
Abstract
Antenatal care (ANC) is a critical intervention, and providing high-quality care results in positive maternal and neonatal outcomes. A facility-based cross-sectional study design was used among 4 public health facilities in Dessie Town, and 421 pregnant mothers were selected by a systematic random sampling technique. Data were collected using observation and interview through a pretested questionnaire, then entered and analyzed using EpiData 4.7 and SPSS 26. Finally, predictors of the quality of the ANC service were identified using multivariate logistic regression. Overall, 270 women (64%) were satisfied with ANC services in this study. Only 49 (70%) attributes of structural quality and 32 items (69.56%) of process quality attributes were met, which is inadequate and needs improvement. Mothers aged 20 to 24 (AOR = 3.067; 95% CI = 1.416, 6.641); mothers who took 30 min and more to get to the health facility (AOR = 2.745; 95% CI = 1.475, 5.111); mothers who had a choice of care providers (AOR = 2.829; 95% CI = 1.676, 4.777); merchants (AOR = 2.310; 95% CI = 1.077, 4.955); and farmers (AOR = 2.111; 95% CI = 1.138, 3.8) were positive predictors of women's satisfaction with ANC services. Although ANC client satisfaction was good, structure-quality attributes and process-related quality were inadequate and needed significant improvement. This implies that urgent interventions are needed to improve process and input quality attributes.
Introduction
Globally, maternal and perinatal morbidity and mortality continue to be unacceptably high, particularly in developing countries. 1 In 2019, ∼ 303 000 women died due to pregnancy-related causes (15% of all global deaths), 2 1.9 million babies were stillborn, and 2.3 million neonates died in 2021. 3
Antenatal care (ANC) can be defined as the holistic care provided to pregnant women and adolescent girls by skilled care providers in order to achieve the best health conditions for both the mother and fetus throughout pregnancy. 4 ANC reduces maternal and perinatal morbidity and mortality both directly, by screening and treating pregnancy-related health problems, and indirectly, by identifying women and girls who are at a higher risk of complications during labor and childbirth and ensuring referral to an appropriate care level. 4
According to the UNICEF 2022 report, 88.3% (urban: 92.3%; rural: 81.99%) and 66.29% (urban: 77.54%; rural: 56.02%) of pregnant women in the world had received ANC at least once and 4 or more times, respectively. Furthermore, in the Sub-Saharan region, 81.9% of pregnant women had received ANC at least once, and 53.58% had received it 4 times or more. 5 According to the 2019 Ethiopian Demographic Health Survey (EDHS), 74% of Ethiopian pregnant women received ANC at least once, and 43% received it 4 or more times. 6 Despite this, up to half a million pregnant women in Ethiopia may suffer from short-term and long-term illnesses or injuries as a result of pregnancy-related issues each year, and this implies that both the coverage of service and the quality of ANC need more effort to reach the desired goal. 7
Quality is a key aspect of achieving any nation's sustainable development goal. The extent to which a service meets the plan to deliver that service while offering services at a fair price and meeting the client's expectations is referred to as “quality.” To help deter pregnancy-related issues, the content and quality of ANC must be revised.8–12
ANC quality is measured along three dimensions based on the Donabedian model: input, process, and outcome. 13 Physical infrastructure, documentation, skilled staff, medical drugs, vaccinations, equipment, and supplies are all examples of input dimensions. In addition, interpersonal communication, history-taking, clinical examination, counseling, health screening, and preventive measures are all process attributes. Ultimately, the outcome will be measured by client satisfaction.14–16
Previous studies found that factors such as client socio-demographics, socioeconomics, and care providers’ technical skills; insufficient financial provisions; integration with other health services; and the availability of consumable items, drugs, and basic equipment were associated with the quality of ANC services.17–22
In Ethiopia, the actual experience is that pregnant women attend at least 4 ANC visits. However, the WHO recently issued holistic guidelines on routine ANC for pregnant women, including a minimum of 8 ANC visits. Besides, it puts an emphasis on quality over quantity and what is known as a “positive pregnancy experience,” which is a fresh approach and is designed to enhance both neonatal and maternal outcomes. 23 The new holistic ANC guideline has not been implemented in most developing countries, including Ethiopia, due to inadequate access and availability of services, miscommunications, a shortage of resources and drugs, and an insufficiency of trained professionals.24–26
Although some studies on the quality of ANC have been done in different parts of Ethiopia, ANC quality studies have mainly focused on the frequency of visits or constituents of focused ANC and used different quality measurement models and tools. In particular, facility inventory and process attributes of ANC quality instruments were not used effectively. Furthermore, it has not been documented yet in the study area. Therefore, the aim of this study was to assess the quality of ANC in public health centers in Dessie, northeastern Ethiopia, and determine the predictors. As a result, it would close an existing information gap and serve as the basis for action to enhance ANC quality.
