
Abstract
Background
The COVID-19 pandemic has disrupted mothers’ and children's access to essential health services. Concerns about the transmission of COVID-19 to infants resulted in strict procedures, which then caused delays in initial contact and breastfeeding. This delay then impacted the well-being of mothers and babies.
Purpose
This study aimed to explore the experience of mothers with COVID-19 in breastfeeding. This study was qualitative research with a phenomenological approach.
Methods
Participants were mothers with a confirmed history of COVID-19 during the breastfeeding period either in 2020, 2021, or 2022. Semi-structured in-depth interviews were conducted with 21 mothers. Data were analyzed using thematic analysis.
Results
Three themes were obtained: breastfeeding during the mother was confirmed COVID-19, changes in the mother's condition, and social support received by the mother. Based on this theme, it can be seen that mothers are temporarily separated from their newborns, which causes breastfeeding difficulties. Mothers confirmed to have COVID-19 in 2020 and 2021 appear to have more significant concerns about transmitting COVID-19, as indicated by the mother's decision not to breastfeed and to undergo separate isolation with the baby.
Conclusion
Mothers need support to continue to breastfeed. The benefits obtained from breastfeeding are far more significant than efforts to prevent transmission by separating mother and baby, so mothers should be encouraged to continue breastfeeding.
Introduction
Coronavirus disease-19 (COVID-19) causes service restrictions in almost all health services (Direktorat Kesehatan Keluarga, 2020). Service constraints impede access to key maternal and infant health care, such as mother-infant interaction and breastfeeding (Lubbe et al., 2020; Renfrew et al., 2020). It has been proven in previous studies that breastfeeding provides essential benefits for both mother and baby (Aşcı et al., 2021; Mufdlilah et al., 2022). For mothers, breastfeeding can reduce the risk of postpartum hemorrhage, postpartum depression, anemia, breast cancer, and degenerative diseases such as heart disease and type 2 diabetes (Dieterich et al., 2013; Mocelin et al., 2020; United Nations Children's Fun, 2018). For infants, breastfeeding that is given early and exclusively can save more than 820,000 children under the age of five each year (Doan et al., 2020; United Nations Children's Fun, 2018). In addition, breast milk protects infants from the risk of infection by viruses or bacteria that can cause death (United Nations Children's Fun, 2018). Babies that directly breastfed by mothers with COVID-19 are considered safe based on the finding that the risk of spreading COVID-19 during breastfeeding is low (Bertino et al., 2020; Luo et al., 2021; Pereira et al., 2020; Sultana & Yasin, 2021).
World Health Organization advises COVID-19 women to continue breastfeeding their newborns by paying attention to health protocols and the mother's ability to give breast milk, specifically through breastfeeding or giving expressed breast milk (Karana, 2020; Sultana & Yasin, 2021; World Health Organization, 2021). This recommendation is supported by evidence from previous studies showing that mothers with COVID-19 do not transmit it to their babies (Guo et al., 2021; Pissarra et al., 2020; Salvatore et al., 2020). Babies who were given rooming-in and allowed to be breastfed directly, then repeated PCR examinations on the fifth to the seventh day, showed negative results. As a result, if health measures are followed appropriately, COVID-19 transfer through breast milk and horizontally is extremely unlikely (Oncel et al., 2021; Salvatore et al., 2020). This indicates that breast milk still needs to be given to babies even though the mother is in a COVID-19 condition (Bardanzellu et al., 2021; Karana, 2020).
However, several studies also show that babies of mothers with COVID-19 were not directly breastfed or not given mother's milk because of fears of transmission and separation of mothers. The study of Pissarra et al. (2020) showed that mothers were worried about the transmission of COVID-19 to their babies, so mothers decided to separate from their babies and delay breastfeeding until SARS-CoV-2 was negative (Pissarra et al., 2020). Nevertheless, if the goal is the health and well-being of mothers and children, the impact of the separation must be considered (Stuebe, 2020). Babies separated from their mothers also have a physiological and psychological impact on mothers and babies and interfere with the continuity of the breastfeeding process (Pacheco et al., 2021). The impact of delaying skin-to-skin contact between mother and baby can disrupt the physiology of newborns. In addition, the separation of the baby also causes stress for the mother because of the loss of opportunities for bonding or early closeness between mother and baby (Pacheco et al., 2021; Stuebe, 2020). Based on several studies that have been conducted, it showed that mothers with COVID-19 could not optimally breastfeed their babies because there were obstacles that they faced. Therefore, researchers aimed to explore the mothers’ experiences with COVID-19 in breastfeeding.
Review of Literature
In the background, we have conveyed the important benefits of breastfeeding for mothers and babies (Dieterich et al., 2013; Mocelin et al., 2020). However, the condition of COVID-19 has had an impact on maternal and child health services, including breastfeeding services (Lubbe et al., 2020; Renfrew et al., 2020). The World Health Organization (WHO) has recommended that the practice of breastfeeding by mothers with COVID-19 be safe by following health protocols. However, several previous studies have shown that mothers with COVID-19 could not give breast milk directly to their babies and rooming in is not carried out on the basis of preventing transmission (Pacheco et al., 2021; Pissarra et al., 2020). This is the main gap or problem in this study, so researchers want to find out more about the experiences of mothers with COVID-19 in breastfeeding. The purpose of this study was to gain experience of mothers with COVID-19 in breastfeeding.
