
Abstract
Anesthesia is one of the most significant developments of modern medicine that allows treatment involving unbearable pain to be performed while the person is relaxed, asleep, and with no memory of the procedure. However, patients around the world have little or limited knowledge regarding anesthesia. It is in view of that, this study was undertaken to assess patients’ knowledge on anesthesia services at a preanesthetic clinic and recovery wards of a teaching hospital in Northern Ghana. Descriptive quantitative survey was used to identify patients’ knowledge about anesthesia services with the purpose to observe, describe, and document the situation as it naturally occurs. Data obtained from 100 participants were double entered into Microsoft Excel spreadsheet and validated for data errors. Data were then coded and exported to SPSS version 20.0 for Windows for analysis. Descriptive statistics such as frequencies and percentages were used to describe data. The results showed that 53% of participants were aware of anesthesia services as opposed to 47%. However, 30% of the respondents could not identify the type of anesthesia services, while 68% did not know the route of administration of anesthetic agents. Most importantly, 51% had no idea of what an anesthetist is, while 33% knew nothing about the role anesthetists play in the health delivery system. As a result, 26% thought an anesthetist is the theatre nurse, while 25% were of the view that the doctor doubles as the anesthetist. Anesthetists must therefore make conscious efforts to disseminate information before and after surgeries and follow-up clients who underwent anesthesia to provide for continuity of care. This may include preparation of leaflets, brochures, videos, and handouts to improve patients’ knowledge and attitude and to disseminate it to all departments in the hospital where anesthesia services are provided.
Introduction
Anaesthetists' role has extended not only inside but also outside the traditional operating room setting as they play critical role in intensive care units, trauma centers, pain clinics, and as a member of resuscitation teams all over the world (Kong et al., 2017). For instance, anesthetists provide services for magnetic resonance imaging, computed tomography, fluoroscopy, endoscopy, electroconvulsive therapy, and cardiac catheterization (Raymer, 2013). They have also assumed administration and leadership position on the medical staff of many hospitals and health-care facilities (National Practitioner Programme, 2007). As a result of reforms and contributions of anesthesiologists and nurse anesthetists, anesthesia is now much safer and more pleasant for the patient than it was 50 years ago (Okine, 2017). Factors contributing to the improvement include a fuller understanding of physiology, better preoperative assessment and preparation of patients for surgery, closer monitoring of anesthetized patients and introduction of new techniques such as muscle relaxants, tracheal intubation, and calibrated vaporizers for volatile anesthetic agents (Raymer, 2013). Improvements in anesthesia have allowed surgeons to attempt more complicated operations on an increasing number of patients which has resulted in a growing demand for more anesthetists. Every anesthetist needs a foundation in medical science for his or her clinical technique. A sound knowledge of physiology and pharmacology is essential, with understanding of changes in the illness or injury (World Health Organization, 2003).
Notwithstanding the tremendous reforms in anesthesia and role of anesthetists, unfortunately, Kong et al. (2017) found that patients who have undergone previous operations learned little or nothing about anesthetists and their work. Hence, there is a widespread public misconception about the role of anesthetists and their responsibilities inside or outside the operating room. Poor public knowledge of anesthesia and the role of anesthetists has been documented in developing and developed countries (Marulasiddappa & Nethra, 2018). In Ghana, a study conducted in 2015 at the Korle-Bu Teaching Hospital in Accra with 279 patients showed that nearly half the patients indicated anesthesia was all about “putting people to sleep and waking them up” (Aniteye, 2014; pp. 69–70). Less than 15% of patients had knowledge of the role of anesthetists outside the confines of the operating theatre suites (Raymer, 2013). Other studies showed that patient’s knowledge and perception on anesthesia practice and role of anesthetists in health-care delivery even in teaching hospitals was limited. The role of anesthesia extends beyond the operating room and is necessary in postoperative monitoring, intensive care units, for coexisting medical conditions, as well as providing pain relief (particularly in children and women in labor). A workforce trained in basic anesthetic techniques at the primary health-care level can also resuscitate critically ill patients or those with severe trauma and stabilize their condition, before transfer to a more specialized facility (Mooruth, 2015; Okine, 2017). To safely deliver anesthesia in emergency and surgical procedures, investments for appropriate training are required. This will improve the knowledge of patients presenting for surgery regarding anesthetists and anesthesia. It is in view of this assertion, this study assesses patients’ knowledge on anesthesia services by examining patients’ views on types of anesthesia services, risks of anesthesia services, and the role of anesthetists in health-care delivery.
