
Abstract
Background. Burn is a major public health problem in pediatric populations worldwide. This study aimed to determine the survival status and predictors of mortality among pediatric burn victims admitted to burn centers in Ethiopia. Methods. A retrospective cohort study was conducted on the patient charts of 412 pediatric patients with burn injuries at burn centers in Addis Ababa from the 1st of January 2016 to the 30th of December 2019. Data was entered into the Epi-Data manager. Then, the data was exported to STATA V-14 for cleaning and analysis. For the analysis, the proportional hazard model was used. After the model fitness test, variables with a P-value of <.25 in the bivariate analysis were fitted to the multivariate analysis. Finally, statistical significance was decided at a P-value of <.05, and the hazard ratio was used to determine the strength of the association. Result. The study reported an overall incidence rate of 2.4 per 1000 child days. Additionally, it revealed that the median hospital length of stay was 25.00 days (95% CI: 21.57, 28.45). During the follow-up period, 8.25% of deaths occurred among pediatric patients with burn injuries. Specifically, having a full-thickness burn (adjusted hazard ratio [AHR] 2.51, 95% CI: 1.12, 5.62) and neck burn (AHR 2.82, 95% CI: 1.04, 7.68) were identified as significant predictors contributing to increased mortality among burn-injured pediatric individuals. Conclusion. The study highlighted significant mortality rates among pediatric patients suffering from burn injuries. Based on the findings a full-thickness burn injury and burns in the neck area are independent predictors of mortality in pediatric burn patients. Based on the identified predictors of mortality in pediatric burn patients, clinicians should prioritize early recognition, prompt intervention, multidisciplinary management, vigilant monitoring, and preventive strategies to optimize outcomes and reduce mortality rates in this vulnerable population.
Introduction
Burn is a common public health problem, encountering about 11 million yearly burn injuries.1,2 It is a common reason for pediatric hospitalization and the fourth most common type of trauma worldwide, after traffic accidents, falls, and interpersonal violence. 3 Globally, fire-related burns are a major public health problem; each year, they account for an estimated 265 000 deaths. 4 Childhood burns place a massive socio-economic burden on individuals, their families, and health services. 5
Death due to burn injuries in developing countries is estimated to be higher than in developed countries. 5 Pediatric burn injury mortality rates are 21.4% in the Gambia, 6 7.9% in South Africa, 7 and 27% in Central Malawi. 8 Burn injury remains a significant source of morbidity and mortality in developing countries, particularly in Ethiopia. 9 Burn injuries are common in Ethiopia, and a large proportion of the pediatric population suffers from this problem. 10 In Ethiopia, a single-site study found that 7.8% of burn victim children died. 11 The high mortality rate in pediatrics associated with burn injuries in Africa is challenging to the community. These challenges are apparent in Ethiopia, where burn care services and resources are limited.
The etiological classification of burn injuries is thermal burn, scalds, electric burn, and chemical burn. 12 Hot water, food, appliances, flames, grills, vehicle-related burns, and curling irons are common causes of burns. Death due to burn injuries in developing countries is estimated to be higher than in developed countries. 5 Previous studies reported that Pediatric burn patients died as a result of, shock, respiratory failure, sepsis, inhalation injuries, and Multi-organ failure.13,14 The extent of burn injury, nutritional status, causes of burn injury, depth of burn injury, age of the child, residency, condition at admission, and type of management given before and after admission were reported in different literature as significant causes for the poor progress of burned patients.3,6,8
Treatment of burn patients is expensive, complex, and resource-intensive. Burn patients may have long periods of rehabilitation and multiple outpatient visits after an initial period of acute care is given to them. 15 Due to the traumatic nature of the injury, survivors of severe burns have long-term physical and psychosocial consequences. 16 The majority of burn victims suffer from permanent disabilities, scars, and stigma; on the other hand, a greater proportion of mortality is seen in low and middle-income countries.17,18
Developed countries have conducted numerous studies focusing on pediatric burn populations. However, despite the wealth of research in developed nations, data are scarce regarding hospitalized pediatric patients with burn injuries, particularly concerning the outcomes, and factors associated with mortality. This gap in knowledge underscores the need for further investigation into this critical area. Therefore, the primary objective of this study was to assess the survival status and identify predictors of mortality among pediatric burn patients admitted to burn centers in Addis Ababa, Ethiopia. By addressing these gaps, the study aims to contribute valuable insights into improving the management and outcomes of pediatric burn injuries in these settings.
