
Abstract
Background
Antenatal care (ANC) is a care that could be provided to pregnant women by health professionals to uphold and maintain optimal health of women through pregnancy, labor, and puerperium period (1). ANC helps to provide basic preventive and therapeutic care, raise awareness on maternal danger signs, orient to birth preparedness, and improve health-seeking behavior of women (2–4).
Quality of health service is crucial at any time while the quality of ANC is important to increase utilization of other maternal health services (5–8). Good quality ANC service could increase client satisfaction (9,10). Similarly, it has a role to achieve health service goal that aimed at dropping maternal death (11) as evidences show that maternal death is high in countries where ANC coverage is low and where it has poor quality (10,12–15).
Delivery of good quality ANC service necessitates the presence of structures such as infrastructures, adequately trained health professionals, infection control facilities, diagnostic equipment, supplies and essential drugs, and appropriate utilization of guidelines (5–7). Conversely, the limitation of this prerequisite is continued to be challenging in Ethiopia. Research shows that physical infrastructures such as generator, waiting area, private examination room, couch in the ANC room, clean toilet, and water are either not available or nonfunctional. Furthermore, shortage and low qualification of health care providers, scarcity of equipment such as fetoscope, stethoscope, blood pressure apparatus, weight scale, ANC guideline, and thermometer are also not sufficiently available (16,17). In general, scarcity of the infrastructures leads ANC seeking women to be referred to private clinic (16). Additionally, gaps in structural readiness of health facilities, inadequacy of key essential supplies, unguaranteed properly equipped and staffed facilities leads to low quality of ANC services (18,19). Consequently, less satisfaction of the women and high dropout from the maternity continuum of care after ANC booking remained a public health problem in Ethiopia (16,19–22).
Moreover, traditional belief, delivering five and above children, high or low maternal age, ignorance, shyness/fear, long distance to health facility, educational status, history of stillbirth, and status of pregnancy are other ANC service use hindering factors in this country (23–25).
Consequently, improved access and better quality ANC service should be considered in Ethiopia (7,26–29) to contribute to the reduction in maternal death from 412/100,000 (30) to 70/100,000 by the end of the Sustainable Development Goals (SDGs) (26). For concerning bodies to take relevant action, availability of organized data-based information is important.
Previously, few studies had been carried out to assess the quality of ANC services in Ethiopia. Nevertheless, the majority of these studies were focused on town and higher-level health institutions. The remaining studies were conducted at higher facilities such as university hospitals (31,32). This study is different in addressing the rural public health facilities where more than three-fourths of Ethiopian populations live (33). It was also conducted using the Donabedian quality-of-care framework by incorporating the three dimensions of health service quality assessment; the structure, process, and outcome (34). It had also added some values; the client satisfaction where it could help to recommend on patient-centered care which is one of the pioneering points to improve the quality of health care services (35).
Methodology
Study Area and Period
Facility-based cross-sectional study was conducted from March 11 to April 19, 2019 at Bele Gasgar Dstrict which is located at 272 km to Southeast from the capital city of Ethiopia. The district had four public health facilities. As it is recommended by World Health Organization to conduct a facility census in the study area where it is small, all the available health facilities were included in this study (36).
Sample Size Determination
Required sample was calculated using Epi Info version 7.1, considering 60.4% proportion of client satisfaction among ANC users (37) in Jimma town, 95% level of confidence interval and error of margin 5%. Finite population correction was done since source population, the ANC users in the district from preceding year was 3,572 < 10,000. For nonresponse, 10% of the sample was added and the final sample size became 366.
Participant Requirement
Primarily, a list of ANC utilizing women was taken from their registry at Bele Gasgar District Health Office to frame for sampling system. A total of 366 samples were distributed proportionally to all available public health centers (3 health centers and 1 district hospital). Computer-based randomization was done to pick individual women for the interview.