Methods
Design
This study used a qualitative method with a phenomenological approach. This approach was used to describe certain events as a result of ongoing interactions and life processes packaged as life experiences (Streubert & Carpenter, 2011). Researchers used this method and approach to explore experiences that mothers confirmed COVID-19 and during the breastfeeding period so it was appropriate with the purpose of this research.
Research Question
The COVID-19 pandemic has hampered mothers’ and children's access to basic health care. Due to concerns about the transmission of COVID-19 to infants, strict procedures were implemented, resulting in delays in initial contact and breastfeeding. Therefore, the research question is how was the experience of mothers with COVID-19 in breastfeeding?
Participants
The research was conducted in some community health center working areas in Central Java Province and the Special Region of Yogyakarta, Indonesia. Creswell recommends a sample size in qualitative research with phenomenology of 5–25 participants and Morse suggests at least 6 participants (Kumar, Kumar, et al., 2020). The recruitment of participants was assisted by the village midwives and local cadres as gate keepers or facilitators in this study. The researcher conveyed to the village midwife regarding the research carried out and the expected participant criteria. A total of 21 mothers who met the criteria were willing to participate in this study.
Inclusion/Exclusion Criteria
Determination of participants based on purposive sampling technique, that is, participants are determined to be oriented to the research objectives selected according to the criteria of participants that have been previously determined (Gibbs, 2018). Participants’ inclusion criteria included mothers with a history of COVID-19 during the breastfeeding period (when newborns to children aged less than or equal to 24 months), could communicate fluently verbally and be willing to become participants.
Institutional Review Board Approval
Prospective participants who meet the inclusion criteria and are willing to become participants are given an informed consent form. Ethical approval was obtained prior to implementing data extraction and analysis. The researcher maintains the confidentiality of the participant data and writes the identity of the participant anonymously.
Data Collection and Analysis
This study used an in-depth interview technique using field notes, and the interview process was recorded using an audio recorder. The researchers 1 and 3 are midwifery lecturers with doctoral/PhD degrees who already have research experiences. The researcher 2 is a midwifery master's degree student who has received qualitative research insights and training. Researchers conducted direct interviews with 17 participants at participants’ homes, and four were interviewed online in June-July 2022. The duration of the interviews was 30–45 min. Researchers gave semi-structured questions to mothers using open-ended questions. The researchers conducted a pilot interview on a mother who had similar characteristics to the participants. The data were analyzed by using the thematic analysis method. Thematic analysis is one way to analyze data to identify patterns or find themes through researchers’ data (Braun & Clarke, 2006). The data analysis steps carried out were: (1) the researchers read the interview transcripts repeatedly then (2) recorded the data to be used as a starting point for discovering codes. After that, (3) grouping the initial codes that have been obtained and then developing the initial theme. Furthermore, (4) the researchers conducted a review of the themes that had been obtained. The researcher ensured that the data in the theme must come together in a meaningful way. (5) The next step was to interpret each theme and then develop it by providing an explanation of the essence. In the final step, the researcher wrote and developed the overall report.
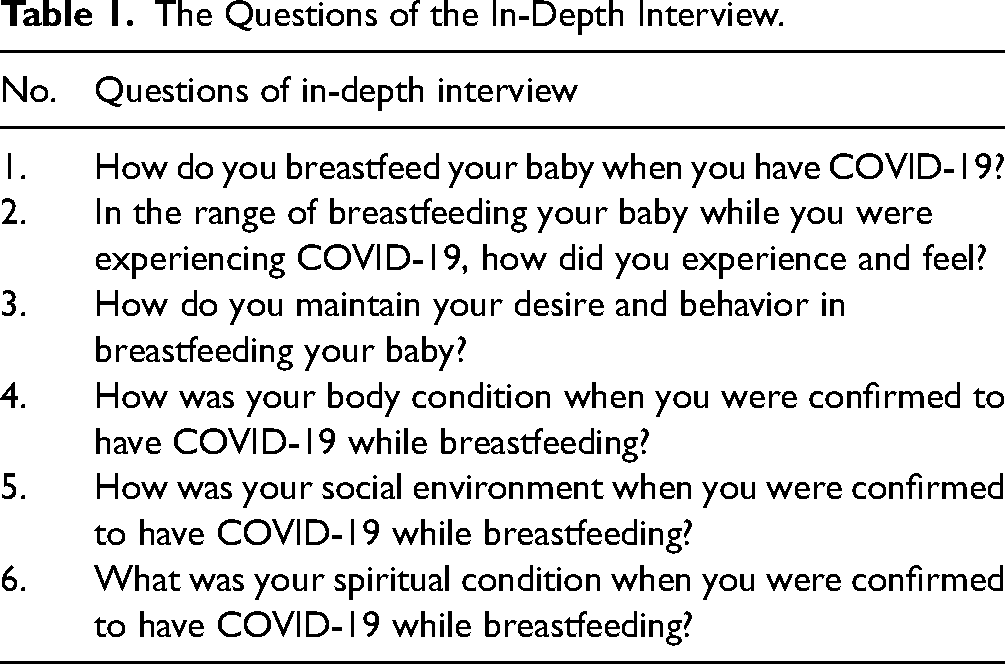
The research refers to strict criteria for maintaining the trustworthiness and validity of qualitative research compiled by Lincoln and Guba (Forero, 2018). The criteria are credibility, transferability, dependability, and confirmability. The steps taken to maintain rigor, that is, collect data according to the conditions of the participants without any distortion, member checks to ensure the results or clarify the results of interviews, conduct transcription by writing word by word from the recordings obtained so as to minimize loss of meaning from interview data, show the quotes and write down the entire analysis process and data systematically (Table 1).
