. The Shapiro–Wilk test was used to assess the normality of continuous variables. A descriptive statistical analysis was carried out using frequency, percentage, median, interquartile range, mean, and standard deviation (SD). To identify factors that are associated with OVD, both bivariate and multivariable binary logistic regression analyses were executed, and the variables in bivariate analysis with p-values < .25 were fitted to the final multivariable binary logistic regression analysis, and to identify the determinant factors of OVD among mothers. To assess the fit of the model, Hosmer and Lemeshow's goodness of fit test was used with a p-value of .05. Variation inflation factor (VIF) was used to determine the presence of multicollinearity, with VIF > 5 indicating the presence of multicollinearity. Variables with p-values of .05 were considered statistically significant in the final model, and an adjusted odds ratio (AOR) of 95% CI was used to assess the strength of the association. Finally, the findings were presented through narrations, tables, and graphs.
Results
Sociodemographic Characteristics of Participants
A total of 440 mothers participated in this study making a response rate of 100%. The mean (±SD) age of participants was 27.61 (±4.68) years and the majority, (n = 286/440, 65%) of them were in the age group of 25 to 34 years. The majority of the study participants were Orthodox Christians, at (n = 215/440, 48.9%). With regard to their marital status, (n = 357/440, 81.1%) were married, and more than half (n = 261/440, 59.3.9%) of the participants attended elementary school. The median monthly income of the respondents was US$34 (US$20–US$40; Table 1).
Sociodemographic Characteristics of Mothers Who Gave Birth at AHMC, Ethiopia 2022 (n = 440).
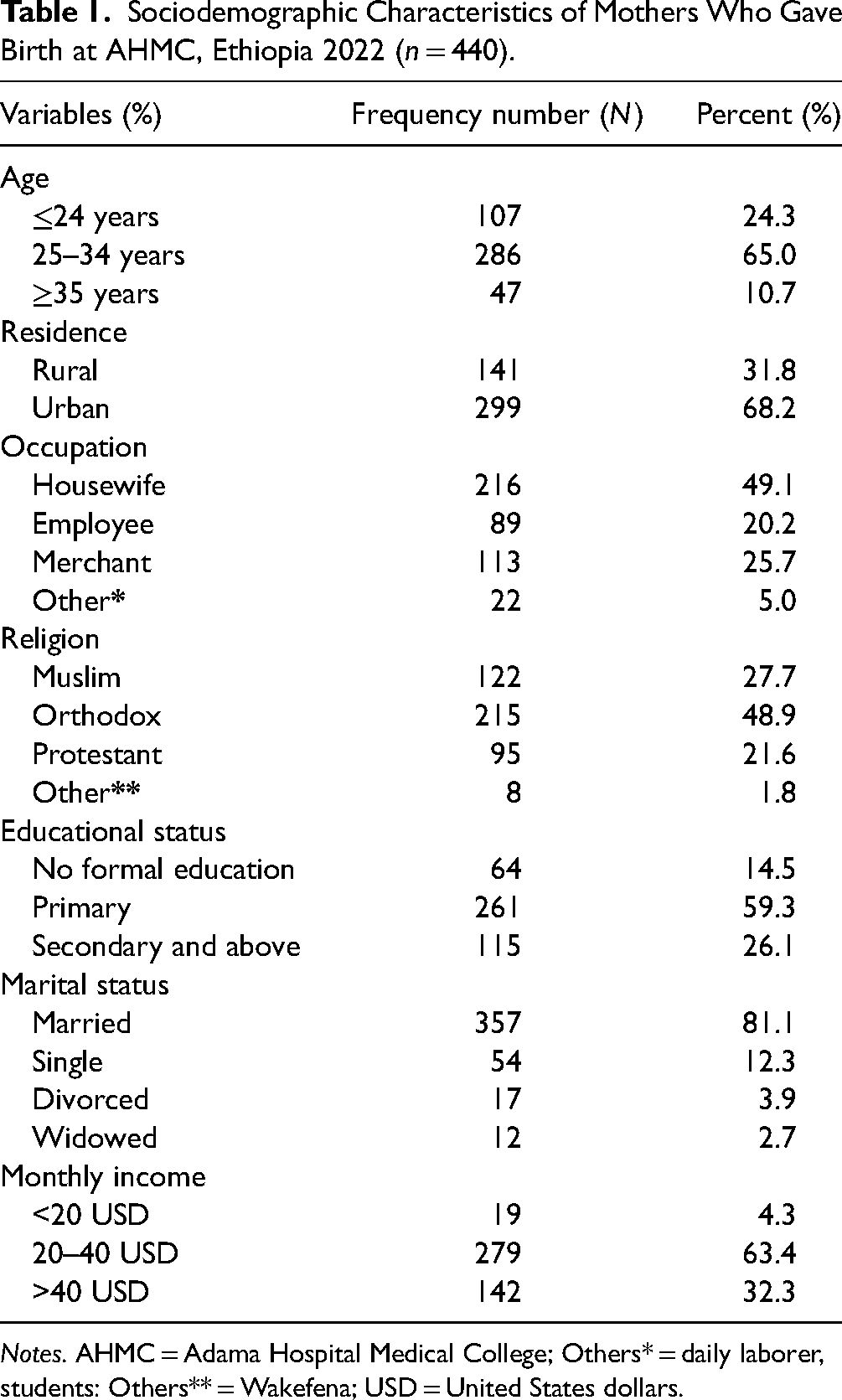
Notes. AHMC = Adama Hospital Medical College; Others* = daily laborer, students: Others** = Wakefena; USD = United States dollars.
