
Abstract
Background:
Although cervical cancer is the most prevalent cancer in women and has a high morbidity, mortality, and low quality of life burden among human immune virus-positive women, there is little evidence of it in northeastern Ethiopia.
Objective:
Sought to determine the magnitude and associated factors of cervical cancer screening among human immune virus-positive women in public health facilities in northeastern Ethiopia.
Methods and material:
A multicentered, institution-based cross-sectional study with 401 participants using the systematic random sampling technique was employed. The data was gathered through personal interviews and chart reviews. The predictors were established via multivariate logistic regression analysis.
Result:
The magnitude of cervical cancer screening was 19.2% (15.7%–22.9%). Multiparity, bad obstetric history, hearing about cervical cancer, recommendations from medical professionals, duration of antiretroviral therapy >10 years, a family record of cervical cancer, and knowing cervical cancer were revealed to be predictors of testing for cervical cancer.
Conclusion:
The magnitude of cervical cancer screening was 19.2% (15.7%–22.9%). Multiparity, bad obstetric history, hearing about cervical cancer, recommendations from medical professionals, duration of antiretroviral therapy >10 years, a family record of cervical cancer, and knowing cervical cancer were revealed to be predictors of testing for cervical cancer.
Keywords
Introduction
Cervical cancer (CC) is ranked as the fourth-highest cause of cancer in women globally, accounting for 604,000 new cases and 342,000 deaths in 2020. Of these, middle- and low-income countries will account for over 90% of new cases and deaths globally. 1 The annual number of new cases of CC is anticipated to climb from 570,000 to 700,000 between 2018 and 2030, with a yearly total of deaths climbing from 311,000 to 400,000. 2 More than 85% of those afflicted are young, illiterate women living in the world’s poorest countries. 2
The incidence, mortality, and prevalence of CC in Sub-Saharan Africa were 25.2%, 23.2%, and 27.6%, respectively. The incidence, mortality, and magnitude of CC in Ethiopia were 17.3%, 16.5%, and 18.2%, respectively. 3 CC is an issue of public importance in Ethiopia, as it is the second biggest cause of cancer-related death among women of reproductive age following breast cancer. 4 Furthermore, each year, CC is projected to impact 23% of Ethiopians for every 100,000 women. 5
CC is the most common cancer among women living with HIV (WLWHIV). WLWHIV have a higher risk of remaining infected with human papillomavirus (HPV) than HIV-negative women, and they are six times as likely to acquire CC 6 and have a greater chance of getting it at earlier ages.7,8 Moreover, the time it takes for CC to develop in women with weakened immune systems, such as those with HIV infection, can be slashed in half when compared to immunocompetent women. 1
Despite the fact that the WHO recommends CC screening and treatment 9 and that the UN stressed the importance of HIV/AIDS integrated services for dealing with coinfections and co-morbidities, such as CC screening, 10 only 30% of low-income nations stated that they had public-sector CC screening and management services, compared to more than 90% of high-income countries. Furthermore, only around one-fourth of low-income nations have included the HPV vaccination in their national vaccination programs. 1 In current studies in Ethiopia, such as Tigray, Gondar, Addis Abeba, and Adama, the uptake of CC screening among women living with HIV (WLHIV) was low and required more effort, with 8%, 10%, 25%, and 26.9%, respectively.11–14
Many studies have identified the following barriers to CC screening uptake: Sociodemographic factors such as age, educational level, and occupation; HIV and sexual behavior factors such as having several sexual partners, having a sexually transmitted disease (STI), getting started with sex at a young age, the duration since HIV diagnosis, and having a high HIV viral load; poor knowledge and unfavorable attitude-related factors; facility-related factors such as the inability and insufficient knowledge of medical personnel; the insufficient finances and expensive cost of screening; and a shortage of screening facilities.5,12,14–16
The WHO has established 90-70-90 goals that must be reached by 2030. By the age of 15, 90% of girls are fully vaccinated against HPV, 70% of women are tested, and 90% of women with CC receive medical care. 1 As a developing nation, Ethiopia adopted less expensive but more effective CC testing methods known as Visual Inspection with Acetate Acid (VIA). 17 From October 2009 to September 2014, under the project name “Addis Tesfa” “CC Prevention Initiative,” Pathfinder International Ethiopia implemented a one-visit strategy of VIA testing and cryotherapy of precancerous lesions for HIV+ women. 17 Moreover, the Ethiopian Ministry of Health intends to test and manage a minimum of 80% of the appropriate populations for CC by 2020. 18
Despite the fact that the study area includes numerous small towns with high HIV prevalence at the national level, the implementation of CC screening with WLWHIV findings is little recorded. Moreover, unlike other previous studies, it involves multi-center health facilities, increasing the representation issue. As a result, the current project assesses CC screening uptake and associated factors among WLHIV, filling the knowledge gap and providing potential recommendations for barriers to CC screening uptake for local health managers and care providers. This allows us to meet the 90-70-90 objective and enhances the quality of life for WLWHIV.