Methods
Study Design, Area, and Period
A retrospective cohort study was carried out on pediatric patients admitted to burn centers at Yekatit 12 Hospital Medical College and Addis Ababa Burn Emergency Trauma (AaBET) of St. Paul Millennium Medical College Hospital between January 1st, 2016, and December 30, 2019. Yekatit 12 Hospitals Medical College and Addis Ababa Burn Emergency Trauma (AaBET), located in the Addis Ababa regional state, are Ethiopia’s 2 largest hospitals providing burn care. The study was conducted from February 21 to July 6, 2019.
Study Population
The study population included all children less than 18 years of age who presented with burn injuries from the beginning of 2016 to the end of 2019 in burn care centers in Addis Ababa.
Eligibility Criteria
The study’s inclusion criteria encompassed pediatric burn victims under the age of 18 with complete and legible records. Moreover, cases with incomplete documentation or missing crucial information were excluded.
Operational Definition
Sample Size Determination and Sampling Procedure
The sample size was determined using a double proportional formula with a 95% confidence interval, a power of 80%, an unexposed to exposed case ratio of 1, and a percent of outcome in the unexposed group. A place of residence was 41%, and the percentage of outcomes in the exposed group was 27%, 19 yielding 391 after adding 10% of incomplete records to the total sample size, the required sample size was 423 (Table 1). From January 1st, 2016 to December 30th, 2019, 1040 pediatric patients were admitted to burn centers with burn injuries. The lists of medical records were obtained from the burn center registry and the liaison office reports. Using the medical records number (MRN) of the centers, we selected the first participants using lottery methods. Using proportional allocation, 214 pediatric charts were from Yekatit 12 Hospital Medical College, and 198 pediatric charts were from AaBET hospital. Hence, proportionally 423 burned pediatric patients’ charts were selected by using a systematic sampling method from the HMIS registration of both burn centers. Eleven records were omitted due to missing key information (missing death or discharge summaries and missing dates of admission).
Determination of Sample Size to Assess Survival Status and Predictors of Mortality Among Pediatric Burn Victims Admitted to Burn Centers in Addis Ababa, Ethiopia, 2020.

Data Collection Tools and Procedures
The information available in the burned pediatric patient charts was checked first, and we prepared an appropriate data extraction checklist in English. The checklist was adapted from related variables by reviewing related literature.20-23 The extraction checklist included gender, age, body part injury, mechanism of injury, length of stay, depth of burn, TBSA, pre-hospital intervention, preexisting medical condition, anatomic location of the burn, and other factors chosen to predict mortality. The charts were obtained from the registration books of the burn centers. Four data collectors (bachelor nurse practitioners working outside the study area) and 1 supervisor in the MSc rank were appointed, and the data collection was accomplished within 4 weeks from March 12 to April 11, 2020.
Data Process and Analysis
After the data was checked for completeness and consistency, it was entered into the Epi Data version 4.4.2.1 software and exported to STATA version 14 for data cleaning, coding, and analysis. Then, an exploratory analysis was applied to determine missing values, influential outliers, and the nature of the data. The data were summarized using frequency, tables, percentages, graphs, and means with standard deviations or medians with an interquartile range based on the distribution of the data. For the comparison of survival differences and to estimate the median survival time, a Kaplan-Meier curve was used. Bivariate analysis was computed using the Cox proportional hazards model to determine the association between each independent variable and outcome variables. As a result, variables with a p-value less than 0.25 are considered eligible for multivariate analysis to determine the net effect of each variable on the outcome variable. The basic assumption of the multi-linear regression model, including the assumption of multi-collinearity, was checked using the variable inflation factors <10 for all independent variables and all variables in the acceptable ranges. The proportional hazard model assumption was checked using a global test (Schoenfeld residuals; P = .865). In addition, the assumption for the proportional hazard model was assessed graphically by the log minus log survival curve and statistically, and it was fulfilled among variables that were eligible for multivariable Cox proportional hazards analysis. Variables with a P-value of <.05 were declared statistically significant when associated with the dependent variable in a multivariable Cox proportional hazards analysis. To describe the association between the outcome (death) and the independent variable adjusted hazards ratio (HR) with a 95% confidence interval (CI) was used.