Methods
Study Design, Area, and Period
The facility-based cross-sectional study was employed from February 2022 to June 2022 in Dessie town, which is located 400 km, from Addis Ababa and ∼ 500 km from the Amhara region's capital, Bahirdar. It has a total of 6 public health facilities and one comprehensive and specialized hospital and is estimated to provide service for about half a million residents. Moreover, there are also 4 private hospitals, more than 10 higher-level clinics, and a number of medical suppliers and drug stores. The main economic activity is trade.
Study Population
All pregnant women who attended ANC services at public health facilities in Dessie Town are a source of population. However, the actual data was taken from pregnant women who attended ANC services at public health facilities in Dessie Town during the data collection period.
Eligibility Criteria
Pregnant women who attended ANC services during the data collection period and were willing to participate were included in the study.
Sampling Size
A single population proportion formula was used to calculate the sample size. The following assumptions were taken into account: The proportion of mothers in Bahirdar Zuria who were satisfied with the service they received was 52.3%, 27 with a 95% level of confidence and a 5% margin of error. By including a 10% nonresponse rate, the total sample size increased to 421.
Sampling Technique
Among the 6 public health facilities in Dessie Town, 4 of them were selected in a simple random method through the lottery technique, namely: Dessie Health Center, Tita Health Center, Banbuha Health Center, and Segno Health Center. Population allocation to size was performed to obtain study subjects by considering the last 6 months of client flow at each facility. Based on this, the total average number of ANC visits per month was 2000 (600 in Dessie Health Center, 520 in Banbuha Health Center, 390 in Tita Health Center, and 490 in Segno Health Center). Then, in the selected health centers, a commensurate allotment based on size was made. As a result, 126 mothers were involved at Dessie Health Center, 110 at Banbuha Health Center, 82 at Tita Health Center, and 103 at Segno Health Center. Ultimately, a systematic random sampling technique was used to obtain the pregnant mothers for every fifth interval until the required sample size at each public health facility was obtained. The ANC registered list was considered as a sample frame.
Operational Definition
Input (structural) quality: It includes 70 items to assess infrastructure, statistical data, record-keeping, staff, medical drugs, vaccinations, equipment, and supplies. Each item received a 1 if the answer was yes and a 0 if the answer was no. Each health facility's overall score ranged from 0 to 70. As a result, the following structure qualities of the center were scored: Health facilities with fewer than 35 infrastructure items were deemed to have poor structure quality. Moreover, those health facilities are meeting between 36 and 53 items of infrastructure that were considered to be of inadequate structural quality. Furthermore, those health facilities that meet the above-mentioned 53 items of infrastructure were considered to have good structure quality. 28
Process quality: From 46 items, a scoring system was developed to calculate 5 dimensions of process attributes: (1) interpersonal communication, (2) history taking, (3) clinical examination, (4) counseling, and (5) health screening and preventive measures. This scoring system determines whether or not an accepted process quality standard has been met.
All activities were taken into account and given a score of “1” if they were observed and performed in accordance with accepted care standards, and a score of “0” if they were not. To determine a score for each dimension of care, the scores of the key items for each individual client–provider interaction observed were added up and averaged. Furthermore, the overall summary score was created by aggregating the mean scores of all care dimensions and was assigned as the process index. The total scores ranged from 0 to 46. As a result, the quality care process was scored as follows: low quality < 23; moderate quality 23 to 37; and high quality ≥ 37. 29
Outcome component of quality: Satisfaction is defined as pregnant women's self-reported level of satisfaction expressed as satisfied or dissatisfied based on exit interviews of the ANC service received from health professionals. 28 The satisfaction tool includes 3 sections: client personal information, perception of pregnant mothers with technical and service management of facilities, and general satisfaction of pregnant women (which comprises 12 items). Accordingly, clients who scored higher than the median were considered to be satisfied with ANC service, and clients who scored lower than the median were classified as dissatisfied with ANC service. 28
Data Collection Instruments and Techniques
For each measure of quality, the authors used different data collection tools. The client satisfaction tool and the facility inventory tool were adapted from WHO: An Assessment Tool for the Quality of Outpatient ANC and PNC for women and newborns. 28 Furthermore, the ANC observational checklist tool was modified to assess the following process qualities: maternal and child health integrated program and maternal and Newborn Quality of Care Survey. 29 The information was gathered through observation and in-person interviews with semistructured questionnaires. The adapted tool was then modified and contextualized to fit the objectives of the study and translated into the local Amharic language, particularly the exit interview.
