
Abstract
Background
Workplace violence against nurses is a burgeoning public health issue affecting developing countries’ healthcare industries. Medical staff, particularly nursing staff, have been subjected to a high level of violence from patients, visitors, and coworkers.
Objective
Aimed to assess the magnitude and associated factors of workplace violence among nurses working in public hospitals in northeast Ethiopia.
Methods
A multicenter hospital-based cross-sectional study was employed among 568 nurses using census method among public hospitals in Northeast Ethiopia in 2022. The data was gathered using a pretested structured questionnaire and entered into Epi Data version 4.7 before being exported to SPSS version 26 for analysis. Furthermore, at 95% CI, multivariable binary logistic regression was used, and variables with P-values of <.05 were found to be significant.
Result
Out of the total 534 respondents, 56% had been exposed to workplace violence in the past 12 months, with verbal abuse accounting for 264 (49.4%), physical abuse 112 (21%), bullying 93 (17.2%), and sexual harassment 40 (7.5%). Being female nurses (adjusted odds ratio [AOR = 4.85, 95% CI (3.178, 7.412)]), having an age > 41 [AOR = 2.27, 95% CI (1.101, 4.701)], nurses who had drunk alcohol in the past 30 days [AOR = 7.94, 95% CI (3.027, 20.86)], nurses who drink alcohol in their lifetime [AOR = 3.14, 95% CI (1.328, 7.435)], and male patients [AOR = 4.84, 95% CI (2.496, 9.415)] were positive predictors of workplace violence.
Conclusion and recommendation
In this study, the magnitude of workplace violence among nurses was relatively higher. Nurses’ sex, age, alcohol habit, and sex of patients were associated with workplace violence. Therefore, intensive facility-based and community-based behavioral change health promotion activities on workplace violence should be done, with particular focus on nurses and patients.
Introduction
Workplace violence (WPV) is defined as an act or threat of violence against workers that occurs within or outside of the worksite and includes verbal abuse, physical assaults, bullying, sexual assault, and homicide, which is one of the top reasons for workplace deaths (AnnMarie Papa et al., 2013; Boyle et al., 2016; Zhang et al., 2021).
According to the National Institute for Occupational Safety and Health, there are four kinds of WPV in the health-care industry. Type I: The guilty party is a criminal with no ties to the company or its employees. Type II: When a customer, client, or patient receives care or services, he or she becomes violent. Employee-to-employee violence is classified as type III. Personal relationship violence is classified as type IV (Rosenstock, 1997).
WPV among medical personnel has been noted as an issue of public health worldwide, with higher rates particularly in Sub-Saharan Africa, where the quality of care and service is poor (Abdellah et al., 2017). Violence occurs four times more frequently in the medical setting than in any other private setting (Violence, 2007). This is due to the fact that healthcare workers must communicate with their patients, clients, and patient relatives in tough circumstances, and patients or clients may respond violently as a result of their health condition or therapy (ICN, 2003). Nurses, in particular, are frontline forces and more vulnerable to violence than other hospital staff because they have direct access to patients (Weldehawaryat et al., 2020). WPV is a big hurdle for nurses, with more than half of them experiencing at least one act of violence in the previous 12 months across the globe (Choi et al., 2017; Shi et al., 2017; Sisawo et al., 2017; Speroni et al., 2014; Sun et al., 2017; Zahra et al., 2018).
Injuries caused by WPV can be physical, psychological, or both. Physical and psychological WPV has a variety of ramifications, including upsetting emotions, burnout, low job motivation, lack of job satisfaction, substance abuse, and other psychological effects, all of which potentially harm the victims’ well-being and result in poor performance and productivity loss (Boyle et al., 2016; Legesse et al., 2022; Zhang et al., 2017). Furthermore, WPV affects not only victims, their families, and coworkers but also healthcare organizations that have suffered from lost income, health costs, overhead expenses, and litigation (Kitaneh et al., 2012; Najafi et al., 2018). As a result, the health sector has suffered from massive financial losses, poor service quality, and a lack of staff retention (Friend et al., 2018; Kim et al., 2023).
Despite Ethiopian Labor Proclamation No. 377/2003 (Article 92), which states that “employers have a legal obligation to protect their employees’ health and safety,” there is no nationwide Occupational Standard Health policy or professionally established body or association that addresses how the event must be managed and controlled (Legesse et al., 2022, Seblework, 2006).