Data Quality Assurance
Before starting the actual data collection, a pretest was conducted on 21 of the randomly selected burned pediatrics charts at Alert Specialized Hospital, which was not included in the actual study. The training was given to data collectors and a supervisor for 1 day, focusing on what information was to be collected and how they were going to collect relevant information. The evaluation of the collected data was done at the end of each day by the principal investigator and supervisor for its completeness. Charts with incomplete data during data collection were excluded.
Ethical Considerations
Ethical clearance was obtained from the Addis Ababa University institutional review board (IRB) (protocol number
Result
In the period from January 1st, 2016, to December 30, 2019, 1040 cases of pediatric burns were documented in chosen public hospitals in Addis Ababa, Ethiopia. Through a systematic sampling method, 423 participants were initially selected for the study, with 412 (97.4%) ultimately taking part. Regrettably, 11 pediatric burn cases had to be excluded due to incomplete data. Each hospital in the selection received a proportionate allocation of the sample size.
Socio-Demographic Characteristics
From 425 pediatric charts, 412 (97%) records met enrollment criteria in the final analysis; of the 412 participants’ records, 214 (51.9%) were males, and the majority of 233 (56.6%) participants came from urban areas. Pediatric burn victims’ mean age was found to be 5.2 years old. More than half (56.6%) of the study participants originated from urban areas, while the