Methods
Study period and design
From November to December 2022, a multicenter facility-based cross-sectional study approach was used in public health facilities in northeastern Ethiopia. A total of 14 public hospitals, two comprehensive and specialized hospitals that provide specialty care, and three private general hospitals. However, public hospitals in this zone are expected to serve 5 million people. All public hospitals in northeastern Ethiopia offer ART and CC testing, and there are currently 31,000 HIV patients receiving ART in hospitals, with 14,649 of them being women aged 25–49.
Source of population
All HIV-positive women who were getting ART at public hospitals in northeastern Ethiopia were used as a source of population. However, randomly selected women living with HIV and receiving ART in selected public hospitals in northeastern Ethiopia were considered study units.
Inclusion and exclusion criteria
Women who were HIV-positive and receiving ART during the study period were included; however, women who were unable to communicate or were extremely ill during the data collection period were removed.
Sampling size determinations and sampling procedures
The sample size was calculated using a single population proportion formula. The following assumptions were considered: The magnitude of cervical screening in Hawassa town was 40.1%, 15 with a 95% level of confidence and a 5% margin of error. The overall sample size was expanded to 406 by including a 10% non-response rate.
The study included all 14 public hospitals in northeastern Ethiopia that provide ART and CC screening services. HIV-positive women getting ART were proportionally allocated throughout the hospitals. Finally, using the ART logbook as a sample frame, a systematic random sampling technique was applied to select study participants for every 38th client.
Data collection technique and instrument
The data were gathered via a pre-tested, structured interviewer-administered checklist and chart reviews derived from various literature15,19,20 while taking into account the particular circumstances of the project area and the aim of the study. To ensure uniformity, the questionnaire was initially composed in English and then transcribed into Amharic dialects before being rewritten back into English by a language specialist. The questionnaire is divided into five sections. Section one discusses sociodemographic parameters such as age, educational level, occupation, and place of residence. The second component addressed sexual and reproductive health variables such as sexual history, menstruation pattern, family planning, parity, and CC history. Section three gathered HIV-related information such as duration of HIV infection, duration of ART, viral load, HIV status of partners, and history of STIs and collected through chart reviews. Part four discussed CC screening knowledge and attitude, while the final portion addressed CC screening uptake (Supplemental file 1).