Methods
Descriptive quantitative survey was used to categorize patients’ knowledge about anesthesia services with the purpose to observe, describe, and document the situation as it naturally occurs. The study was carried out at a preanesthetic clinic, surgical, and obstetric theatres recovery wards at Teaching Hospital in Northern Ghana. The hospital is the third largest tertiary health institution located in Northern Ghana with 800 bed capacity. Participants included for this survey were patients taken through preanesthetic assessment teaching by the anesthetist about anesthesia, and those who had undergone anesthesia but have revered postoperatively. This group of participants were chosen in order to assess the effectiveness of pre- and postanesthetic teaching of clients by anesthetists. The convenience sampling method was used to select 100 patients on daily basis consecutively as they were booked for surgery at the anesthetic clinic together with those in the chosen wards recovering from anesthesia until the 100th person was selected. Ethical clearance was obtained from Hospital’s institutional review board to conduct the study. The facility-based study made use of respondents accessing health care at the Teaching Hospital from the five Regions in Northern Ghana. Data were collected using a researcher-developed questionnaire extracted from previous studies in literature reviewed and validated by the Institutional Review Board or Research Department of the Tamale Teaching Hospital before administration. The data were double entered into Microsoft Excel spreadsheet and validated for data errors. Data were then coded and exported to SPSS version 20.0 for Windows for analysis. Descriptive statistics such as frequencies and percentages were used to describe or summarize data as well as determine the level of awareness of respondents on anesthesia.
Results
Demographic Characteristics
Participants sociodemographic characteristics were examined to find out the influence these may have on the knowledge of anesthesia. In addition, 100 patients participated in the study. Results show that 57% were males and 43% were females. The age ranged from 10 years to 75 years with a majority (63%) being 30 years and older. It was interesting to note that 55% had either no education at all or only gone through junior high school. Table 1 shows the demographic details of the respondents.
. Demographic Features of Respondents.

Patient’s Knowledge on Anesthesia Services
Out of the 100 participants, 62% of the clients received anesthesia for the first time and about 53% had heard of the term anesthesia as opposed to 47%. Out of those who heard about anesthesia, 22% got their information from the anesthetist while 11% were informed by the surgeon. Significantly, 30% of the respondents did not know the type of anesthesia they were given during operation. With reference to anesthetic assessment, only 28% preferred assessment by the anesthetist, 21% wanted assessment from the scrub nurse, 20% chose surgeon, and 31% wanted any health worker. About 84% recognize that anesthetic assessment before surgery is relevant; however, 68% did not know the route of administration of anesthetics and 50% were not even informed of the kind of operation that would be carried out. Results also demonstrate that 47% of the clients’ greatest fear regarding operation was postoperative pain, 25% dread of complications from anesthesia, and 28% are afraid the surgeon–anesthetist conflicts. The findings also show that 69% did not know about the possible risk for complication from anesthesia; however, 39% of participants thought that general anesthesia has the higher risks for complications. Regrettably 49% did not know who should be an anesthetist (Table 2).
Respondents’ Knowledge on Anesthesia Services.

Role of the Anesthetist in Health-Care Delivery
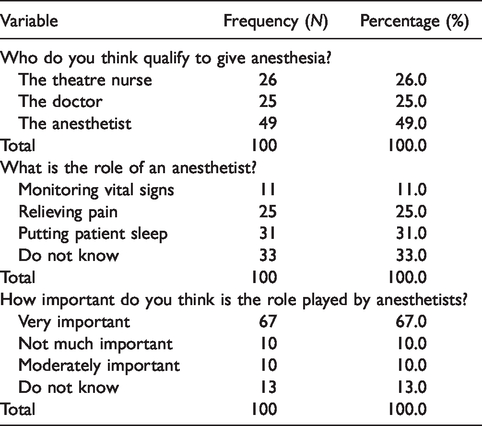
The findings in this study show that 49% of patients seeking anesthesia services know that the anesthetist qualified to give anesthesia. In contrast, 26% thinks the theatre nurse can give anesthesia, while 25% says the doctor doubles as the anesthetist. With regard to role of the anesthetist, 33% did not know the anesthetist role in health-care delivery, 31% think the anesthetist role is to put patient to sleep during operation, while 25% see the anesthetist as someone who relieves patients’ pain during and after surgery. Notwithstanding the confusion in the role of the anesthetist, 67% were of the view that the anesthetist role is very important (Table 3).
. Client’s Views on Role of the Anesthetist in Health-Care Delivery.