Data Collection Tool and Method
Data collection tool was adapted from “WHO survive availability and readiness assessment (SARA)”(36), “WHO Inventory tool for maternal health supplies(ITMHS)”(38), “Ethiopian standard agency health center requirement (ESA)”(39), “Inventory tool for maternal health supplies (ITMHS)”(38), and other related literatures (17,31,38). The tool for client satisfaction was adapted from the study performed in Bahir Dar town, Ethiopia (31). All the interview tools were prepared in English and translated into the local language Afan Oromo and back to English by two language experts independently.
Data of the availability and functionality of infrastructure and manpower were collected by observation using a resource inventory checklist. Data on the types of ANC visits and client satisfaction were collected through exit interviews at health facilities. Furthermore, 80 pregnant women and ANC service providers were observed for the health care provider and client interaction.
Measurements
Structure was measured using five items (39); presence of health professionals, availability of infrastructures, accessible and functionality of basic equipment, accessibility of essential drugs, and availability of laboratory. The overall structure quality attributes were measured against the standard of yes answer ≥75% to the inventory checklists (36).
Process was measured using the participants’ response to service provision questions and observation of consultation sessions. Moreover, client satisfaction was assessed with 5-point Likert scale. During analysis, strongly agree and agree responses were classified as “satisfied” while strongly disagree, disagree, and neutral were classified as “not satisfied”. Neutral responses were classified as not satisfied considering that it might represent a fear of expressing dissatisfaction since the interview was done within the health facilities (31). Client satisfaction of less than mean point was categorized as “under satisfied” whereas mean point and above was categorized as “satisfied”. Generally, the overall quality of ANC was measured from the summation of these three components using 75% as a cut-off point, where the presence of 75% or more of the recommended components of care indicator items was categorized as “good quality of ANC”.
Data Analysis
Double data entry was done in EpiData Manager version 4.4. The data were analyzed using SPSS version 23.0. Descriptive statistics was done to summarize participants’ characteristics. Principal component analysis was done for the overall structure quality attributes of the process. Multicollinearity was checked using variance inflation factor. Cox and Snell, Nagelkerke chi squares, as well as Hosmer and Lemeshow test for model adequacy were checked and all results were with a benchmark. Bivariate logistic regression analysis was carried out to select candidate variables for multivariable logistic regression at p-value <.25. Backward stepwise likelihood logistic regression model was constructed to identify factors associated with client satisfaction. AOR, p-value <.05 with 95% CI was used to report the association.
Result
Sociodemographic and Obstetric History of the Respondents
A total of 360 pregnant women participated in the study making a response rate of 98.4%. The mean age of participants was 25.61 years (SD ± 5.05) while their mean traveling time was 60 min (SD ± 7.7 min) (Table 1).
Distribution of Sociodemographic and Obstetric Characteristics of Respondents.

Abbreviation: ANC, antenatal care.
Structure Attributes
All ANC service delivery points were equipped with necessary equipment such as weight scale, fetoscope, safety box, high-level disinfectant and alcohol, clean and surgical glove, focused antenatal care (FANC) card, registration logbook, examination couch, and sterilizer. Nevertheless, only two health facilities had measuring tape for the ANC unit where others were using finger method to measure fundal height. One health facility was sharing a thermometer with all other units available at that facility. Three health facilities had standing light or torch. None of the health facilities had working ANC guidelines.
Regarding the availability of essential drug supplies, drugs such as amoxicillin, penicillin, iron or folic acid, or both tablet and tetanus toxoid vaccine were available in all health facilities and distributed for free on working days. Two health facilities had sulfadoxine pyrimethamine while three facilities had magnesium sulphate and aldomate. Two facilities had TDF +3TC+ EFV for prevention of mother to child transmission of HIV where the remaining two facilitiessend HIV positive women to the nearest hospital.
Concerning the laboratory services, 50% of all basic laboratory tests were available in all facilities. There was shortage of basic tests such as venereal disease research laboratory test (VDRL), urine analysis, blood group/Rhesus (Rh), hemoglobin/hematocrit (HCT), and stool examination in two facilities.
All health facilities had private rooms and ambulances. Two facilities had no water supply in the examination room and one facility had no electric supply. Three facilities had waiting areas though only one facility had a clean toilet.