remaining 43.4% came from rural regions. The vast majority (94.2%) of burn accidents occurred within the home environment. Concerning the mechanism of burning, approximately 69% (285 participants) sustained scald injuries. The study revealed that the primary cause of mortality among pediatric burn patients was multi-organ failure, accounting for 29.4% of cases (Table 2).
Socio-Demographic and Clinical Data of Pediatric Burn Victims Admitted to Burning Centers, Addis Ababa, Ethiopia, 2020.
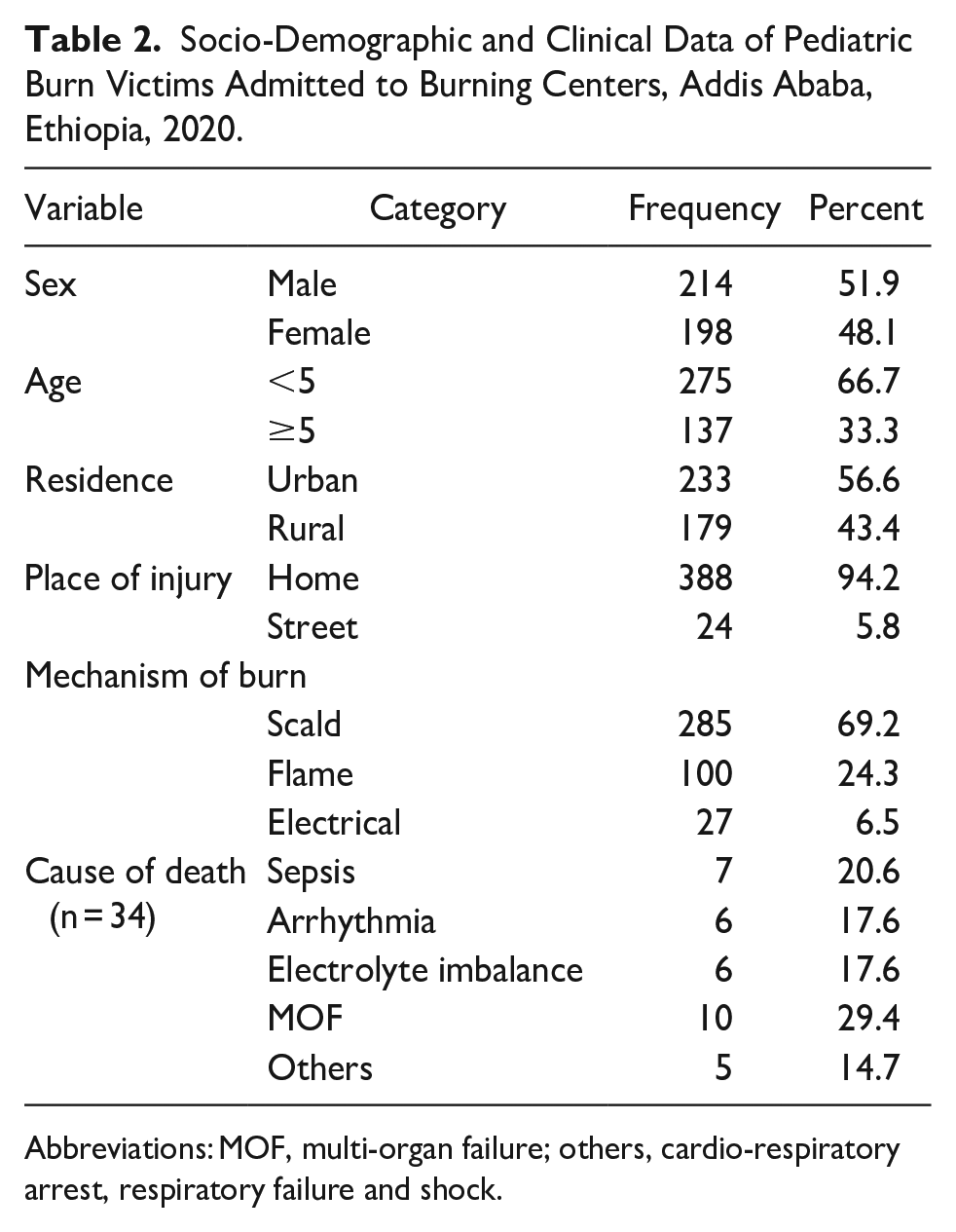
Abbreviations: MOF, multi-organ failure; others, cardio-respiratory arrest, respiratory failure and shock.
Clinical-Related Variables of Pediatric Burn Victims
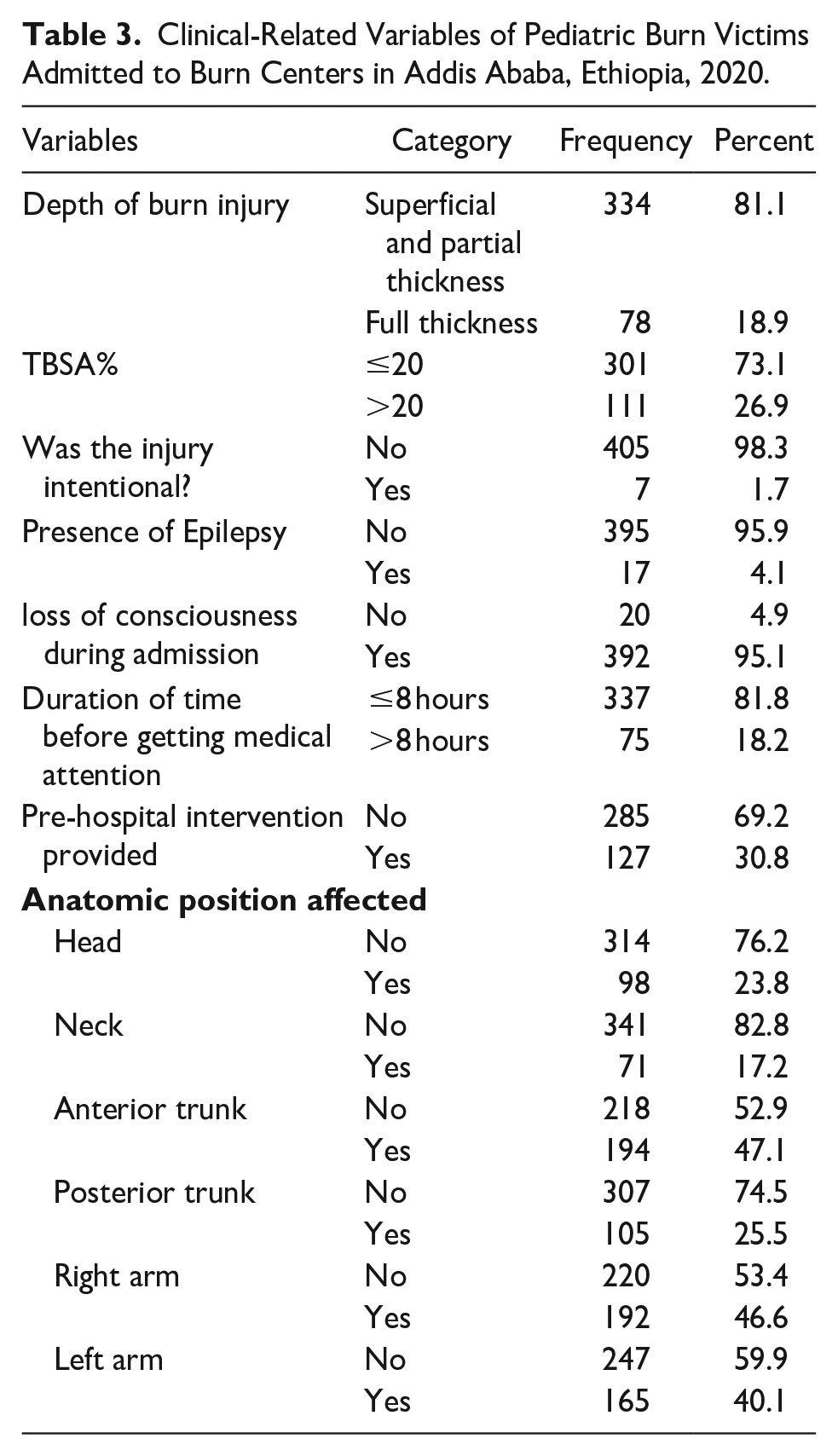
Only 111 (26.9%) of the total number of pediatric burn victims have TBSAs of more than 20%, with the mean total burn surface area accounting for 15.54 ± 11.83 SD. It was the cause of 21 (61.8%) fatalities. According to the study, from the total deaths 17 (50.0%) of them had full-thickness burns. The majority of the 383 burn patients (93.9%) did not have any underlying medical conditions. Sixty-seven (17.7%) of burn patients experienced an illness during their hospitalization; of these, 29 (85.29%) died. Of the participants, only 127 (30.8%) received pre-hospital care. Analysis of the affected body parts revealed that approximately 47% of participants sustained injuries to their anterior trunk, while 46.6% experienced injuries to their right arm (Table 3).
Clinical-Related Variables of Pediatric Burn Victims Admitted to Burn Centers in Addis Ababa, Ethiopia, 2020.