Risks of Anesthesia Administration
In respect of the risk of anesthesia, 64% of the clients surveyed were not told that aspiration, vomiting, and cardiac arrest constitute anesthesia risk. As a result, 68% were not educated on anesthesia risks. Furthermore, while 48% thinks giving anesthetic agents without preanesthetic assessment was the most fatal risk, 22% say it is riskier when the surgeon refuses to pay attention to advice from the anesthetist. Even though there is evidence that most participants were not educated on anesthesia risk, 24% of them feel patients’ disregard to risk education on anesthesia is dangerous. About 60% of the participants surveyed are not aware anesthetists can be sued for incompetence (Table 4).
Respondents’ Knowledge on Risks of Anesthesia Administration.

Discussion
Anesthesia is an important supportive specialty that allows sophisticated surgery to be performed. Therefore, the purpose of this study was to determine the knowledge of patients on anesthesia services and anesthetists’ role in health facilities in Northern Ghana. Out of the 100 clients who were surveyed less than 30% of the participants were engaged in an occupation with a regular income and had relatively higher knowledge in anesthesia service compared with those within the poverty belt. This could be explained in a sense that people with high income could afford materials containing information about anesthesia which they may use to enhance their knowledge. This confirmed the assertion of Smith (2017) that higher income correlated well with correct knowledge of clients on anesthesia. In terms of education, the majority of participants were below the tertiary level with a significant number never attending school. Meanwhile, Pinto et al. (2017) demonstrated among a Brazilian population that education was a statistically significant factor to define patients who knew about anesthesia services and anesthetists. This may be explained by the relationship that those of higher intellect look for more information and show more coherent assimilation. Similarly, Urban, Bleckwenn, Ana, and Bonn (2002) demonstrated again that a high level of education correlated well with the knowledge of anesthesia services and role of the anesthetist.
In terms of knowledge of anesthesia, Marulasiddappa and Nethra (2018) stated patients globally, especially in less developed countries, have little or limited knowledge regarding anesthesia and limited access as there is a severe shortage of anesthesiologists and limited supply of anesthesia in low-resourced settings. This assertion was confirmed in this study as a significant number of patients had poor knowledge of anesthesia. Meanwhile, a better understanding and recognition of the importance of anesthesiology may help improve patient outcomes. Anesthetists also must make concerted efforts to design structured information dissemination programs before and after surgeries and follow-up clients who underwent anesthesia. This routine will promote information retention regarding anesthesia services because the study revealed that majority of clients seeking surgical care had no idea regarding anesthesia services.
This notwithstanding a survey in Island by Smith (2017) revealed that 95% of patients were knowledgeable regarding anesthetists and anesthesia services. The survey however created a trend which showed that patients of poor and developing nations had less knowledge on anesthesia services when compared with the developed world. The general public health awareness is not matched with the awareness of anesthesia procedures, but it is a major supportive specialty that allows major advanced surgery to be performed. Consequently, many authorities consider it imperative to educate their patients about the anesthesia activities. This study also unveiled that anesthetists seldom explain anesthetic procedures to clients; hence, most of the patients did not know how anesthetists work and could not choose for themselves one type of anesthetic technique or the other. In a similar study done in West Africa, which determined the types and technique of anesthesia, out of 229 patients surveyed, 91.3% knew the type of surgery they were going to have, while 67.6% had knowledge of the anesthetic techniques to be used (Mooruth, 2015). In this study, a majority (60%) of participants never had the opportunity to be exposed to education about anesthesia services and practices. Meanwhile in some countries, patients who are to undergo surgery are provided at the time of admission with small booklets that describes the roles of anesthetists. Patients may also be shown a video of perioperative patients’ care and the procedures followed after admission to the wards. This may help alleviate anxiety and help the patient get the most out of the service available. Unfortunately, in most health facilities in Northern Ghana, anesthetists only have brief contact with the clients where a head to toe evaluation is done after which the anesthetist is missing from the scene until they meet again in the operating room. As a result of this, most participants in this study knew next to nothing about the role of the anesthetists and could not tell who was qualified to administer anesthesia. This was evident when some clients expected to receive anesthesia from the scrub nurse or any health worker. Some participants even described the anesthetists as an assistant surgeon; a clear sign of lack of knowledge or poor client–anesthetist relationship. These findings confirmed findings of a research conducted in England which established that knowledge level of patients regarding the role of anesthetists was as low as 1% to 5% (Smallwood, 2005). Another study conducted in Finland also established that patients thought anesthetists work only in the operating room; they do not know the role of anesthetists in the intensive care unit, emergency service, pain clinics, and with other invasive procedures (Story et al., 2015). Also in this study, less than two thirds of patients had heard of anesthesia. This may indicate poor public education about anesthesia, which could negatively impact the knowledge and perception of the general public regarding anesthetist’s role in health-care delivery.