On the other hand, none of the health facilities had fulfilled the minimum requirement of the standard health care provider. There were shortage of laboratory technologist/technical and pharmacist/druggist highly.
In general, the overall structure quality attributes was 71.4%, where 18 (64%) human resources, 30 (83%) essential drugs, 18 (75%) infrastructure, 51 (85%) basic equipment, and 10 (50%) basic laboratory tests were available (Table 2).
Distributions of Available Structure Quality Attributes in Antenatal Care (ANC) Services.
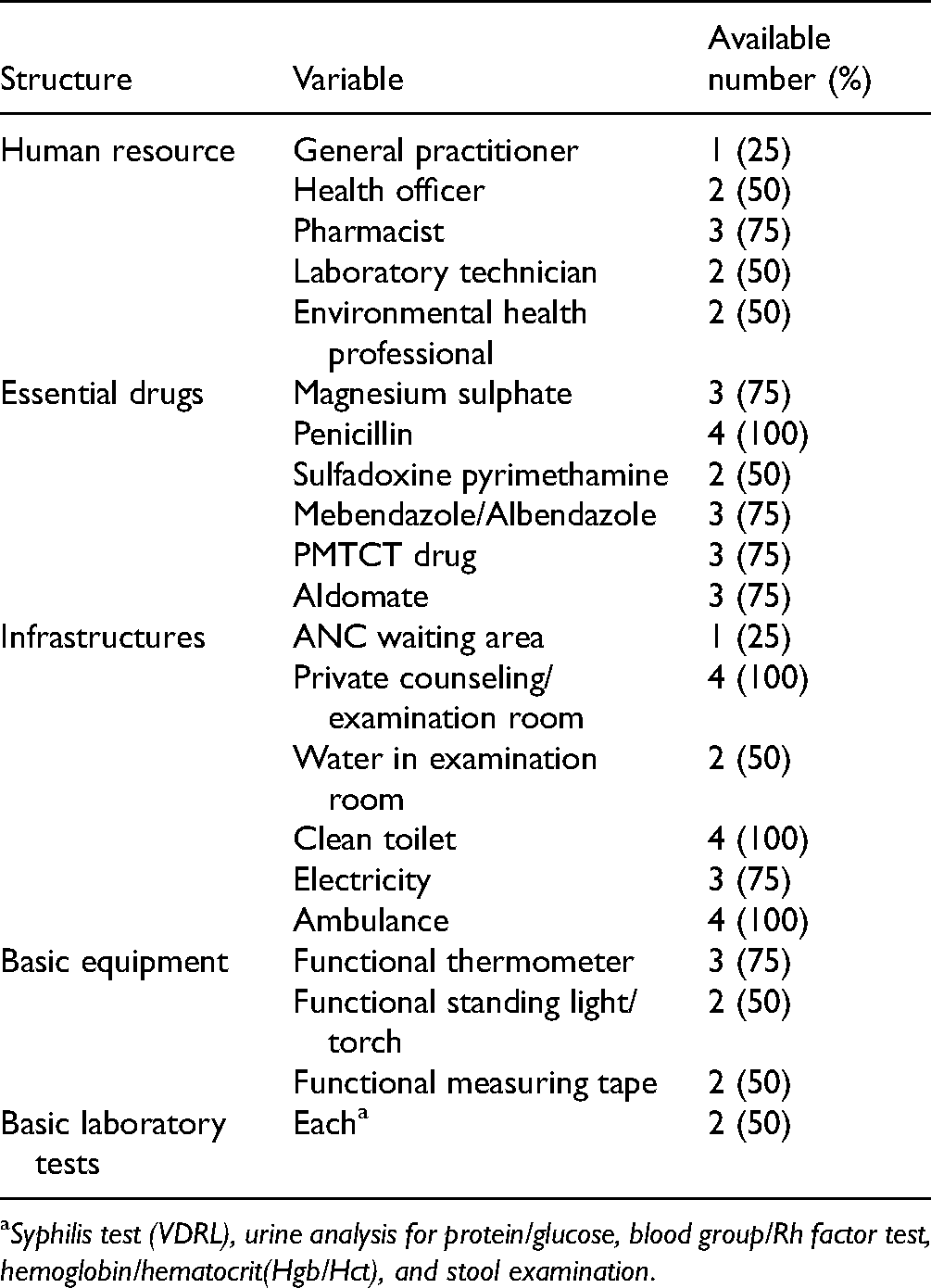
Syphilis test (VDRL), urine analysis for protein/glucose, blood group/Rh factor test, hemoglobin/hematocrit(Hgb/Hct), and stool examination.