The Questions of the In-Depth Interview.
Results
Participant Characteristics
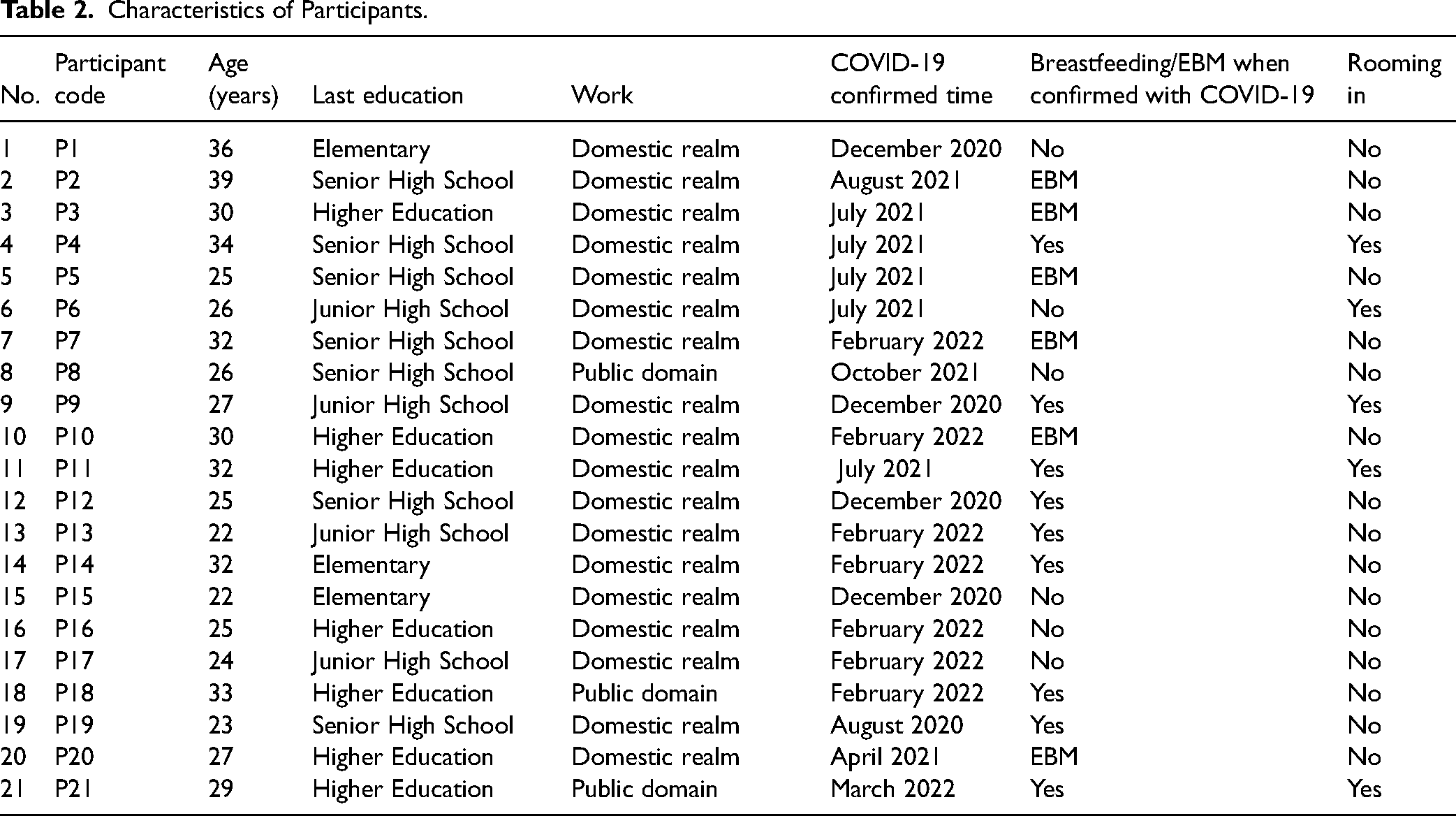
Participants are mothers with a history of COVID-19 while breastfeeding in the age range of 22–39 years with education varying from elementary to master's degree and all mothers are Muslim.
The results showed that 28.6% of mothers with COVID-19 continued to breastfeed (direct breastfeeding), 28.6% gave expressed breast milk and 42.9% did not breastfeed. Most of mothers (76.2%) were not rooming in (mothers and their babies stay together) when the mother was confirmed with COVID-19. All of the mothers who gave birth with COVID-19, there was no early initiation of breastfeeding (Table 2).
Characteristics of Participants.
Research Question Results
Breastfeeding During the Mother was Confirmed to Have COVID-19
Mothers’ experience with COVID-19 in breastfeeding found several sub-themes (Table 3).