Data Quality Management and Analysis
The tool has been translated into the local Amharic language. For 2 days, 8 data collectors (with a BSC in midwifery and ANC training) and 2 supervisors (with an MSC in public health) were trained, and a pretest of 5% of the sample size was conducted at Haik Health Center (α=0.831). The data was cleaned, encoded, and entered into Epi-Data software Version 4.7 before being exported to SPSS Version 26 for analysis. The proportion of each of the 3 quality attributes was calculated and assessed using descriptive statistics. A bivariable logistic regression analysis was performed to select variables for multivariable analysis. Besides, those variables that had a P-value < .2 during the bivariate analysis are transferred and analyzed in multivariable logistic regression. Then, after doing a multivariable analysis, a variable was deemed statistically significant if its P-value was < .05. The adjusted odds ratio with its 95% confidence interval was used to demonstrate the strength of association between each explanatory variable and the outcome variable. The variance inflation factor was used to test for multicollinearity. In factor analysis, all outcomes were compared to a reference point using Nagelkerke chi-squares and the Hosmer and Lemeshow test for model fit.
Results
Sociodemographic Characteristics of the Respondents
This study included 421 pregnant mothers, 421 of whom finished the interview successfully, resulting in a response rate of 100%. The mother's mean age was 29.56 years (SD ± 6.012 years), and the preponderance of these women, 109 (24.9%), were between the ages of 25 and 29. Moreover, about 241 (57.2%) of respondents had 4 to 6 family sizes. Of the total respondents, 347 (82.4%) were married, 349 (82.9%) had 1 to 3 children, 201 (47.7%) were housewives by occupation, and 143 (34%) had primary education status (Table 1).
Sociodemographic Characteristics of Antenatal Care (ANC) Attendant Women at Public Health Facilities in Dessie Town, Northeast Ethiopia, 2022.

Healthcare Availability and Utilization-Related Characteristics
The majority of respondents (296, 70.3%) drove 5 km to the health facility, and it took 312 (74.1%) mothers 30 min or more to get there; 252 (59.9%) had no one accompany them on their ANC visit; 152 (36.1%) were returning to the ANC for the second time; and their current gestational age was 16 to 24 weeks (35.2%). Further, the majority of respondents (299, 71%) began their ANC visit more than 12 weeks ago; 238 (56.5%) had the opportunity to choose their care providers (Table 2).
Obstetrics and Health Service-Related Characteristics of Pregnant Women who Attended Antenatal Care (ANC) Visit at Public Health Facilities in Dessie Town, Northeast Ethiopia, 2022.

Structural Quality Attributes
Overall, the facility inventory survey mean summary scores indicated inadequate structural quality (49 items, or 70%). Regrettably, all health facilities require immediate interventions to ensure the availability of infrastructure such as adequate waiting rooms, examination rooms, hand washing facilities, and adequate and clean toilets. This infrastructure was particularly deficient (59%). Besides, essential ANC drugs such as magnesium sulfate, injectable antibiotics, and antihypertensive drugs were inadequately available during the time of the survey, and in particular, folic acid supplementation was totally unavailable in all health facilities and needed immediate intervention (Table 3).
Results of Structural and Process Quality Components of Antenatal Care (ANC) in Selected Public Health Facilities of Dessie Town, Northeast Ethiopia, 2022.