Process Attribute
Almost all 356 (99%) respondents agreed that care providers treat them respectfully. During observation, only 2 (10%) of care providers introduced themselves to women where 90% got to history takingdirectly without greeting (Table 3).
Distributions of Process Quality Attribute of Interpersonal Aspect.

After principal component analysis (PCA) was done, 18 variables explained the whole variability of quality of ANC was 76.6%. Thus, the overall structure quality attributes of the process was 108 (30%) 95% CI = 25–35 (Figure 1).
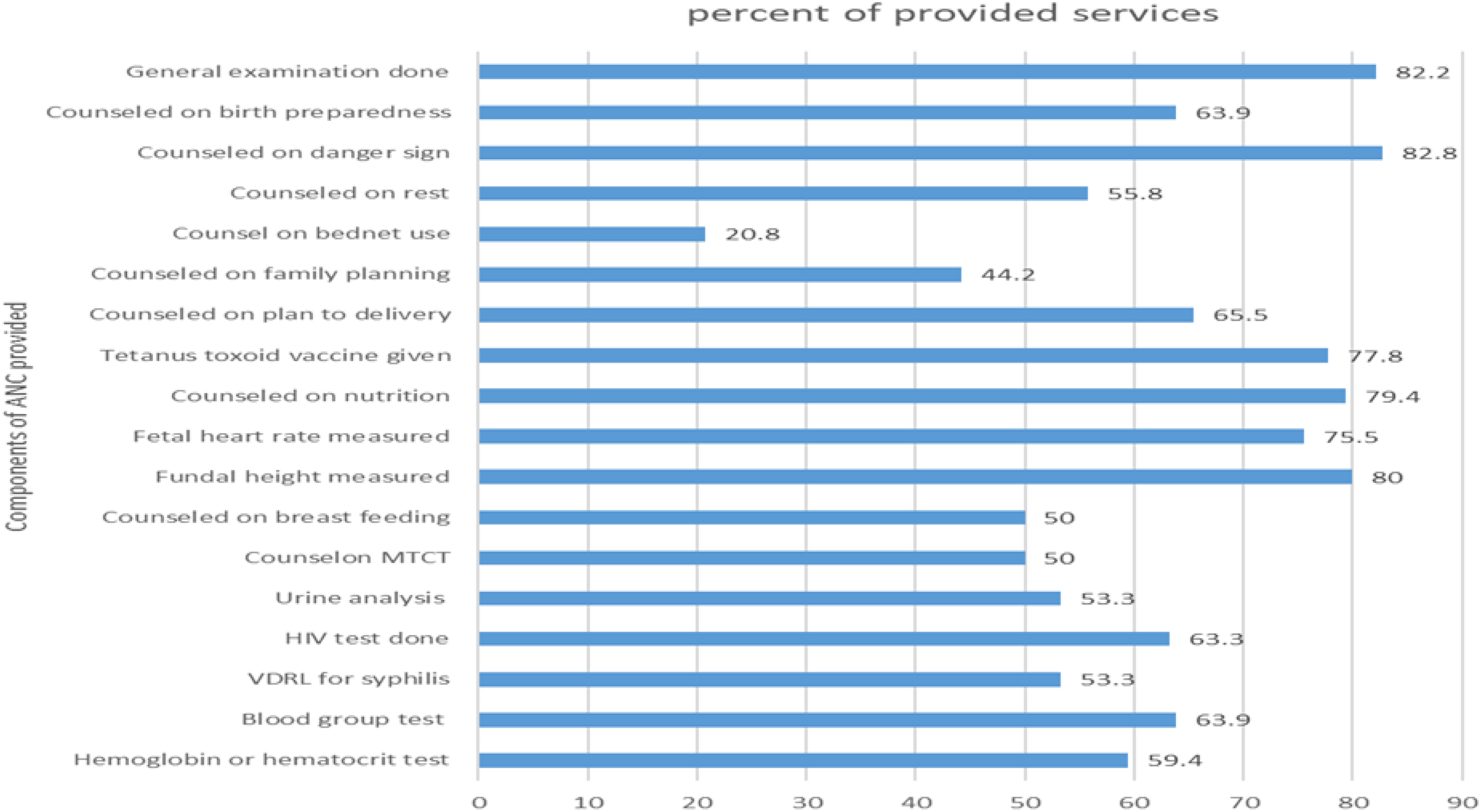
Components of antenatal care (ANC) services done at the four public health facilities.