Themes and Subthemes.
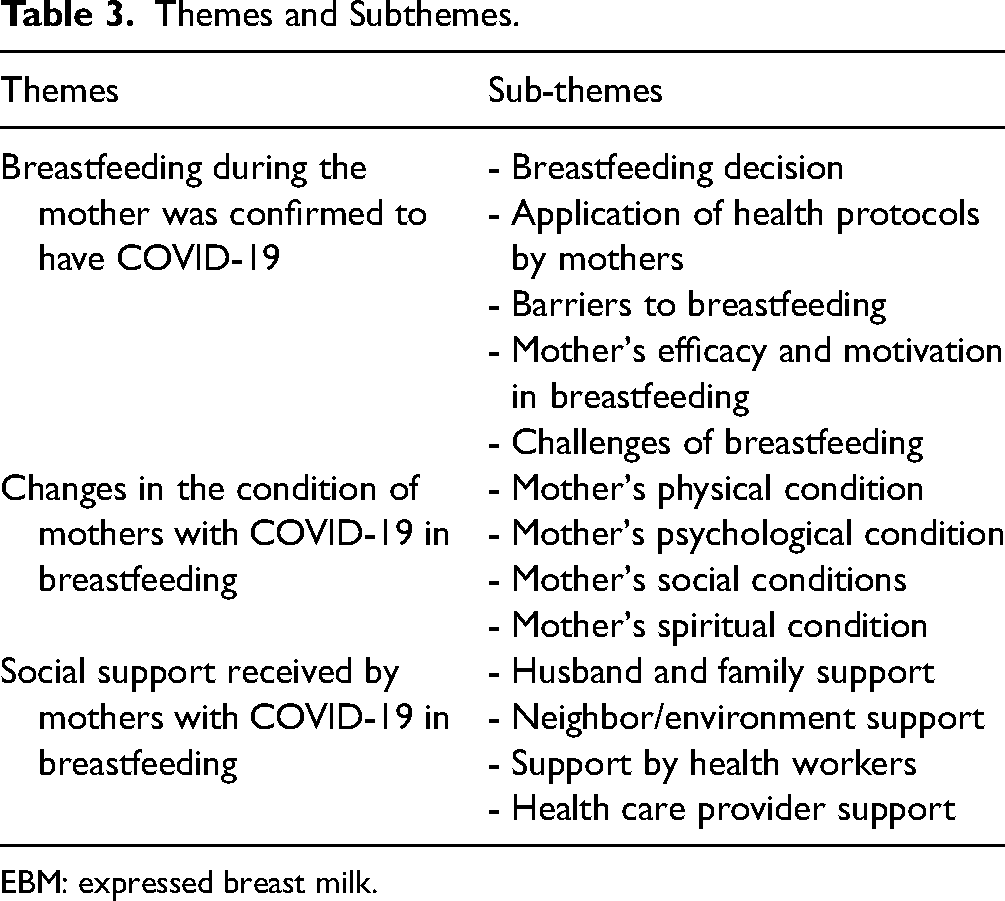
EBM: expressed breast milk.
Breastfeeding Decision
This sub-theme covers how mothers decide whether or not to breastfeed their newborns after testing positive for COVID-19. The mother revealed that when she was declared COVID-19, she continued to breastfeed her baby directly or by expressing breast milk. “… as usual, breastfeeding mothers….” (P4)
“ Yes, it is pumped continuously, yes a little, but it comes out quite well…” (P2)
Some participants decided not to breastfeed while confirmed COVID-19.
“Yes, pumped every day, but the breast milk is thrown away…” (P1)
Some participants breastfed using expressed breast milk, and only a few participants did not breastfeed when they were confirmed COVID-19. Two participants who were confirmed to have COVID-19 in 2020 did not breastfeed for as long as they were confirmed. Only one confirmed participant in 2021 did not breastfeed the baby when confirmed COVID-19. Participants who confirmed COVID-19 in 2022 continued to breastfeed their babies directly or with expressed breast milk.
Application of Health Protocols by Mothers
The sub-theme of applying health protocols by mothers describes mothers’ experiences with COVID-19 in implementing health protocols in breastfeeding their babies. Some mothers said that when they were sick, they breastfed or expressed breast milk by implementing health protocols. …. I have to wear a mask, also before holding the baby, I have to wash my hands, wash my hands with a mask before breastfeeding. (P9)
… before pumping, I always wash my hands first, use soap…, I dry them, use hand sanitizer, … wear a mask, yes…. the pacifier or the breast milk bottle…. I sterilize it first… then I dry it… (P10)
Barriers to Breastfeeding
The sub-themes of breastfeeding obstacles include babies needing special care, separation of mothers and babies, and mothers’ concerns about transmitting COVID-19 to their babies. The baby was referred. …. (P2)
….immediate isolation…, alone, no one to accompany . …. I can't meet the baby, I can't meet my husband. (P12)
… not giving breast milk to the baby, afraid about it . (P8)
The obstacles that arise in 2020–2022 are the separation of mothers and babies.