Process Attributes Quality
Interpersonal communication performance was almost compromised (only 3 activities were met out of 6) and needs immediate intervention in all health facilities, like greeting and compassionate and respectful care. However, verification criteria in history-taking and clinical examination skills were relatively classified as good quality. Accordingly, the obstetrics and medical histories of the majority of study subjects (90.7%) were obtained, including parity, gravidity, last menstrual period, and health problems encountered during previous pregnancies. Besides, 380 (90.3%) of clients’ blood pressure, weight, and heights of the uterus were examined at least once during the ANC, and vaginal examinations were done among 361 (85.7%) study subjects at least once. Further, care providers partially met the verification criteria for both providing counseling and health screening through laboratory examinations, and preventive measures were deemed inadequate and in need of immediate improvement. As a result, only 117 (27.8%) study subjects had hepatitis B and VDRL tests, and 280 (66.5%) had blood and urine protein tests. Furthermore, only 266 (63.2%) of the study participants received free vitamins and medicine, and none received any folic acid at all. Overall, the process-related quality summary score was 32 items (69.56%), all of which were classified as inadequate and in need of improvement (Table 3).
Women's Satisfaction With the ANC Service
The highest score on the satisfaction component was ANC cost fairness (98.3%), followed by 98.1% of the women being enthusiastic about inviting relatives or friends to utilize the ANC services in the health facilities. On the other hand, the most common dissatisfaction components, 87 (20.7%), were less clean latrines and inadequate water supplies, followed by 52 (12.4%) waiting times that were unfair. Overall, 270 women (64.1%) were satisfied with ANC service, while 151 women (35.9%) were dissatisfied with the service.
Factors Associated With ANC Service Satisfaction
The following variables were found to be predictors of women's ANC service satisfaction after performing a multivariate logistic regression analysis: mothers who found between 20 and 24 years old; time taking 30 min or more to get to the facility; mothers who had an opportunity to a selection of care providers; merchants and farmers by occupation; and had received advice about the birth plan and did not go to a private clinic for ANC service.
In the current study, the odds of satisfaction among mothers who were between 20 and 24 years old were almost 3 times higher (AOR = 3.067; 95% CI = 1.416, 6.641) compared to mothers in the age group between 35 and 49 years old. Similarly, those mothers who did not go to a private clinic for ANC service were 3 times more likely (AOR = 3.33; 95% CI = 1.876, 5.923) to be satisfied than their counterparts. Merchants and farmers mothers by occupation had roughly 2 times (AOR = 2.310; 95% CI = 1.077, 4.955) and 2 times (AOR = 2.111; 95% CI = 1.138, 3.915) higher odds of ANC service satisfaction than housewife mothers. Besides, those mothers who had received advice about the birth plan were 7 times more likely (AOR = 7.122; 95% CI = 2.024, 25.054) to be satisfied with ANC service than their counterparts. Furthermore, those mothers who had the opportunity to select their care providers during ANC visits were nearly 3 times more likely (AOR = 2.829; 95% CI = 1.676, 4.777) to be satisfied than their counterparts. Finally, the odds of a mother taking 30 min or more to get to the facility were nearly 3 times (AOR = 2.745; 95% CI = 1.475, 5.111) more likely to have ANC service satisfaction than their counterparts (Table 4).
Factors Associated With Antenatal Care (ANC) Service Satisfaction Among Pregnant Women Attended at Public Health Facilities in Dessie Town, Northeast Ethiopia, 2022.