In respect of the risks of anesthesia administration, the majority of the participants expressed lack of knowledge and were equally not educated on these risks as they awaited their turn to be anesthetized. The induction of anesthesia abolishes the normal laryngeal reflexes that prevent inhalation of stomach contents. Due to gastric, biliary, and pancreatic secretions present even during fasting, nil per os indicates the restriction of oral intake for a period of time prior to surgery, minimizing the volume, acidity, and solidity of stomach contents. Such measures reduce both the risk of aspiration occurring as well as the severity of pneumonitis, should an aspiration event occur. Another dangerous phenomenon that was identified in this study is the perceived surgeons–anesthetists conflicts before and during surgeries. These seeming confrontations between the anesthetists and surgeons normally result in cancellation or delay of cases. Hence, 28% of patients in this study while awaiting surgery were afraid of doctor anesthetic conflicts. On the other hand, 47% were also worried about postanesthetic pain. This implies, patients may not know that this modern era painless postoperation is possible. This therefore calls for rigorous education of patients to empower them to take their health into their own hands. What was also regrettable in this study is the fact that about 60% did not even know they could sue health workers including anesthetists for negligence and incompetence.
Despite the high risks for complications associated with anesthesia, there are equally enormous benefits such as earlier postoperative recovery, reduced preoperative anxiety and pain, and improved patient satisfaction. A good patient–anesthetist relationship created during the preoperative visit may aid in reducing patient anxiety. Reliable information assists in mentally preparing the patient for the intended surgery and anesthesia, thereby improving patient cooperation.
Conclusions
This study provided a review of patients’ knowledge on anesthesia services and the role anesthetists play in health-care delivery. Generally, patients in this study exhibited poor knowledge on anesthesia and role of anesthetists. This was a result of anesthetists’ failure to explain anesthetic procedures to clients. These notwithstanding, there are enormous benefits of anesthesia and anesthetists and their associate stakeholders must therefore make aggressive efforts to disseminate information before and after surgeries to enhance information retention regarding anesthesia services. This must be central to advancing patient care, both in its broader concept and patient empowerment specifically.
Strengths
The study was conducted in a referral center in the whole of the Northern sector of Ghana and parts of Southern Ghana. This has provided variety of patients from wider scope in a single confined area for the survey. We were also able to identify a number of areas of deficiency in patients’ knowledge in the direction of anesthesia that, when addressed, will improve practice, affect policy, and add to the body of knowledge in anesthesia.
Limitations
The study design was cross-sectional study design which was used to investigate a phenomenon at a single point in time and could not determine cause and effect as done in the trend study. The respondents were recruited from a single selected hospital which made it difficult to generalize results to the whole population of patients in Ghana. However, these limitations do not invalidate findings in this study.
Recommendations
Anesthetists should make enough efforts to design structured information dissemination programs before and after surgeries and follow-up clients who underwent anesthesia. This may include preparation of leaflets, brochures, videos, and handouts to improve patients’ knowledge and attitude and to disseminate it to all departments in the hospital where anesthesia services are provided. Anesthetists and stake holders should collaborate to improve patients’ health information regarding anesthesia and bring about a positive attitude toward the profession and its professionals. Anesthesia scholars should embark on research on ways to improve patients’ knowledge and attitude toward anesthesia and anesthetists.
Acknowledgments
We acknowledge Yussif Zakaria and Mr. Alhassan Mohammed Shamudeen, Head of Research Department, Tamale Teaching Hospital, for all his support given to us during the data collection period and helping us obtain the ethical certificate to conduct the study.
Author contributions
S. S. carried out literature review and developed the methodology and instrument of the study. He also analyzed, interpreted data, and discussed findings of the study. S. S. was the major contributor in the writing of the manuscript. J. G. and A. B. Y. did the editorial work and doubled as the consultants for the study. A. W. and S. A. collected the data in the field from respondents (patients) and entered data into the SPSS software version 20. All authors read and approved the final manuscript.
Consent
We declare that consent to undertake this study was granted by the research department and ethics unit of the Tamale Teaching Hospital. All participants who took part in this study gave their consent and the aims of the study were explained to them in the language they understood well.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.