Mother's Efficacy and Motivation in Breastfeeding
Effectiveness and motivation in breastfeeding describe the mother's experience about the mother's belief in the ability to breastfeed and motivate the mother in breastfeeding, including the mother's perception of breastfeeding and the benefits of breastfeeding as well as the motivation to breastfeed. … Breast milk is cheap, economical, practical. It also doesn't cause allergies, which is also good for the brain baby, the immune system is also good, and it contains vitamins; basically, there are many benefits. (P1)
Challenges of Breastfeeding
This sub-theme describes participants’ experiences regarding what keeps mothers trying to breastfeed challenges, such as breast milk not coming out/coming out little, tiny nipples, and babies being reluctant to suckle. This challenge occurs when the mother is sick and after experiencing COVID-19. Efforts to overcome difficulties and maintain breastfeeding by participants include: Yes, when I got home, … it still didn't come out, but I try and try again (P12)
…. I eat a lot and pump every day, so I produce milk every day. (P1)
…. that was the day … how much it started to decrease because there was still not enough breast milk, I finally looked for a breast milk donor . … (P3)
Changes in the Condition of Mothers With COVID-19 in Breastfeeding
Mother's Physical Condition
This sub-theme explains the participants’ condition while they are declared COVID-19 and the symptoms they experience. …, like fever …. cold, … the throat feels uncomfortable . … no smell at all. ….. (P11)
In addition to experiencing the symptoms above, some participants did not experience symptoms when they were declared COVID-19. The statements of the participants include: …. no complaints, nothing at all,…. I don't have a fever, I don't have a cough, I don't feel anything, it's just normal… (P9)
Mothers who confirmed positive COVID-19 in 2020 showed no severe symptoms experienced; even four out of five mothers were asymptomatic. However, the majority of confirmed participants in 2021 and 2022 showed symptoms including fever, cough, runny nose, anosmia, headache, sore throat, and even shortness of breath. This condition may be influenced by different COVID-19 variants, namely SARS-CoV-2 or early COVID-19 variant (2020), Delta variant (2021), and Omicron variant (2022).
Mother's Psychological Condition
This sub-theme describes the mother's mental state in the form of things felt and thought by the mother during breastfeeding and while being declared COVID-19. Participants conveyed feelings of sadness, symptoms of anxiety, disappointment, surprise, and rejection of the conditions they faced. … it's sad, I want to be able to initiate early breastfeeding,… I can’t immediately try breastfeeding like that. (P16)
In the beginning, I don't dare to breastfeed, … I am afraid of transmitting the virus to baby (P1)
Startled,…. I'm confused too, … don't feel sick, don't feel like a cold, why am I being tested for COVID with positive result… (P7)
Mother's Social Conditions
This sub-theme describes the condition of the mother's interaction with the surrounding environment during the breastfeeding process and confirmed COVID-19, namely the existence of social isolation/restrictions and stigma from the community. … when I wanted to go home, when I got home, it turned out that the house was already excited that I had COVID and all the residents were far away from all of my family… (P9)
All participants experienced social restrictions through isolation for approximately two weeks. Mothers with confirmed COVID-19 in 2020 and 2022 experience stigma from society.
Mother's Spiritual Condition
This sub-theme describes the mother's experience relating her emotional state to God. Participants expressed spirituality in the circumstances they experienced, including the power of prayer, surrendering to God's decrees, and breastfeeding, which is a fortune from God . ….continue to pray… thank God… I'm in good health. (P7)
Submit to the circumstances … however I have to keep moving forward, … do not forget to keep praying …. (P1)
… because breast milk has been given from God, of course… (P10)
Social Support Received by Mothers With COVID-19 in Breastfeeding
Husband and Family Support
This sub-theme describes participants’ experience getting support from their husbands and families. ….my husband goes back and forth to deliver food, and he just left it on the terrace… (P10)
Yes, sincerely already, … when my mother and father-in-law call me, they continue to advise that…, they always bring something, fruit or other food … (P11)
Neighbor/Environment Support
Participants received instrumental support by being assisted in providing food and groceries and offering assistance. … all the neighbors too, they are kind, those who bought the groceries… (P20)
Support by Health Workers
The sub-theme of health worker support describes mothers’ support from health workers who provide services, including midwives, doctors, nurses, and other health workers. They said that if I want to be exclusively breastfed, I can only pump it… (P8)
Yes, tell me to keep the distance, …. tell me to wear a mask when breastfeeding, keep washing my hands like that, keep washing my hands so keep it clean, the doctor said (P14)
Some participants stated that they had not received information from health workers regarding breastfeeding while the mother was sick.
…no information about it… (P20)
Health Care Provider Support
This sub-theme describes the condition of providing health services for mothers during confirmed COVID-19 in breastfeeding. Participants stated that at the beginning of breastfeeding, namely after delivery at the hospital, the mother was immediately separated from the baby and isolated. …. after birth, we are separated and can’t meet at all…. must be separated for 14 days… (P5)
Several participants who gave birth at the community health center stated that they were treated directly with their babies. Besides, mothers could still breastfeed while observing the health protocols for preventing COVID-19. …yeah… the baby and I were immediately rooming-in care (P6, 26 years old, 2021)
It was found that there were differences in maternal care with COVID-19 during the breastfeeding period between the hospital and community health center.