Operational definition
Uptake of CC screening: When a woman living with HIV self-reports that she underwent a test for CC during the last 5 years. 21
Bad obstetrics history: Defined as participants who have any stillbirth, abortion, or early neonatal death. 22
CC screening attitude: Participants who responded to the CC screening-related attitude question above the median were considered to have a favorable attitude, whereas those below the median had an unfavorable attitude toward CC screening. 21
CC screening knowledge: Of the total six knowledge-based questions, participants who got a correct response at least three and above were considered to have good knowledge, whereas those who got a correct response below three had poor knowledge about CC screening. 21
Data quality management and statistical analysis
The tool validity was assured in the prior studies.15,19,20,23 Fourteen data collectors and four supervisors were trained, and a pre-test of 5% of the sample size was performed with a Cronbach alpha of 0.87, indicating that the instrument was reliable. Fourteen oncology nurses and four medical doctors were hired as data collectors and supervisors, respectively, after training was given. After being cleaned, encoded, and input into Epi-Data version IBM SPSS Statistics Version 26, the data were exported to for further analysis. Descriptive statistics were employed to determine the magnitude of CC screening. In order to identify candidate factors and determine whether a crude relationship existed, bivariate analysis was performed; variables with p-values less than 0.25 were included in the final mode. A variable was then considered statistically significant if its p-value was less than 0.05 following a multivariable analysis. A 95% confidence interval-based adjusted odds ratio was utilized to illustrate the degree of association between every explanatory factor and the dependent variable.
Ethical approval and consent to participate
In November 2022, the ALKAN Health Sciences Business and Technology Research Ethics Committee evaluated and accepted the study protocols (3302/0347/22) and got ethical approval. Then, explicit authorization letters were also supplied by public hospitals in Northeast Ethiopia. Prior to the interviews, each respondent supplied a written agreement after fully understanding the goal of the study. Moreover, an indicator fingerprint was taken as a signature for those illiterate participants after they fully comprehended the aim of the study. Furthermore, the research was conducted in accordance with the Helsinki Declaration. Participants who refused to participate in the study were barred from taking the survey. The data was obtained anonymously, and the data provided remained private.
Result