In comparison to the severity of the problem, there is some evidence demonstrating the proportion of WPV against nurses in eastern, southern, and northern Ethiopia. However, no data is available in northeastern Ethiopia. As a result, this study would fill a knowledge gap and greatly assist local stakeholders in their efforts to prevent and control WPV. Therefore, this study aimed to determine the magnitude of WPV and its predictors among nurses working in public hospitals in northeastern Ethiopia.
Literature Review
WPV is a common practice around the world, with the health industry alone accounting for 25% of incidents; more than 50% of health personnel have already been involved in such incidents (Hahn et al., 2012). A study done in the USA among 284 nurses revealed that 20% were physically assaulted, 43% were threatened with physical assault, and 55% were verbally assaulted (Ridenour et al., 2015). The same is true across Europe; in places like Italy, the magnitude of WPV was 45% (Magnavita et al., 2012), and a study carried out in Germany found that about 70% of nurses experienced physical and 89.4% verbal aggression (Franz et al., 2010). Further, findings from Palestine revealed that WPV was 80.4%, of which 20.8% were physical and 59.6% were nonphysical (Kitaneh et al., 2012).
Evidence from Sub-Saharan Africa revealed that the magnitude of WPV in the health industry was significant, reaching up to 88%, with bullying and sexual harassment being the most pervasive and widespread (Abodunrin et al., 2014). A study in Egypt showed that the WPV was 27.7%, particularly 69.5% verbal and 9.3% physical violence (Abbas et al., 2010). Another study in Malawi discovered that WPV among nurses was 71%, with 22% being physical, 95% being verbal, and 16% being sexual harassment (Duma et al., 2016). Further, the magnitude of WPV in Gambia and Nigeria was 62.1% and 66%, respectively (Douglas et al., 2019; Sisawo et al., 2017). According to Ethiopian studies, the WPV ranges from 29.9% to 82.8% (Fute et al., 2015; Likassa et al., 2017; Tiruneh et al., 2016).
Several studies have found that sociodemographic factors such as sex, educational status, occupational type, and work and organizational factors like direct contact with patients and worrying about violence in their workplaces are related to WPV against nurses (Fute et al., 2015; Likassa et al., 2017; Shafran-Tikva et al., 2017; Tiruneh et al., 2016) (Figure 1).

Conceptual framework shows associated factors for nurses that affect workplace violence adapted and modified from literature (Fute et al., 2015; Likassa et al., 2017; Shafran-Tikva et al., 2017; Tiruneh et al., 2016).
Conceptual Framework
Prevention and control of WPV are means of improving the quality of life of medical personnel. As a result, the quality of care and patient and nurse job satisfaction increased, while also fostering a positive work attitude and organizational productivity. This, in turn, leads to a stable healthcare system and a productive society. Therefore, this study attempted to assess the magnitude of WPV and associated factors among nurses working in public hospitals in northeastern Ethiopia.
Methods
Study Design and Period
A multicenter hospital-based cross-sectional study design was employed in the South Wollo Zone public hospitals in northeastern Ethiopia from May 2022 to June 2022. There are 14 government hospitals with 568 nurses overall in the South Wollo Zone. Of these, one is a comprehensive and specialized hospital, two are referral hospitals, four are general hospitals, and the rest, seven, are primary hospitals with a total of 1150 beds. Moreover, the public hospitals in this zone are estimated to provide for 5 million people.
Inclusion and Exclusion Criteria
The study included all nurses who had worked in south Wollo zone public hospitals for at least 6 months; however, nurses who were unavailable due to maternal and annual leave, as well as nurses who went for short-term training outside the hospital during the data collection period, were excluded.
Sampling Size and Procedure
The study included all government hospitals in the South Wollo Zone. A census was conducted, and all 568 nurses working in government hospitals in the South Wollo Zone during the study period were included in the sample.