Discussion
Breastfeeding During the Mother was Confirmed to be COVID-19
Most participants in this study continued breastfeeding their babies during COVID-19, even though the babies were initially given formula because the milk had not yet come out. Previous research has found that mothers with COVID-19 still want to breastfeed their babies/children (Aşcı et al., 2021; Pereira et al., 2020). Mothers also perceive breast milk can protect their babies/children from diseases or viruses, including COVID-19. This perception increases the motivation of mothers to continue to prioritize breastfeeding even though the mother is in a COVID-19 condition (Aşcı et al., 2021; Mufdlilah et al., 2018; Radwan & Sapsford, 2016).
The condition of COVID-19 requires mothers to make a decision whether to breastfeed their babies or not. This sub-theme was obtained when some mothers still decided to breastfeed directly or through expressed breast milk and several participants decided not to breastfeed their babies because of fears of transmission. The literature study by Vassilopoulou et al. (2021) on 27 studies in 2020 showed that 13 studies stated that mothers with COVID-19 continued breastfeeding, and two studies showed that mothers gave expressed breast milk. Nine studies mentioned that mothers did not breastfeed when confirmed COVID-19, and three other studies did not have data related to breastfeeding (Vassilopoulou et al., 2021). Breastfeeding is carried out either directly through breastfeeding or expressed breast milk (Anand et al., 2021; Aşcı et al., 2021; Fumagalli et al., 2021; Luo et al., 2021; Oncel et al., 2021). Aşcı et al. study (2021) stated that almost all mothers with COVID-19 (93%) still decide to breastfeed their babies (Aşcı et al., 2021; Fumagalli et al., 2021). This study also showed that some mothers give breast milk through expressed breast milk. Mothers with COVID-19 can also breastfeed their babies through expressed breast milk if the condition of the mother and baby does not allow for direct breastfeeding (Oncel et al., 2021; Spatz et al., 2021; United Nations Children's Fund, 2020).
Some participants stated that they still pumped breast milk so that milk would continue to be produced, but breast milk was not given to the baby but was thrown away. Another study showed that mothers who were afraid of transmitting COVID-19 through breast milk were 58% of the participants (n = 36) (Doshi et al., 2021). Previous research has also shown that there are mothers with COVID-19 who do not breastfeed (Oncel et al., 2021; Peng et al., 2020; Pereira et al., 2020; Pissarra et al., 2020; Vassilopoulou et al., 2021).
Most participants in this study had implemented health protocols for their babies during contact with babies, including breastfeeding babies or expressing breast milk. This result is supported by previous research, which states that the prevention of transmission procedures performed to reduce the risk of transmission during breastfeeding are washing hands, wearing a mask, disinfecting all touched surfaces, and washing the breasts with soap and water (Aşcı et al., 2021; Elhalik et al., 2020; Peng et al., 2020; Vassilopoulou et al., 2021; Yang et al., 2020).
Participants in this study encountered breastfeeding challenges, such as the baby's medical condition necessitating special care and anxieties of transmitting and separating mother and baby. The survey of Salvatore et al. (2020) showed that there were 12 infants (15%) requiring treatment in the NICU (Salvatore et al., 2020). Concern about the transmission of COVID-19 from mother to baby is also an obstacle in breastfeeding (Fumagalli et al., 2021). Such circumstances cause the mother to opt not to breastfeed, to separate from the infant, and discard the expressed milk until she is declared negative (Pissarra et al., 2020). Another obstacle faced by the participants was the separation of mother and baby. The recommendation for separation of mother and baby is carried out only for medical reasons, namely if the mother's condition shows severe symptoms or there are complications from the mother's disease and the baby's condition requires NICU care (Elhalik et al., 2020).
Participants also tried to overcome problems and maintain breastfeeding, among others, by meeting nutritional needs, breast massages, and giving donor breast milk. Based on previous research, it has been shown that nutritional intake in breastfeeding mothers affects milk production (Endah & Oktavianti, 2014). Breast massage is used to help expel breast milk and overcome the problem of breast milk that has not come out, in addition to providing nutritional needs. The research results by Katmini and Sholichah (2020) stated that breast massage could facilitate milk production (Katmini & Sholichah, 2020). Participants made efforts to maintain breastfeeding because breast milk is insufficient, namely by giving donor breast milk. The study of Pereira et al. (2020) stated that nutrition in case 1 was through donor pasteurized breast milk and expressed breast milk until the 17th day, and then the mother was already breastfeeding (Pereira et al., 2020).
Changes in the Condition of Mothers With COVID-19 in Breastfeeding
This study found that the most common symptoms were fever, cough, and runny nose. In addition, mothers’ symptoms are sore throat, headache, anosmia, and shortness of breath. Some participants also reported a decrease in appetite. Previous research has shown that mothers’ clinical symptoms include cough, fever, muscle aches, fatigue, sore throat, nasal congestion or runny nose, loss of taste and smell, and shortness of breath or difficulty breathing. Symptoms of diarrhea, nausea or vomiting, conjunctivitis, and sneezing may also occur but are rare (Pérez-Bermejo et al., 2021). In addition to participants with clinical symptoms, this study also found participants without symptoms. This result is in line with research by Pereira et al. (2020), which stated that in 10 cases out of 22 mothers with COVID-19, there were no clinical symptoms felt by the mother (Pereira et al., 2020). Luo et al. (2021) also showed that there were two women (14.3%) (Luo et al., 2021).