Obstetric-Related Information
Nearly two-thirds (n = 298, 67.7%) of mothers were multigravida, and (n = 421/440, 95.7%) had at least one ANC visit. In terms of the previous history of stillbirth, (n = 424/440, 96.4%) did not have a stillbirth. Of the total, (n = 364/440, 82.7%) women had a gestational age between 37 and 41 weeks, and 280 (n = 280/440, 63.6%) of them were multipara (Table 2).
Obstetric-Related Characteristics of Mothers Who Gave Birth at AHMC, Ethiopia, 2022 (n = 440).

Notes. AHMC = Adama Hospital Medical College; ANC = antenatal care.
Research Question Results
Magnitude of Operative Vaginal Delivery
The overall magnitude of OVD was (n = 65/440, 14.8%; 95% CI: 10.8, 18.8), in a separate analysis, vacuum-assisted delivery accounted for (n = 43/65, 66.2%), and forceps (n = 22/65, 33.8%), with a ratio of vacuum to forceps: 2:1 (Figure 1).

Magnitude of operative vaginal delivery among mothers who gave birth at Adama Hospital Medical College (AHMC), Ethiopia, 2022 (n = 440).
Clinical Indication for Operative Vaginal Delivery
Sixty-three (96.9%) of the operative vaginal deliveries were emergency procedures and (n = 2/65, 3.1%) were elective/planned. The delayed second stage of labor, 35 (53.8%) was the most common indication for OVD followed by fetal distress (n = 18/65, 27.7%) and severe preeclampsia/eclampsia (n = 9/65, 13.8%). The majority of (n = 64/65, 98.5%) of the procedures were successful (Figure 2).

Indications for operative vaginal delivery among mothers who gave birth at Adama Hospital Medical College (AHMC), Ethiopia, 2022 (n = 65).
Factors Associated with Operative Vaginal Delivery
In bivariate logistic regression analysis variables such as residence, maternal age, occupation, gravidity, gestational age, monthly income, parity, and the number of ANC follow-ups, and had a p-value of < .25 and were selected as candidate variables for multivariable logistic regression analysis.
In multivariable logistic regression analysis, residence, maternal age, gravidity, gestational age, and the number of ANC follow-ups persisted to be statistically significant variables associated with OVD at a p-value of <.05.
Hence, mothers who reside in rural areas had 2.09 (AOR, 2.09; 95% CI: 2.01, 7.41) times higher odds of OVD as compared to those who came from urban areas. Besides, mothers with maternal ages 25 to 34 had 4.95 times higher odds of OVD than those with ages <24 (AOR, 4.95; 95% CI: 1.62, 9.2). The odds of OVD were 3.5 times more likely in respondents who were primigravid as compared to their counterparts (AOR: 3.5; 95% CI: 1.26, 9.98). Mothers with gestational age ≥ 42 weeks had 3.09 times (AOR: 3.09; 95% CI: 1.38, 6.9) higher odds of having operative vaginal deliveries than mothers with a gestational age of <37 weeks. On the other hand, mothers who have ANC follow-up <4 times were 3.9 times more likely to deliver by OVD as compared to those who have ANC follow-up ≥4 (AOR:3.9; 95% CI: 1.09, 9.45; Table 3).
Factors Associated With Operative Vaginal Delivery Among Mothers Who Gave Birth at AHMC, 2022.

Notes. AHMC = Adama Hospital Medical College; OVD = operative vaginal delivery; OR = odds ratio; CI = confidence interval; 1.00 = reference. *Refers to significant at p < .05, **refers to significant at p < .001.
Discussion
This cross-sectional study was conducted to assess the magnitude of OVD and associated factors among mothers who gave birth at AHMC. The overall magnitude of OVD among mothers who gave birth at AHMC was 14.8%. Rural residence, maternal age 25 to 34, primigravida, gestational age ≥42 weeks, and ANC follow-ups less than four times were independent determinants of OVD.
In this study, the overall magnitude of OVD was 14.8% (95% CI: 10.8, 18.8). The findings of this study are comparable to the findings of previous studies in Nigeria (11.6%; Ogunniyi & Sunusi, 1988), Tikur Anbessa Specialized Hospital (11.9%; Abebaw & Kebede, 2021), and Jimma University Medical Center (10.3%; Hubena et al., 2018). But higher than the studies conducted in Sokoto, Ibadan, Enugu, Zaria, and Abakaliki, with reported rates of 1.06%, 1.57%,1.5%, 3.6%, and 3.7%, respectively (Adaji et al., 2009; Aimakhu et al., 2004; Iyoke & Onah, 2006; Onoh et al., 2014; Shehu & Omembelede, 2016). The discrepancies in the findings could be attributed to different methods to clinical circumstances between specialists from various fields, resulting in various behaviors and obstetric interventions. Such national discrepancies also were noted within the various regions of several countries (Ameh & Weeks, 2009; Gei & Pacheco, 2011). However, our finding is lower than that of studies done in TASH (18.7%; Obstetricians & Gynecologists, 2000). The variations in the OVD prevalence could be explained by a lack of trained personnel, equipment availability, and experienced human resources.