Data Collection Technique and Instrument
The data was collected using a pretested, self-administered structured questionnaire adapted from a joint program of the International Labor Organization (ILO), the International Council of Nurses (ICN), and the World Health Organization (WHO) to assess WPV and perceived causes of violence or assault, their response to or reactions to violence, and the hospital procedure for dealing with violence (ILO/ICN/WHO/PSI, 2017). The pretest was done in two hospitals in north Wollo zone (namely, Lalibela and Woldiya comprehensive hospitals) with 5% of the sample size. Based on the findings of the pretest, ambiguous items were amended, and the reliability test was (α = 0.87).
Five components comprise the data collection tools: Part I inquired about six socio-demographic characteristics of nurses, including age, gender, income level, marital status, religion, and ethnicity.
Part II evaluated educational and experience factors and has six items, such as work experience year, length of service in the current working unit, work unit, educational qualifications, and title of nurse.
Part III evaluated work organization factors and has eight items, of which three have a yes/no response, such as working in shifts, working anytime between 12 p.m. and 1 a.m. local time, and having direct physical contact with patients or clients. Furthermore, the number of staff, type of patient, and sex of the patient are all involved in this package.
Part IV: Assessing WPV if the participants experienced at least one incident of WPV in the past 12 months. Part IVA evaluated the physical abuse of the nurses and their reactions to such episodes in the past 12 months prior to the study period and has 18 items if the participants had experienced physical abuse (ILO/ICN/WHO/PSI, 2017). Moreover, Part IVB assessed the verbal abuse of the nurses as well as their reactions to such episodes in the past 12 months prior to the study period. It has 15 items if the participants had experienced physical abuse (ILO/ICN/WHO/PSI, 2017). In Part IVC and Part IVD, an inquiry was made about bullying and sexual harassment and the nurses’ reactions at those scenes, respectively. If the participants had experienced bullying and sexual harassment, there are five and 15 items, respectively (ILO/ICN/WHO/PSI, 2017).
Part V: The performance tool consists of nine items designed to assess nurse performance as well as factors influencing nurse performance. The performance measurement instrument has 5-point Likert scale items (1 = extremely poor, 2 = poor, 3 = good, 4 = very good, and 5 = excellent) with a minimum score of 9 and a maximum score of 45, and finally, the median was considered the cutoff point value for good and poor performance (Al-Ahmadi, 2009).
Operational Definition
WPV: Participants experienced at least one sort of assault in the workplace, such as physical violence, verbal abuse, bullying, or sexual harassment, in the past 12 months (Legesse et al., 2022).
Verbal abuse includes shouting at, insulting, and displaying a lack of regard for someone's value and dignity; therefore, nurses were asked if they had experienced any of the verbally abusive behaviors listed from four distinct sources (coworkers, patients, and patients’ families) in the past 12 months (Weldehawaryat et al., 2020).
Physical violence: punching, biting, hurling things, strangling, pushing around, kicking, dragging on the floor, pushing against the wall, beating with a stick, and threatening an individual with a gun, knife, or any other type of weapon in the past 12 months (Weldehawaryat et al., 2020).
Sexual harassment: attempts to initiate or force sexual relations, threats to have sex (sexual blackmail), and giving money, gifts, or privileges in exchange for sexual favors are all examples of sexual harassment in the past 12 months (Weldehawaryat et al., 2020).
Work performance: nine items on a 5-point Likert scale ranging from strongly disagreeing (1 point) to strongly agreeing (5 points) were used to measure work performance. Accordingly, good work performance was defined as a score that is greater than or equal to the mean value, and poor work performance was defined as a score that is less than the mean value (Al-Ahmadi et al., 2009).
Statistical Analysis and Data Quality Management
The tool has been translated into the local Amharic language. Thirteen data collectors and four supervisors were trained, and a pre-test was conducted. The data collection procedure was done at the same time in selected public hospitals. Furthermore, the respondents were asked whether they had been interviewed previously or not to prevent contamination of data across the selected hospitals nurses. The data was cleaned, encoded, and entered into Epi-Data software version 4.7 before being exported to SPSS version 26 for analysis. WPV was calculated and assessed using descriptive statistics. A bivariable logistic regression analysis was performed to select variables for multivariable analysis. Then, after doing a multivariable analysis, a variable was deemed statistically significant if its p-value was less than .05. The adjusted odds ratio (AOR) with its 95% confidence interval (CI) was used to demonstrate the strength of association between each explanatory variable and the outcome variable.