Client Satisfaction
More than half 198 (55%), 95% CI = 50–60 of respondents were satisfied to the provided ANC service (Table 4).
Satisfaction Levels of Pregnant Women on ANC Services Received.
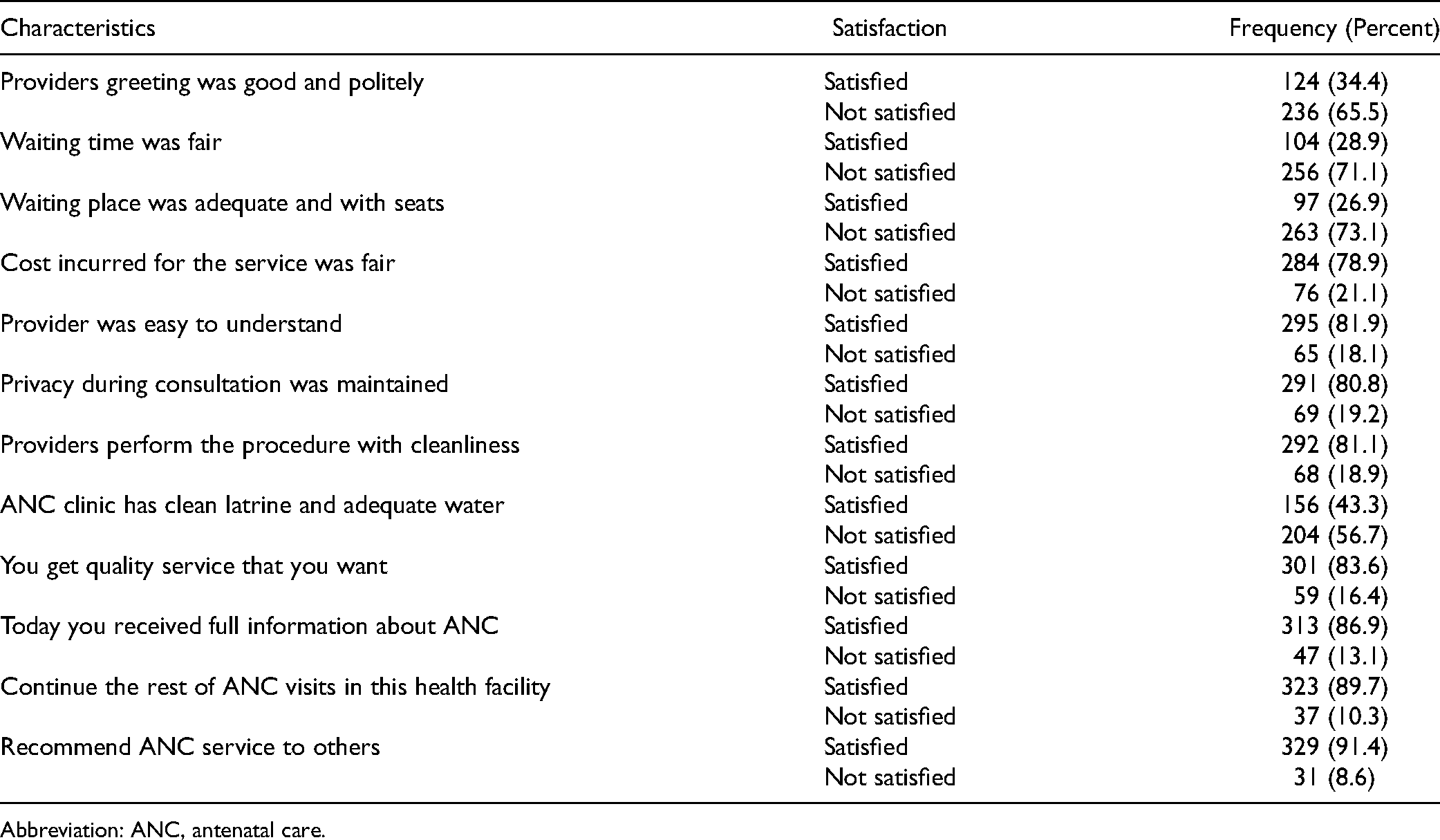
Abbreviation: ANC, antenatal care.