Sociodemographic profile of the participants
The study involved 401 respondents in total, yielding a response rate of 98.7%. The median age of the respondents was 35.01 (SD 5.94) years, and 298 (74.3%) of the participants were between the ages of 25 and 40. The vast majority of participants, 262 (65.3%), were urban dwellers, with 204 (50.9%) being single (Table 1).
HIV-positive women’s sociodemographic profile who visit ART clinics in public health facilities in northeastern Ethiopia, 2022 (n = 401).

Sexual and reproductive characteristics of the study subject
The vast majority of participants (207, or 51.8%) began having sex after reaching the age of 18, 337 (84%) had a normal menstrual cycle, 298 (74.3%) are or have been using contraception, and 251 (62.6%) were primipara. In addition, the majority of participants, 350 (76.1%), had no negative obstetric history, and 95.8% and 57.9%, respectively, had no family history of CC or gynecological problems (Table 2).
HIV-positive women’s sexual, reproductive, and HIV-related characteristics who visit ART clinics in public health facilities in northeastern Ethiopia, 2022 (n = 401).
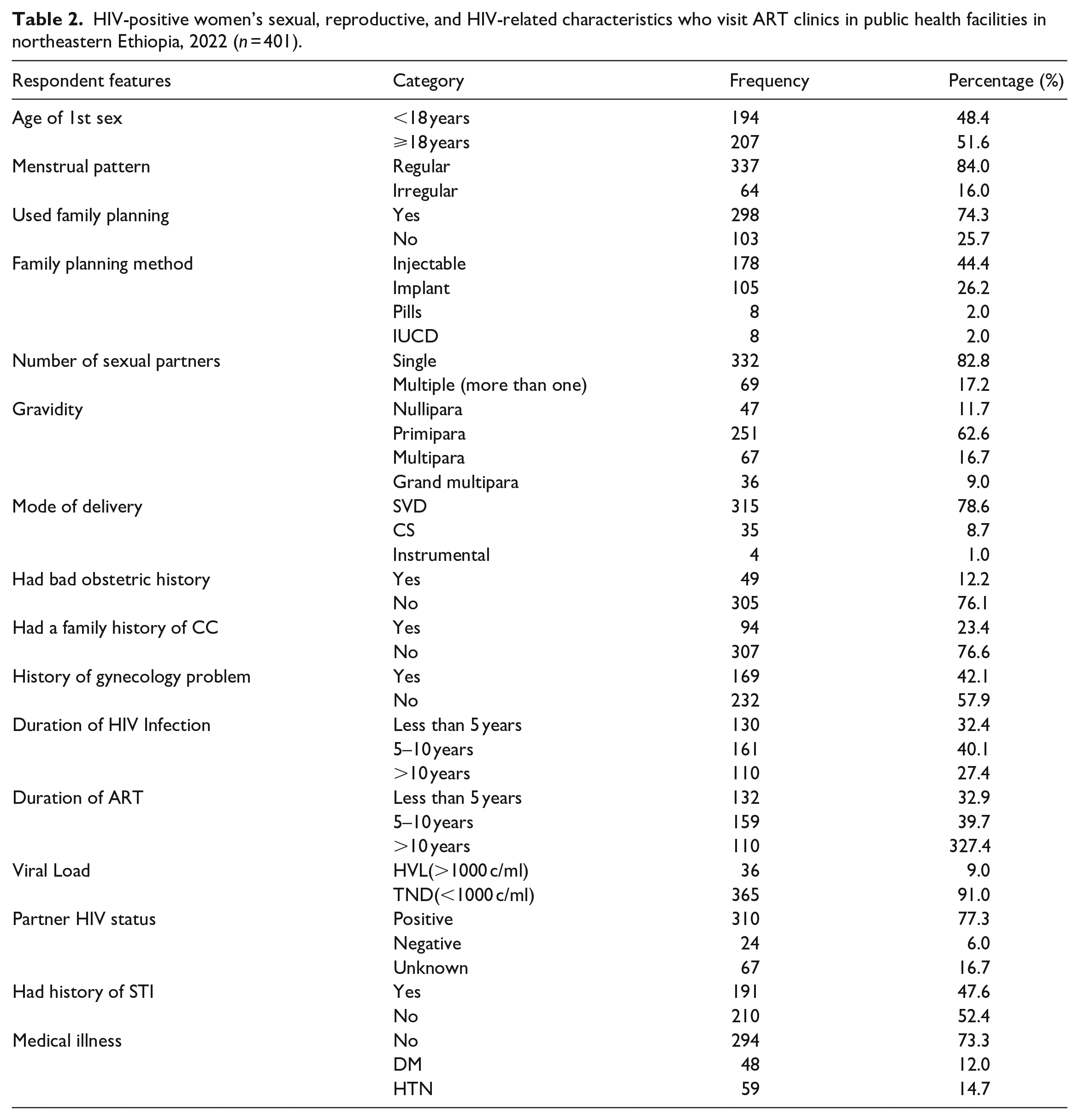
HIV-related characteristics of study subject
This study also looked at respondents’ HIV-related features. One hundred sixty-one (36.3%) of the respondents had been infected with HIV for 5–10 years. In terms of ART duration, 159 (39.7%) of respondents had ART for 5–10 years. Moreover, approximately 365 (91%) of HIV patients have a suppressed viral load, and 77.3% of their partners have a positive HIV status. In terms of STI and medical disease history, 52.4% and 73.3% had no history of STI or medical or surgical disease, respectively (Table 2).
Knowledge and attitude about CC screening characteristics of study subject
From the total number of participants, 236 (58.9%) had a favorable attitude, and 218 (54.4%) had adequate knowledge about CC screening.
Uptake of CC screening
In the current study, the magnitude of CC screening among HIV-positive women visiting ART clinics was 19.4% (95% CI: 15.7%–22.9%) (Figure 1). Of these participants, most (72.2%) have been screened in the last year, and all of them were screened by VIA. The overall proportion of precancerous cancer among total participants who were screened for CC was 9.5%. From the total of 323 respondents who were not screened, about 80% of participants didn’t screen because of inaccessible advice, followed by a fear of screening (12%) (Figure 2).

HIV-positive women visiting ART clinics and their uptake of CC screening in public health facilities in northeastern Ethiopia, 2022 (n = 401).

Reasons for not being screened for CC among HIV-positive women visiting ART clinics in public health facilities in northeastern Ethiopia, 2022 (n = 401).