In this study, the majority of the instrumental deliveries were conducted by vacuum than the forceps delivery. The preference for vacuum over forceps as the instrument of choice found in this review is similar to findings from previous studies (Aimakhu et al., 2004; Iyoke & Onah, 2006; Shehu & Omembelede, 2016). The use of forceps has gradually given way to the use of vacuums over the years. This could be because the vacuum is safer, the skill is easier to understand and has a designed safety mechanism (Alegbeleye et al., 2018; O'Mahony et al., 2010). Also, on contrary, the use of forceps is more difficult technically and requires a long time to master. Despite increasing cesarean section rates, the rate of OVDs remained relatively constant during the study period, in contrast to developed countries where rates are declining due to litigation (Bahl et al., 2011; Bailey, 2005).
In this study, there was a statistically significant association between residence and OVD. Mothers who reside in rural areas had 2.09 times higher odds of OVD as compared to those from urban areas. This finding is supported by a study done in Suhul, Tigray, Ethiopia (Gebre & Hailu, 2017). The possible reason could be due to rural women arriving at the hospital after a long and complicated labor (Yaya et al., 2018).
The odds of OVD were 4.95 times higher among mothers in the age group of 25 to 34 than those with ages <24. This finding is supported by studies done in Norway and Hawassa University Comprehensive Specialized Hospital, Southern Ethiopia (Bago, 2018; Herstad et al., 2015). This association might be explained by the fact that as women's ages increase, so does the maternal complication that leads to OVD.
In this study, the odds of OVD were 3.52 times higher in respondents who were primigravida compared to their counterparts. Similar findings were reported from the studies done in Nigeria and Felege Hiwot Specialized Hospital, Northwest Ethiopia (Adaji et al., 2009; Biru et al., 2019) A possible explanation for this might be a higher tendency to second-stage delays, tight perineum to pass the fetus through the pelvic canal, excessive anxiety and inexperience in labor among primigravidas which all contribute to OVD.
Mothers with gestational age ≥ 42 weeks were 3.12 times more likely to undergo operative vaginal deliveries than mothers with gestational age <37 weeks. This report is in agreement with the finding of the study conducted in Norway (Caughey et al., 2007). The finding is plausible because the risk of maternal peripartum complications increases as pregnancy progresses beyond 40 weeks of gestation which in turn increase the chance of OVD.
Mothers who have ANC follow-ups <4 times were 3.9 times more likely to deliver by OVD as compared to those who have ANC follow-ups ≥4. This might be because a high-risk mother is picked during follow-up and advised to deliver using operative procedures. In addition, good ANC links, the mother with the formal health system and increases the chance of using a skilled attendant at birth.
Strengths and Limitations of the Study
This study's major strength was its attempt to address a neglected health issue among mothers in the study area, by collecting data from primary sources. Since the study used a cross-sectional study design, it will be difficult to establish a temporal relationship between the independent and outcome variables.
Implications for Practice and Research
Health professionals working in the hospital's maternity unit are expected to perform a deliberate assessment of OVD needs prior to care, taking into account the identified factors. Researchers may use this study to conduct more in-depth research that includes other variables and triangulation with qualitative data.
Conclusion
The magnitude of OVD in the study area was relatively low. Rural residence, maternal age 25 to 34, primigravida, gestational age ≥42 weeks, and ANC follow-ups less than four times were independent determinants of OVD. Thus, mothers should be encouraged to get the recommended four ANC follow-ups, and more research is needed to identify and address those issues of why mothers do not have the recommended number of ANC visits.
Footnotes
Acknowledgments
The authors wish to express their heartfelt gratitude and appreciation to mothers and healthcare providers. They also acknowledge Adama General Hospital and Medical College—Institution Review Board for securing ethical letters timely.
Author Contributions
W.K.T., M.S.G., and Y.M.N. contributed to the study's conception, design, data collection, analysis, and the first draft of the manuscript. A.M.G., N.T.B., and T.K.B. provided advice on the study design, data collection, statistical analysis, and final published version. The final manuscript was read and approved by all authors.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Institutional Ethical Review Board of Adama General Hospital Medical College with an Ethical number of AGHMC/2241/2020 and a support letter was written for AHMC by Adama Health Bureau. Then permission was obtained from the Human Resource Office of the hospital. After getting permission from the office, eligible and volunteer mothers were requested. All respondents were assured of the study's objective and their full right to take part in the study and/or withdraw from the study if they were not comfortable with the interview. Every participant was provided a written consent form that included the study's goal, process, and benefit. Selected mothers who agreed to participate in the study were included, and data were recorded anonymously to protect participants’ privacy and confidentiality. and the names of the informants were not included in the questionnaire.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.