Ethical Consideration
Wollo University College of Medicine and Health Science vetted and approved the study procedures (WU/CMHS/756/2022), and ethical approval was obtained. Government hospitals in eastern Amhara also provided explicit consent letters. Having fully understood the purpose of the study, each respondent provided written consent prior to the interview. In addition, the study was carried out in line with the Declaration of Helsinki. Recalcitrant study participants were excluded from the survey. Anonymized data was collected, and participant information was kept confidential.
Result
Of the total of 568 nurses working in the 14 government hospitals in South Wollo, 534 respondents were enrolled, making the response rate 94%.
Socio-Demographic and Life Habit Properties of the Study Subject
More than half of the total participants, 295 (55.2%), were female. The average age of respondents was 30.80 (SD ± 5.8) years old, with 358 (67.0%) being under the age of 30. More than half of the respondents, 315 (59.0%), were married. Moreover, 90 (16.9%) of respondents were current alcoholic drinkers, while 69 (12.9%) were current chat users (Table 1).
Socio-Demographic Characteristics of Nurses Working in Public Hospitals in Northeastern, Ethiopia, 2022 (n = 534).

Note. Others* = Catholic, Osho; Others = **Afar, Tigre.
Educational and Work Experience Related Properties
In terms of present hospital roles, 462 (86.5%) of the total respondents were ordinary nurses. In terms of educational attainment, 374 (70.0%) of nurses had a BSc degree, and just 20 (3.7%) had a master's degree. Almost three-quarters (390) of the participants worked in the night shift. The respondents’ job experience ranged from 6 to 38 years, with a mean of 9.74 (SD ± 5.95) years, and 196 (36.7%) worked for 6 to 10 years (Table 2).