Predictors of uptake of CC screening
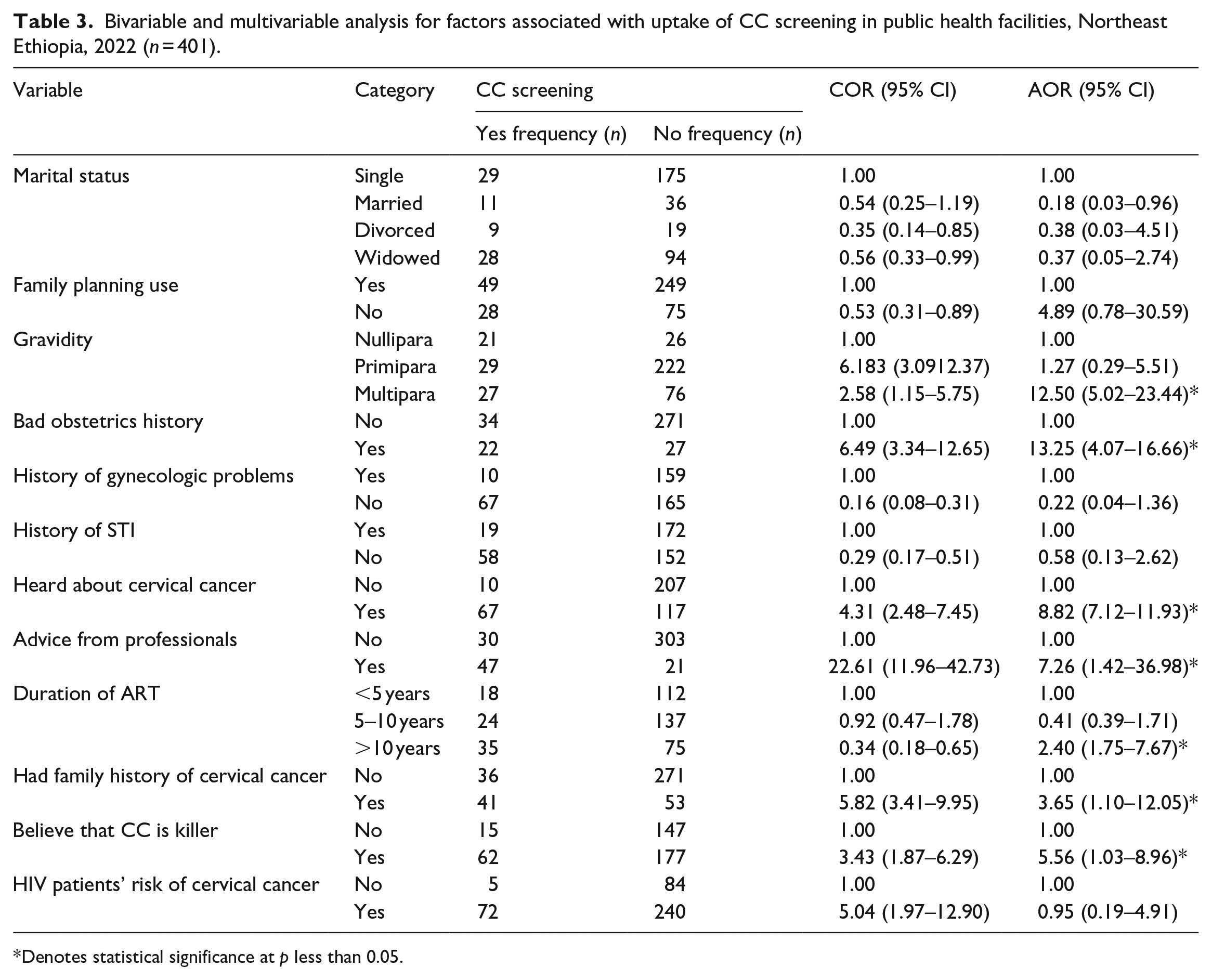
Only seven variables (gravity, bad obstetric history, professional advice, duration of ART, family history of CC, hearing about CC, and believing that CC is a killer) were found to be significantly associated with CC screening after all variables were entered into a multivariable logistic regression.