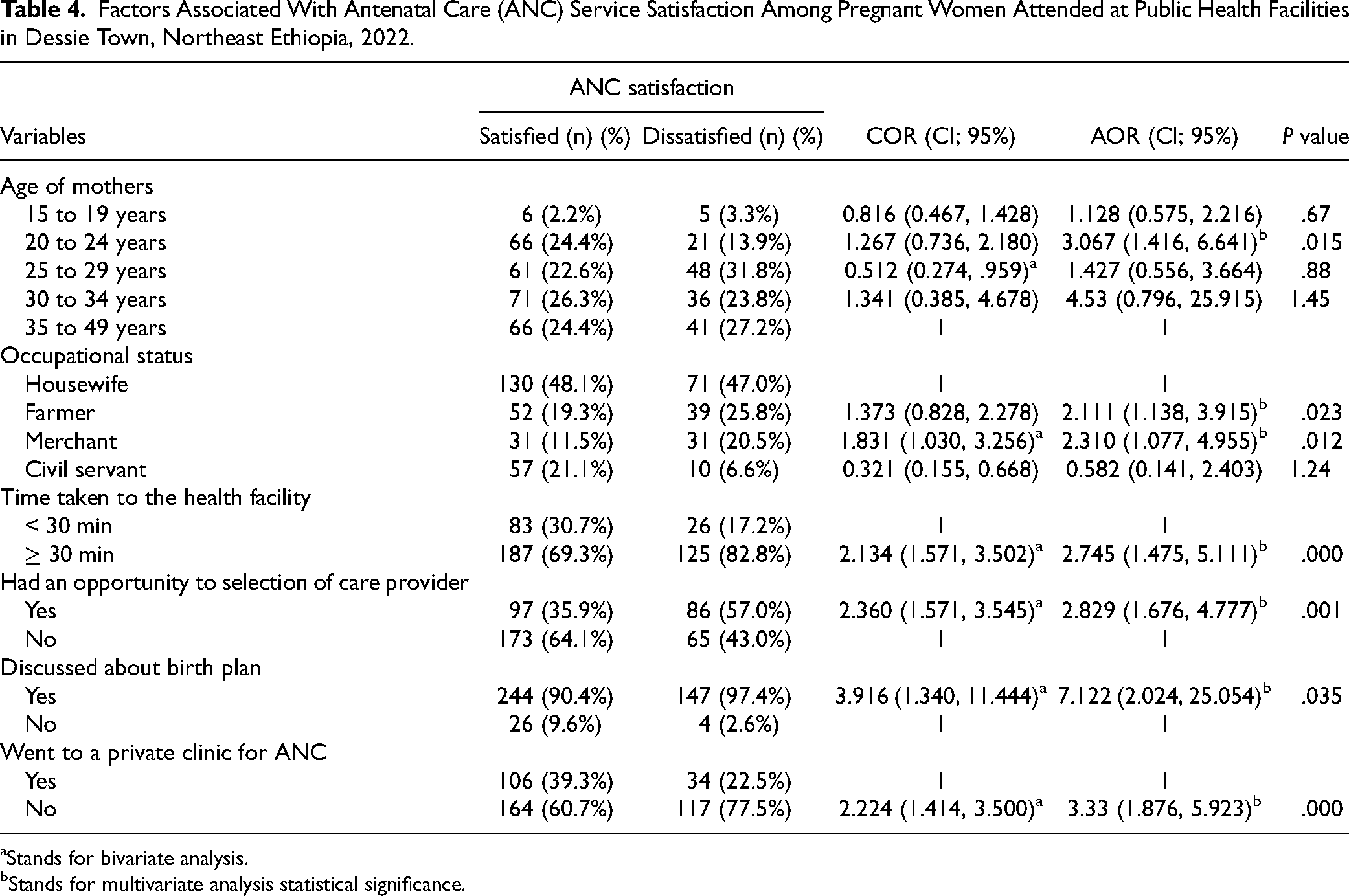
Stands for bivariate analysis.
Stands for multivariate analysis statistical significance.
Discussion
ANC is a chance to encourage the use of qualified birth attendants and positive lifestyles such as breastfeeding, early postnatal care, and birth planning. Several of these chances remain to be missed, despite the fact that more than two-thirds of pregnant women receive at least one ANC visit. Therefore, a quality ANC service should be provided, and the structural, process, and outcome attributes of the quality of the ANC need to be improved simultaneously. As a result, pregnancy-related mortality and neonatal mortality will decrease significantly.
In this study, the structural quality of the ANC clinic was regrettably inadequate. This is in line with studies in the Bele Gasgar District in southeastern Ethiopia, 20 Kellem Wollega, West Ethiopia, 22 and Hossaina Town, Southern Ethiopia. 26 The similarity could be attributed to a lack of decent infrastructure, a shortage of qualified personnel, an immature healthcare finance system, and an integrated pharmaceutical and supply-chain system.
Furthermore, in the current study, the quality of the process attributes of the ANC was insufficient and needed to be improved. This is similar to findings in Nigeria, 18 Kellem Wollega, West Ethiopia, 22 Hossaina Town, Southern Ethiopia, 26 and Wolaita, Southern Ethiopia. 30 This might be explained by a lack of skilled professionals in quantity as well as quality, a high client burden that shortens the interaction time between care providers and clients and makes it likely to have missed an opportunity, a lack of screening equipment such as laboratory machines and reagents, and a lack of essential drug and supplement supplies.