Educational and Work Experience-Related Properties of Nurses Working in Public Hospitals in Northeastern, Ethiopia, 2022 (n = 534).
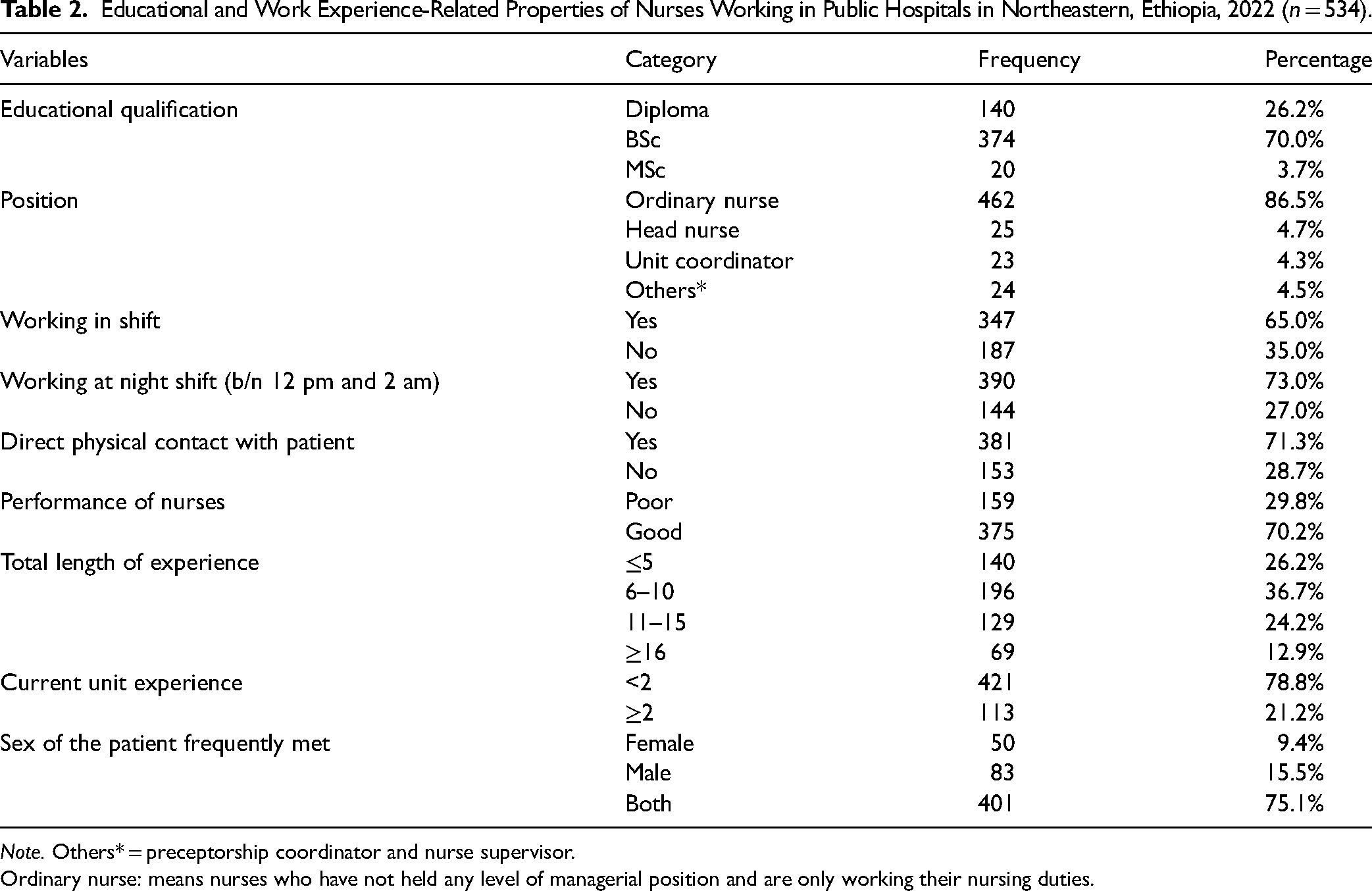
Note. Others* = preceptorship coordinator and nurse supervisor.
Ordinary nurse: means nurses who have not held any level of managerial position and are only working their nursing duties.
Prevalence of Workplace Violence
In the last 12 months, 299 (56%) of the participants had encountered at least one episode of various forms of WPV (verbal, physical, bullying, and sexual). Of the total participants who experienced work place violence, 112 (21%) reported physical assault, approximately 264 (49% of the total) reported verbal abuse, 93 (17.2%) claimed bullying, and 40 (7.5%) reported sexual harassment (Figure 2).
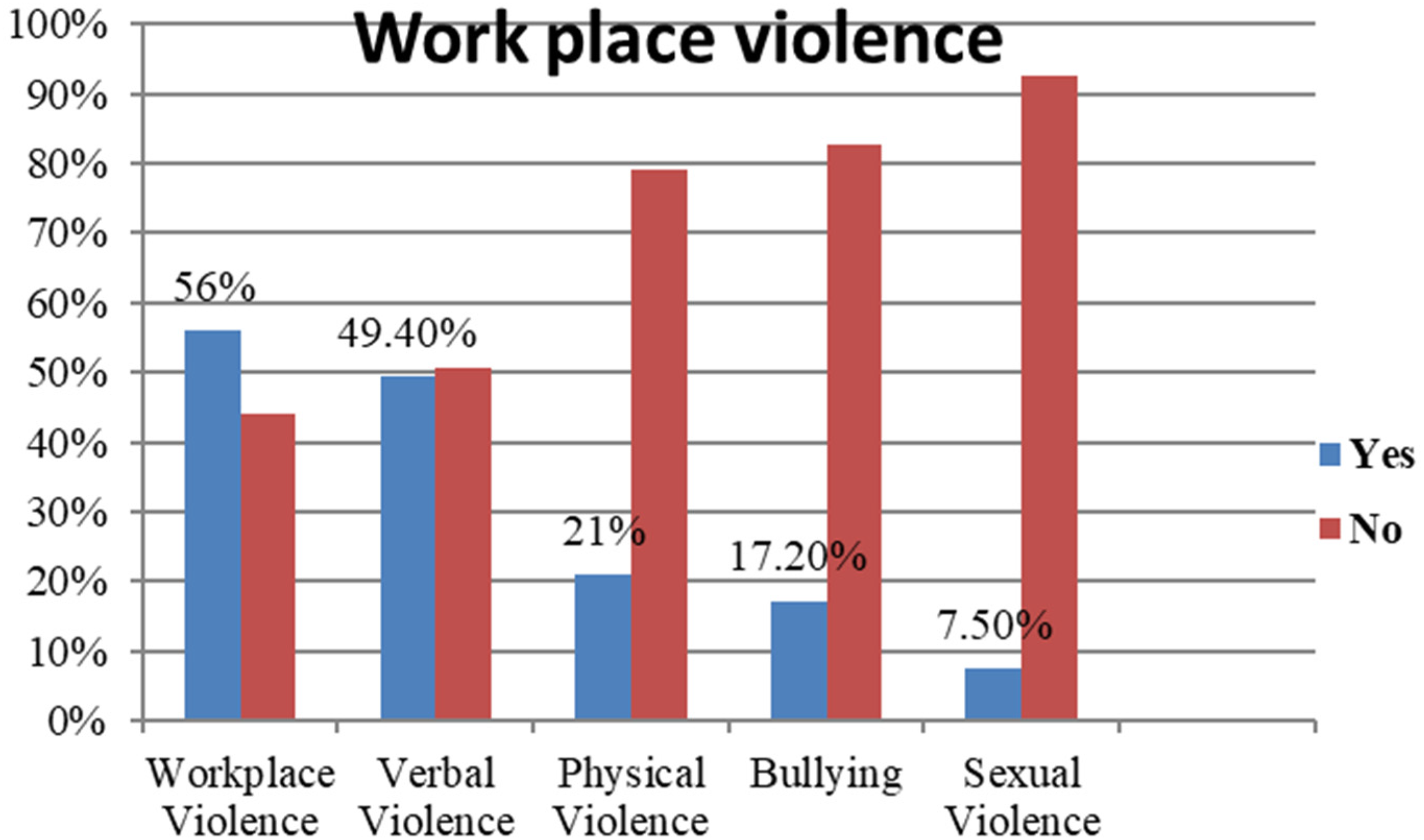
Work place violence among nurses working in public hospitals in Northeastern, Ethiopia, 2022 (n = 534).
Characteristics of the Individual Who Assaults Nurses
From the total verbal violence, 116 (43.9%) were committed by relatives of patients; from the total participants who were physically violated, 59 (52.7%) nurses were attacked by relatives of patients; from the total bullying, 40 (43%) were committed by relatives of patients; and from the total sexual violence, 13 (34%) of the participants experienced sexual harassment at work from a staff member (Table 3).
Characteristics of the Person who Assaults Nurses Working in Public Hospitals in Northeastern, Ethiopia, 2022 (n = 534).

Note. Others* = hospital managers, relatives of patients and general public; Others** = hospital managers, external colleague and general public.