Compared to Nullipara women, Multipara women had a roughly 12-fold higher likelihood of using CC screening services (AOR = 12.50, 95% CI: 5.02–23.44). Women with bad obstetric history are roughly 13 times (AOR = 13.25, 95% CI: 4.07–16.66] more likely to use CC screening services than those without such a history. When compared to respondents whose HIV diagnosis was made less than ten years ago (<10 years), the odds of CC screening use were two times higher for those whose HIV diagnosis was made ten years or more (⩾10 years) (AOR = 2.40, 95% CI: 1.75–7.67). Moreover, HIV-positive women with a family history of CC had 3.6 times higher odds of being screened for the disease than did women without a family history (AOR = 3.65, 95% CI: 1.10–12.05). Women with HIV who receive professional advice are approximately seven times more likely to use CC screening services than women without such advice (AOR = 7.26, 95% CI: 1.42–36.98) (Table 3).
Bivariable and multivariable analysis for factors associated with uptake of CC screening in public health facilities, Northeast Ethiopia, 2022 (n = 401).
Denotes statistical significance at p less than 0.05.
Discussion
This study assessed the prevalence of CC screening and its associated variables among women who are HIV-positive and visit ART clinics in public hospitals located in northeastern Ethiopia. According to the current study, just 19.2% of HIV-positive women in public hospitals in northeastern Ethiopia had CC screening. This result exceeds that of two previous studies that were carried out in Gondar, northwest Ethiopia (10%), and Hawassa, southern Ethiopia (10%).12,15 It is, however, lower than in Addis Ababa (40.1%), Bishoftu, central Ethiopia (25%), and Northwest Ethiopia (23.5%).21,24 This difference might be due to the fact that study periods and sociodemographic disparities between places could be possible variances. The findings of this study were also explored in relation to worldwide situations. The result was significantly lower than the findings from Estonia (49.7%), Canada (25.9%), Thailand (73%), and Ghana (82%). The discrepancy might be due to the study subject’s sociodemographic and socioeconomic status, country income level, and level of health-care system differences.25–27
This study also looked into factors linked to CC. CC screening was found to be substantially associated with gravidity, a bad obstetric history, hearing about cervical cancer, expert guidance, the length of ART, and a family history of CC. This led the current study to show that women living with HIV who had a bad obstetric history were thirteen times more likely than their counterparts to have a CC screening. The findings are consistent with those of other African studies.28,29 This could be explained by the desire for children among women who are HIV-positive and have poor obstetric histories to be very sensitive and inspired to seek counseling, screen, vaccinate, and use medications to avoid recurrent negative outcomes. As a result, this makes them knowledgeable about CC, and this will enable them to do a cervical cancer screening as well.
Participants who were aware of CC were almost nine times more likely than those who weren’t to get screened for it. The results align with studies conducted in Mozambique 30 and Ethiopia.12–16 This could be explained by women living with HIV being eager to know about co-morbidities, including CC, and having the chance to hear or read about CC via the news, care providers, and even social media, which might result in them having adequate information. Once the woman had adequate information, she would likely seek counseling and be encouraged to undergo CC screening.
According to the findings of the current study, those who were multipara were almost 13 times more likely than nullipara to have CC screening uptake. This is comparable with studies in Gondar, northwest Ethiopia, and a systemic review of sub-Saharan Africa.12,16 This could be explained as women living with HIV may require numerous health-care visits for a variety of reasons, including pregnancy, prevention of mother-to-child HIV transmission, delivery, postnatal care, and immunization. Consequently, compared to those who were nulliparous the year before, they will be more likely to be tested for CC and will receive more information and counseling regarding CC screening.
The current study indicated that there was a roughly seven-fold increase in the likelihood of CC testing among women who received information from health-care providers compared to those who did not get advice. The results are consistent with previous research in Kenya and other systematic reviews.31,32 One way to illustrate this would be if someone were to learn about CC screening, their understanding and attitude about the screening would enhance, increasing their likelihood of screening for it.