In addition to the mother's physical condition as indicated by clinical symptoms, changes in the psychological state appear in mothers with COVID-19. Psychological conditions in participants in this study include sadness, anxiety, disappointment, feelings of shock, and rejection of the conditions faced. In addition, there is also trauma, and one does not want to go back to remembering when mothers experienced COVID-19. Research by Aşcı et al. (2021) explained that mothers limit physical touch with their kids, which causes mothers to feel depressed and unable to bond with their children (Aşcı et al., 2021). The mother's sadness emerges not only from the fact that she cannot see the baby but also from the reason that she did not initiate breastfeeding at an early age and thus cannot breastfeed her baby directly. Research by Sanjeev Kumar, Kumar, et al. (2020) shows that mothers with COVID-19 who are separated from their babies, even though their mothers have a desire to breastfeed, cause mothers to feel unable to carry out their maternal duties (Kumar, Rathore, et al., 2020).
This study also stated that participants felt shocked when they were declared COVID-19. In addition, some participants indicated that they felt traumatized and did not want to recall the situation when they were confirmed to have COVID-19. Previous research stated that nearly 95% of all participants with COVID-19 reported feeling sad, angry, shocked, and afraid. Furthermore, a systematic review also found that patients with COVID-19 were more likely to suffer from post-traumatic stress syndrome (AlKuwaiti et al., 2022). Therefore, the psychological condition of mothers with COVID-19 in breastfeeding requires special attention so as not to cause prolonged adverse effects.
The condition of mothers with COVID-19 was also related to social restrictions. According to the findings of this study, the mother felt isolated exclusively in her home and did not interact with her immediate family or her surroundings. Previous research has stated that mothers feel lonely and isolated during isolation and distant from their babies and their families (Aşcı et al., 2021; Fumagalli et al., 2021; Kumar, Rathore, et al., 2020). In addition, strict isolation and quarantine measures have led to delays in early initiation of breastfeeding and expressing expressed breast milk for babies until three weeks after delivery (Peng et al., 2020; Pissarra et al., 2020). Participants in this study also claimed that the COVID-19 condition they were experiencing caused their neighbors or the surrounding environment to provide a negative appraisal or stigma by staying away and not showing empathy. This result is in line with the study of AlKuwaiti et al. (2022), which stated that participants also experienced stigma from their environment due to the COVID-19 condition (AlKuwaiti et al., 2022). However, some participants also expressed empathy for their neighbors by providing motivation through messages, sending food ingredients needed during isolation, and offering help.
Participants in this study reported that as long as COVID-19 was confirmed, they were sure their health would improve with prayers to Allah SWT. This condition is supported by previous research, which states that participants increase prayer during illness, maintain a positive mindset, and believe that everything from God has made it easier for them during isolation (AlKuwaiti et al., 2022). According to the findings of this study, the participants claimed that the condition they were in was a destiny that had to be lived. This result is in line with previous research, which says that this is a form of the Muslim faith. Faith in destiny is to believe and believe that whatever happens is the will of Allah SWT (Hariyadi & Muflihin, 2021). Participants also stated that breastfeeding is a blessing from Allah. Participants believe that God's gift is the best. It is supported in the Quran and Hadith that no milk is healthier than breast milk for babies to consume. Allah has given the best provisions for babies stored in their mother's breasts (Mehrpisheh et al., 2020).
Social Support Obtained by Mothers With COVID-19 in Breastfeeding
The findings in this study indicate that mothers get support from their husbands, namely by meeting the mother's needs, delivering breast milk for the baby when the mother is isolated, taking time to care for the baby, helping to care for the baby, and helping position the baby while breastfeeding. Mothers also obtain support from the family by providing motivation and advice, sending food when the mother is in isolation, and taking care of and caring for the baby when the mother is in isolation. Research results Aşcı et al. (2021) showed that most mothers with COVID-19 received support from their partners and their families (mother and mother-in-law) who accompanied them during isolation (Aşcı et al., 2021). The instrumental support received comprises baby care, positioning the baby when breastfeeding, and offering emotional support through motivating good remarks about breastfeeding and getting better soon from COVID-19 (Aşcı et al., 2021). The support from husband and family is undoubtedly beneficial for mothers to support breastfeeding for babies. This study also obtained the results of neighbors’ support for several participants by sending food or groceries, offering assistance with necessary medical devices, and providing support via WhatsApp. This support shows the concern for the environment of mothers with COVID-19. This result is in line with research showing the support of neighbors or friends who provide support so that mothers feel cared for (Diamond et al., 2020). In contrast to some individuals who received stigma from their neighbors, the mother feels disappointed by this condition.