Factors Associated With Client Satisfaction
Multivariable logistic regression analysis showed that pregnant women who were provided iron pills during one of the visits were two times more likely (AOR = 2.23, 95% CI = 1.31−4.79) satisfied than those who were not provided iron at all. Women who were measured weight were three times more likely (AOR = 3.61, 95% CI = 1.40−9.31) satisfied compared to their counterparts. Women who traveled less than 60 min to reach the health facility were four times (AOR = 4, 95% CI = 2.3−8.16) and those who traveled between 60 and 1,200 min were almost four times more likely (AOR = 3.68, 95% CI = 1.61−8.38) satisfied than those who traveled more than 1,200 min. Similarly, women whose consultation time was less than 30 min were almost three times more likely (AOR = 2.89, 95% CI = 1.14−7.31) satisfied than those whose consultation time was 30 or more minutes. Moreover, pregnant mothers who were initiated to ask question on the service never were 80% times (AOR: 0.20, 95% CI = 0.08−0.45) and sometimes were 68% times less likely (AOR = 0.32, 95% CI = 0.16−0.65) satisfied than those who were usually initiated (Table 5).
Multivariable Logistic Regression of Factors Association with Client Satisfaction Level.

Crude odds ratio, b Adjusted odds ratio, c Prevention of mother-to-child transmission of HIV.
*Significantly associating at p-value <.5.
Discussion
Quality of Antenatal Care and Client Satisfaction
The overall quality of ANC was low 30% [95% CI = 25–35]. Comparable findings were reported in sub-Saharan Africa and Ethiopia (31,40,41). This low quality might be due to the focus of low-income countries on increasing coverage of the service rather than quality of the service (42,43). Additionally, low economic status of the areas and few in-services training to health professionals may also compromise quality of the service. Studies had identified that shortage of infrastructure causes poor quality in the health facilities of Ethiopia (31,40,44–46). It was indicated that poor infrastructures, inadequate skilled staff, stock-outs of consumables, and nonfunctional basic emergency obstetric care facilities are the leading factors of poor quality of maternal health service in less developed countries (18,19,47).
Furthermore, client satisfaction toward the given ANC service was moderately low 55% (95% CI = 50–60). This finding is consistent with the study done in Gondar, Chencha, Demba Gofa of Ethiopia, and in Kenya (17,48–50). Lower satisfaction could be resulted from the shortage of supplies, stocking out of essential drugs, lack of ANC waiting area, absent water supply, and electricity shortage in the facilities (48,51,52). Client and professional communication was poor in this study and this might also reduce client satisfaction.
Factors Associated With Client Satisfaction
Evidence shows that patient satisfaction is highly linked to the quality of services (13,15,53). Moderately low satisfaction in the current study is consistent with the study finding conducted in Jimma. However, it is lower than findings from studies conducted in Egypt and Nigeria, whereas higher than study findingconducted in Demba Gofa. The difference might be due to a subjective nature of the subject matter. Service satisfaction should be best measured with standardized scales and tools. Nevertheless, most of these studies had measured satisfaction using simple yes or no questions where clients’ response can be biased and lead to variation from place to place (17,27,37,54).