Place Where the Violence Takes Place
About 249 (94.3%) verbal abuse incidents, 97 (86.6%) physical abuse incidents, 76 (81.7%) bullying incidents, and around 32 (80%) of the violent episodes occurred inside the hospital.
Prevention of Work Place Violence
In terms of WPV prevention, 137 (51.8%) verbally abused participants, 72 (64.2%) physically abused participants, and 24 (60.0%) sexually abused participants believed that the incidence was preventable.
Victims’ Reactions to Violent Situations
From 534 participants, 264 (49.5%) reported verbal abuse, and the remaining 270 (50.6%) indicated that they had not been abused; when they got it, they responded differently, with 174 (64.9%) taking no action. Furthermore, 21 (8%) were advised to halt their actions, 16 (6.1%) pretended it never happened, 13 (4.9%) reported it to senior staff members, 8 (3%) informed their friends or families, 7 (2.7%) sought counseling, and 5 (1.9%) attempted to defend themselves. Likewise, of the total number of physical attacks, only 112 (21%) were reported. When they were physically attacked, the majority of them (51%) did nothing. Besides, 16 (14.4%) participants tried to pretend it never happened, 9 (8.1%) were told to stop what they were doing, 19 (17.1%) tried to defend themselves, 5 (4.5%) informed their friends or family, and 3 (2.7%) informed senior staff members. Regarding sexual violence, only 40 (7.5%) of the 534 participants reported sexual harassment. When they were attacked, the bulk of them (19, or 47.5%) did nothing, and seven (17.5%) were told to stop their actions; four (10%) pretended it never happened; four (10%) reported it to senior staff members, and two (5%) sought counseling.