Furthermore, the current study found that participants with a family history of CC were about four times more likely than their counterparts. This is due to the fact that those who have family members who have passed away from or are undergoing treatment for CC are more likely to have been subjected to fear and comprehend the illness. This will encourage women to have CC screenings. The findings are congruent with those of a Ghanaian study. 33
In the current study, respondents who had been on ART for more than ten years were roughly twice as likely to screen for CC as those who had been on ART for less than 5 years. This conclusion is comparable with findings from Gondar in northwest Ethiopia and Hawassa in southern Ethiopia.12,15 The possible speculation is that long-term ART-using women living with HIV will have access to information on the value of cervical cancer screening, which may put pressure on them to get checked for CC.
According to the current study, women with HIV who were aware of the high death rate from cervical cancer were almost six times more likely to get screened for the CC than those who were not. The findings are consistent with studies from Addis Ababa, Ethiopia, and Asia.34,35 This could be because knowing that CC is a killer will push people to be screened.
Limitations and strengths of the study
Using a survey instrument that has undergone peer review and validation, the researchers included all 14 public hospitals within the study region. This study also made an effort to address a neglected but important public health issue by gathering data from original sources, especially in the study area. However, it would be challenging to establish a temporal relationship between the independent and outcome variables because of the nature of the study approach. Therefore, completing qualitative investigations and observational follow-up research will address the shortcomings of the current study.
Implication for practice
Health-care providers who treat HIV-positive women must inform and motivate them to get screened for CC on a regular basis. Developing models for the most effective CC campaign strategy and maybe incorporating screening into the HIV care continuum should be a major responsibility of the government and other relevant parties. One strategy to reduce the cancer burden is to systematically encourage the uptake of CC screenings. This ought to address things like the attitudes and knowledge of women who are HIV-positive. Programs for intervention should place a strong emphasis on knowledge expansion since it can influence practice and attitude. A better environment for health-seeking can be created by raising knowledge of CC and encouraging participation from all HIV-positive women, which will increase the use of screening programs.
Conclusion
According to the study, CC testing was not very common among women living with HIV and required more work in the study area. Lack of knowledge and fear of screening were the main reasons for the non-screening trend. Positive predictors of cervical cancer screening were multiparity, a bad obstetric history, hearing about cervical cancer, seeking professional guidance, ART for more than ten years, a family history of CC, and awareness that cervical cancer is deadly. Comprehensive behavioral modification programs through peer education that emphasize women with multiple children, a history of bad obstetrics, knowledge about cervical cancer, use of ART for more than 10 years, and a family history of CC as change agents will be strengthened. Additionally, throughout every visit, the caregivers’ role in CC screening counseling would be improved. The importance of CC screening and its hurdles will be further raised through local TV, radio, and other social media channels.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231225935 – Supplemental material for Uptake of cervical cancer screening and associated factors among human immune virus positive women attending antiretroviral therapy clinic in public health facilities, Northeast Ethiopia, 2022: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121231225935 for Uptake of cervical cancer screening and associated factors among human immune virus positive women attending antiretroviral therapy clinic in public health facilities, Northeast Ethiopia, 2022: A cross-sectional study by Yemane Eshetu Bekalu, Muluken Amare Wudu and Amare Workie Gashu in SAGE Open Medicine
Footnotes
Acknowledgements
The authors of this paper are appreciative of the courteous assistance of the managers and staff at public health facilities in Northeast Ethiopia. We also feel appreciative of the research’s gatherers and participants.
Author’s contribution
The authors contributed significantly to proposal development, gathering information, processing, analysis, and interpretation. The primary investigator and correspondent author, especially, were crucial in article writing, skeptically revising it for significant academic topic issues, journal submission, granting official approval, and committing to be liable for all stages of the procedure.
Data accessibility and material
Any information generated or evaluated as part of this investigation has been incorporated in the publication and is also available to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.