Pregnant women who were provided iron pills in one of the ANC visits were two times more likely satisfied than those who were not provided at all. This finding is different from the finding in Demba Gofa and Sierra Leone. The variation might be the difference in service provision status. Women need to charge for the supplies in other study areas while it is for free in this study area and free service couldincrease client satisfaction € (48,55). The significant association of this variable can be due to the high importance of iron/folic pills during pregnancy for both the mother and the neonate to reduce maternal complications and for organ development in the fetus (56). Women have this information before going for ANC as it is conveyed to them by health extension workers with the 16 health extension packages that are delivered home to home in Ethiopia (57).
Women whose weight was measured during one of the ANC visits were three times more likely satisfied than their counterparts. This finding is supportable with study results in China (58). This can be true due to its importance for women to monitor their weight during pregnancy.
Pregnant women who traveled less than 60 min to reach the health facility were four times and those who traveled between 60 and 1,200 min were almost four times more likely satisfied than those who traveled more than 1,200 min. This result is similar to the study in Harar and Kenya (45,49). High probability of satisfaction with less traveling time could be related to less time consumption. Women could be fatigued traveling for a long time and less satisfied with the health service.
Similarly, clients whose consultation time was less than 30 min were almost three times more likely satisfied than those whose consultation time was 30 or more minutes and this is similar with the study result in Bahir Dar, Kenya, and Kazakhstan. This might be due to the fact that pregnant women need short and easy information and want to go back home to their duties (31,49,59). On the other hand, women who were initiated to ask question on the service never were 80% and sometimes were 68% times less likely satisfied than those who were usually initiated. This can be because they may fear and get tensioned to explain their feeling as many of them were less educated.
In summary, poor quality of health services can worsen the low ANC utilization in Ethiopia. However, study in a single district may not be sufficient to explain quality of services where the authors recommend for study including more representative study areas.
Conclusion
The overall quality of ANC services in this study was found to be low. Consequently, this result should motivate policy makers to design interventions that could improve the quality of ANC service. Additionally, proportion of the clients who were satisfied with the service was moderately low, while satisfaction was positively associated with the provision of iron/folic acid pills, measured weight, shorter travel time, and shorter consultation time and negatively associated with health care provider-initiated client to ask question. Thus, the authors recommend the stakeholder should work on increasing the supply of medication, work on reducing traveling time by increasing nearest health facilities, and giving in-services training for health professionals. Further, it is recommended to produce a standard cut-off point to measure the quality of ANC and client satisfaction for low-income countries.
This study did not address customers’ self-audit on quality of services for which the authors like to recommend further study addressing this. Moreover, facility-based studies may overestimate client satisfaction and be better conducted in the community in the future.
Footnotes
Acknowledgments
The authors would like to acknowledge Jimma University and Bele Gasgar District Health Office for their invaluable support to accomplish this study.
Authors’ Contributions
MA conceptualized and designed the study, supervised data collection, conducted statistical analysis, and interpreted results. BT guided the study and analysis plan and the overall activities. BT prepared the manuscript. All authors approved the manuscript in its final form and have agreed to be accountable for all aspects of the study.
Availability of Data and Materials
All data that support the findings of this study are available in this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jimma University.
Ethical Approval and Consent of Participants
Ethical clearance was obtained from Jimma University Institute of Health Institutional Review Board (IRB). After objective of the study was clarified to the participants, informed verbal consent was obtained from all. Data collectors tick on the space provided in front of “yes I am willing to participate” and collected the data from volunteered participants. No personal identifier is used during data collection.
Statement of Human Animal Rights
All procedures in this study were conducted in accordance with the Jimma University Institute of Health Institutional Review Board's approved protocols
Statement of Informed Consent
Informed verbal consent was obtained from all study participants for their anonymized information to be published in this article.