Factors Associated With Workplace Violence
Only six variables (sex, age, current alcohol drinkers, lifetime alcohol consumption, current khat chewers, and the sex of the patient frequently treated) were found to be significantly associated with WPV after all variables were entered into a multivariable logistic regression. Female nurses were approximately five times more likely to encounter WPV than male nurses [AOR = 4.85, 95% CI (3.178, 7.412)]. Besides, nurses over the age of 41 were approximately three times more likely to be subjected to WPV than nurses under the age of 30 [AOR = 2.27, 95% CI (1.101, 4.701)]. Nurses who were current or previous alcohol users were approximately eight and three times more likely to experience WPV than those who did not drink alcohol [AOR = 7.94, 95% CI (3.027, 20.86)] and [AOR = 3.14, 95% CI (1.328, 7.435)]. Furthermore, nurses who had contact with male patients were at least five times more likely to experience WPV than nurses who had contact with both sexes [AOR = 4.84, 95% CI (2.496, 9.415)] (Table 4).
Factors Associated With Workplace Violence Among Nurses Working in Public Hospitals in Northeastern, Ethiopia, 2022 (n = 534).

Note. *Statistically significant at p < .05 in COR; **Statistically significant at p < .05 in AOR.
Discussion
According to the study, the magnitude of WPV among nurses was 56% (95% CI, 51.8 60.2). Furthermore, the sex of the nurse, the age of the nurse, alcohol drinking, khat chewing, and the sex of the patients were predictors of WPV.
The present level of WPV among nurses working in public hospitals in northeastern Ethiopia is consistent with the results of a Nigerian study (53.5%) (Abodunrin et al., 2014) and 64.1% in eastern Ethiopia (Legesse et al., 2022). However, this study's findings were greater than those of previous studies in Hawassa City Administration, Southern Ethiopia (29.9%) (Fute et al., 2015), Northwest Ethiopia (26.7%) (Tiruneh et al., 2016), and Gamo Gofa (43.1%) (Weldehawaryat et al., 2020). The difference might be due to the operational definition of WPV used in the study in Hawassa, which used the last 6 months to define WPV, whereas this study utilized the last 12 months to define WPV. The study in northwest Ethiopia, Gondar, was conducted among health care workers and included only three types of violence (verbal, physical, and sexual) but excluded bullying, which may reduce the prevalence of WPV. The study in Gamo Gofa zone, Ethiopia, on the other hand, included hospitals, health centers, and health posts, which may have an impact on the setting as well as study subject characteristics discrepancies.
However, the findings of this study are lower than those of previous studies conducted in Palestine (80.4%) (Kitaneh et al., 2012), Nigeria (69.4%) (Douglas et al., 2019), and Oromia (82.2%) (Likassa et al., 2017). This could be due to the fact that in Palestine and Nigeria, the number of hospitals and hospital residence types involved in the study was limited to one and only in major cities. The same is true for the Oromia region, where only referral hospitals with residences in big cities were involved in the study. Those higher-level hospitals in big cities serve many people, and the setting is somehow different in type of service (referral), has a large number of staff, is congested with visitors, has a resident clinician, and has a medical student. As a result, the nurse has a higher chance of getting any type of WPV in this situation. On the other hand, the current study involved more hospitals in terms of number and settings (both rural and urban hospitals), where most of them are located in rural settings, have a lower number of medical staff, and serve a more culturally conservative society when compared to the above-mentioned studies. Therefore, the WPV might be lower than the above-mentioned studies.
According to the current study, 21% of participants were subjected to physical violence, about 49.4% were subjected to verbal abuse, and 40 (7.5%) were sexually harassed. This study's findings were lower when compared to a study conducted among nurses in public health institutions in Hawassa, which found that physical violence accounted for 18.22%, verbal abuse accounted for 89.58%, and sexual harassment accounted for 13.02% (Fute et al., 2015). This could be due to the nature of the hospital setting in Hawassa, where a tertiary hospital is congested with medical students, visitors, patients, staff, and resident clinicians, making it difficult to manage violence prevention tactics and proper safety measures. As a result, the incidence of WPV against nurses might be slightly higher than the current study.