The overall level of pregnant women's satisfaction with the ANC service at selected public health centers of the Dessie city administration was 64%. This finding was comparable with studies on Jimma Zone (60.4%), 31 Debre Tabor Town (59.7%), 19 and Bele Gasgar (55%). 20 However, the rate was lower than those found in other studies conducted in West Ethiopia (79.7%), 22 Gamo-Gofa, Ethiopia (79%), 32 Nigeria (90%), 18 and Sweden (82%). 17 Several studies conducted in Ethiopia found lower rates of client satisfaction than those found in this study: 21.5% in the Gamo Gofa zone, 33% in the Bursa district, and 30.4% in Mizan-Aman.33–35 The variations could be attributed to differences in the pregnant women's subjective nature, the satisfaction indexes used, and the absence of uniform tools for precise classification. Furthermore, the degree of satisfaction may be influenced by the mindset of the clients’ expectations prior to the service and the service they received.
In the current study, the odds of ANC service satisfaction among mothers who found themselves between 20 and 24 years old were almost 3 times higher compared to mothers in the age group between 35 and 49 years old. This is in line with a study in Debre Tabor Town, where mothers aged 18 to 24 years old were satisfied with ANC service. 19
In this study, merchants’ and farmers’ mothers by occupation had 2 times higher odds of ANC service satisfaction than housewife mothers. However, this finding is contradicted by a study done in west Guji, southeastern Ethiopia, where housewives in occupation were more satisfied. 36 The difference might be due to population characteristics and the study area's setting.
According to the findings of this study, those mothers who had received advice about the birth plan were 7 times more likely to be satisfied with ANC service than their counterparts. This is comparable to the Gamo Gofa, southern Ethiopia, study. 33 This implies that providing adequate birth plan counseling during ANC visits makes clients satisfied with the service and improves the habit of institutional delivery, which in turn leads to meeting the target of a good neonatal outcome as well.
In the current study, mothers who took 30 min or more to get to the facility were nearly 3 times more likely to be satisfied with ANC services than their counterparts. This finding is contradicted by studies in Gamo Gofa and Bele Gasgar District.33,20 The possible explanation might be that the distance to a health center or the time required to reach the facility may not be of concern to the client, but rather the compassionate care and general service provided by the care providers. As a result, clients who have traveled a long distance may wish to visit the ANC service in order to have their expectations met. Thus, this implies that health service accessibility is not a guarantee of quality of service.
Limitations
The authors raised the burning issue of the quality of ANC and used the switchboard and the vast survey tool. The local stakeholders can understand which component of the quality of the ANC needs immediate improvement. However, due to the nature of the cross-sectional study design, the authors were unable to establish a causal relationship. Besides, the numerical measurement and data presentation might not sufficiently express the patient experience of the quality of ANC. Therefore, qualitative and follow-up studies will address the current study's limitations.
Conclusion
In this study, although the women's satisfaction with ANC service was reasonably good, the process-related quality and structural quality were inadequate and needed urgent improvement. Furthermore, being young mothers (20 and 24 years old), time taking 30 min or more to get to the facility, having the opportunity to choose care providers, being merchants or farmers by occupation, having received birth plan advice, and not going to a private clinic for ANC services were associated with women's satisfaction with ANC services. A participatory intervention-based plan for ANC service satisfaction shall be developed, with a focus on dissatisfied groups such as older and housewife mothers. The public health facilities shall be kept as the centers of selection for their clients in ANC service by giving them the opportunity to choose their care providers during an ANC visit. Besides, enhancing process-related quality is possible, such as by providing counseling and preventive measures in compliance with guidelines.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank Wollo University, the Department of Pediatrics, and the Child Health Nursing for providing the necessary conditions. Following that, we’d like to thank Dessie City's 4 public health center managers and staff for their assistance. We thank the study participants, as well as the supervisors and data collectors, for their assistance with data collection.
Authors Contributions
The authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit it to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Data Availability
All data generated or analyzed during this study are included in the manuscript and are also available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study protocol was evaluated and approved by Wollo University College of Medicine and Health Science No (CMHS/367/2022) and Ethical clearance was obtained. Permission letters were also obtained from Dessie City's respected public health facilities. Moreover, this study was conducted in compliance with the Declaration of Helsinki. As a result, informed consent was obtained from the study participants prior to study commencement. Anonymous data was taken and the confidentiality of participants’ information was secured.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.