Health workers provided information, assistance with expressing breast milk, communication, and assisting in connecting mothers with their families, as well as encouragement for women to remain calm and not think about things. Aşcı et al. (2021) showed the provision of information in the form of treatment options and their effects on breastfeeding and safe breastfeeding methods for infants. These obstacles occur in breastfeeding, such as insufficient breast milk, breastfeeding support, and breastfeeding support systems for mothers with COVID-19 needed so that mothers do not feel confused and worried about breastfeeding (Aşcı et al., 2021; Fumagalli et al., 2021). Furthermore, the mother requires emotional support from health providers, such as empathy, feeling safe and comfortable, and lowering concerns about the mother and baby's condition (Brown & Shenker, 2021; Fumagalli et al., 2021; Kumar, Rathore, et al., 2020). Most participants had received support from health workers, but some revealed that they had not received precise information regarding breastfeeding during the mother's illness. In line with existing research, participants felt they had not received enough information regarding breastfeeding procedures while the mother had confirmed COVID-19 (Aşcı et al., 2021; Oncel et al., 2021; Rodríguez-Gallego et al., 2022). Therefore, comprehensive information is needed to minimize the worries/doubts about the mother's feelings (Fumagalli et al., 2021).
Support from health care providers is also required. Based on this study, mothers with COVID-19 who gave birth at the health center could join in directly with their babies and were not advised to isolate them separately from their babies. Unlike the participants who gave birth in the hospital, they were immediately separated from the baby and treated in the isolation room. They are also informed to continue separation with the baby for 14 days or two weeks after discharge from the hospital. Babies need close contact with their mothers immediately after birth to bond and continue breastfeeding. Focus especially in the first 1–2 h after birth, that is, skin-to-skin contact and subsequent impacts on breastfeeding, cortisol levels, crying, sleep, pain reduction, and physiological, emotional, and cognitive regulation. Separating mother and baby after birth is considered a source of stress, leading to increased childhood developmental problems. Early separation can cause harmful epigenetic changes and impair infants’ neurodevelopment (Császár-Nagy & Bókkon, 2018; Luo et al., 2021). Furthermore, mothers who are separated from their newborns owing to premature labor suffer mental damage, whereas skin-to-skin contact enhances the mother's mood (Luo et al., 2021). Health care providers need to develop a new breastfeeding support roadmap to set standards of care and update clinical practice taking into account current conditions and possible long-term changes that are a consequence of this COVID-19 pandemic conditions (van Goudoever et al., 2022).
Strengths and Limitations
This study provides an overview of the condition of mothers with COVID-19 during the breastfeeding period. This study used a qualitative phenomenological study method so that it was very appropriate to use it to explore the experiences of mothers with COVID-19 in breastfeeding. The data collection for this research was carried out using the in-depth interview method, both offline and online according to the willingness of the participants so that participants felt more comfortable and could freely tell what they experienced. This research covered five districts/cities in Central Java Province and the Special Region of Yogyakarta with a total of 21 participants in different exposure years, namely 2020–2022 so as to obtain participants with diverse and interesting experiences with a fairly representative number. This study explored the experiences of mothers when they experienced COVID-19 during the breastfeeding period in the past so that sometimes there are things that participants need to remember. However, the data obtained in this study are consistent in mothers with confirmed COVID-19 in 2020, 2021, and 2022.
Implications for Practice
Health workers can optimize the provision of lactation services considering the large benefits obtained from breastfeeding and rooming-in even though the condition of the mother with COVID-19 is compared to the separation of mother and baby.
Conclusion
Most mothers with COVID-19 continue to breastfeed their babies directly or through expressed breast milk by implementing health protocols. Most mothers are isolated and separated from their babies for approximately 14 days. Mothers’ obstacles in breastfeeding include babies needing special care, separation of mothers and babies, and mothers’ concerns about transmitting COVID-19 to their babies. A mother's self-efficacy is a driving force for mothers to continue breastfeeding their babies and make efforts to overcome the difficulties that occur in breastfeeding, which are challenging for mothers. The physical, psychological, social, and spiritual changes in mothers are the impact of COVID-19 experienced mothers. Health workers are expected to increase understanding regarding breastfeeding among mothers with COVID-19 so that they can provide comprehensive care and education so that mothers with COVID-19 do not experience confusion when giving breast milk to their babies. Given the substantial benefits of breastfeeding and rooming-in care, especially in the case of COVID-19 mothers, compared to the separation of mothers and newborns, it is hoped that health care providers may adopt standard operating procedures that take the well-being of mothers and babies into account. As a result, help from husbands, families, the environment, health workers, and health service providers is required to enable COVID-19 mothers to continue breastfeeding.
Footnotes
Acknowledgments
The authors would like to thank all the participants in this study. The authors also would like to thank the National Strategic Grants Fund (DP2M) of the Ministry of Education, Culture, Research, and Technology of the Republic of Indonesia for funding this research through the Master's Thesis Grant program 2022. They also thank the Master of Midwifery Study Program Faculty of Health Sciences, Universitas’ Aisyiyah Yogyakarta, for supporting and facilitating this research.
Author Contributions
The concept and study design: M, NIK, EKS; collecting data: NIK; data analysis and interpretation: M, NIK, EKS; processing the draft of the manuscript: M, NIK, EKS; critical revision of the manuscript: M, NIK, EKS; article finalization: M, NIK, EKS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the National Strategic Grants Fund (DP2M) of the Ministry of Education, Culture, Research, and Technology of the Republic of Indonesia through the Master's Thesis Grant program 2022.
Ethical Aspects and Conflict of Interest
This research has obtained an ethical approval from the Ethics Commission of Universitas ‘Aisyiyah Yogyakarta with number 1474/KEP-UNISA/V/2022.