In this study, verbal abuse was found to be the most common type of WPV, which is consistent with other studies conducted in different nations (Duma et al., 2016; Likassa et al., 2017; Magnavita et al., 2012). This could be because verbal abuse is simple for perpetrators to commit and, most of the time, does not leave the victim with tangible evidence to pursue legal action. This study also found, as in many other investigations, that patient family and patients were commonly cited as the primary sources of violence (Fute et al., 2015; Likassa et al., 2017). This could be because patients and patient relatives interact with nurses in stressful situations.
In the current study, the gender of the study participants had a significant relationship with WPV; female nurses were more likely to experience WPV than male nurses. This is consistent with research undertaken in Jordan (Albashtawy et al., 2013), Palestine (Kitaneh et al., 2012), and Hawassa (Fute et al., 2015). This could be explained as owing to a negative communal attitude regarding female power and aptitude, as well as the traditional thought that men are at the top of the hierarchical structure and are superior to female.
Furthermore, nurses who chewed khat were approximately three times more likely to be exposed to WPV than those who did not chew khat. This is consistent with research undertaken in Gamo Goffa (Weldehawaryat et al., 2020) and Oromia (Likassa et al., 2017). This is possible because such narcotics may cause individuals to perform their duties clumsily, allowing others to attempt to perpetrate violence against them. Or it could be that in most small towns, nurses’ personal lives are not disguised, and culturally, people drink alcohol.
This study also discovered that the age of nurses was linked to WPV. Nurses over the age of 41 were three times more likely to face WPV than nurses under the age of 30. This finding is consistent with findings from other studies conducted in both industrialized and developing countries (Fute et al., 2015; Magnavita et al., 2012; Weldehawaryat et al., 2020). Nurses’ vulnerability to WPV may grow as they get older, because older people may not have as much energy and strength to deal with it as younger or less-aged people.
Strengths and Limitations
The researchers used the Switchboard, a peer-reviewed and validated survey tool, and worked with more than 13 public hospitals. However, this study may have methodological flaws, such as a self-administered questionnaire, which may lead to respondent bias through overestimation or underestimation of the result. Furthermore, due to the nature of the study design, we were unable to establish a causal relationship. Therefore, conducting observational-based follow-up studies and qualitative studies will address the current study's limitations.
Implication for Practice
In this study, WPV implies that it has an impact on front-line forces like nurses’ quality of life and the quality of services. More importantly, the health sector needs to establish a preventing and reporting system for WPV incidents involving medical personnel. The national occupational and safety measures policy and procedures should be revised to protect the existence of nursing professionalism, which is the key to survival. Furthermore, it implies that qualitative, criminal reporting, and consequence studies need to be conducted to know the experience and the actual nature of WPV in Ethiopia.
Conclusion
In this study, the magnitude of WPV among nurses was relatively high and needs immediate intervention. Furthermore, the sex of the nurse, the age of the nurse, alcohol drinking, khat chewing, and the sex of the patients were predictors of WPV. Therefore, hospital administrators must establish WPV especial committee for managing and controlling of WPV. They should also facilitate various training programs on WPV among nurses and nurse managers. Furthermore, nursing managers, nursing in-service training institutions, and the nursing association should all contribute to the development and approval of national occupational and safety measures for WPV. Intensive facility-based and community-based behavioral change health promotion activities on WPV should be done, with particular focus on nurses and patients.
Footnotes
Abbreviations
Acknowledgements
The authors are grateful to the medical directors and nurses at 13 public hospitals in the South Wollo Zone for their kind cooperation. They are also grateful to the data collectors and respondents to the study.
Author Contributions
The authors made valuable contributions to proposal writing, data collection, processing, analysis, and interpretation. The principal investigator and correspondent author, in particular, played an important role in manuscript writing, skeptically revising it for important academic subject matter, journal submission, providing official approval, and agreeing to be responsible for all aspects of the process.
Data Accessibility
Any data produced or reviewed as part of this study are included in the manuscript and are also readily accessible to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
Wollo University College of Medicine and Health Science vetted and approved the study procedures (WU/CMHS/756/2022), and ethical approval was obtained. Government hospitals in eastern Amhara also provided explicit consent letters. Having fully understood the purpose of the study, each respondent provided written consent prior to the interview. In addition, the study was carried out in line with the Declaration of Helsinki. Recalcitrant study participants were excluded from the survey. Anonymized data was collected, and participant information was kept confidential.