The study revealed that the foremost complications stemming from burns were gastrointestinal and wound-focused sepsis, comprising 67 (16.3%) cases, with anemia trailing at 22 (5.3%). Notably, a substantial majority of participants, 347 (84.1%), underwent treatment with intravenous antibiotics, and all patients received wound care. Additionally, the study highlighted that approximately 32% of participants underwent surgical intervention for their burn injuries (Table 4).
Treatment and Complications of Pediatric Burn Victims Admitted to Burn Centers in Addis Ababa, Ethiopia, 2020.

Abbreviation: Others, contractures; gangrene and respiratory distress.
Survival Status and Incidence of Mortality Among Pediatric Burn Victims
Four hundred and twelve pediatric burn victims were included in the study. According to this study’s findings, the median hospital stay was found to be 25.0 (95% CI: 21.57, 28.5). The pediatric burn victims’ follow-up time ranges from a minimum of 1 day up to a maximum of 269 days. This study also revealed that 34 (8.3%) of the total admitted pediatric burn victims died during the follow-up period, and 19 (55.9%) of these deaths were male. Of the pediatrics included in the analysis, 378 (91.8%) were censored (from which 313 (95.5%) were discharged to home, 5 were referred and 15 (4.0%) of them were discharged against medical advice) upon completion of the study. The incidence rate was found to be 2.4 deaths per 1000 person-day observation (95% CI: 1.77, 3.46) with a total follow-up to the extent of 13 753 person-day.
Survival Status Using the Kaplan Maier Curve
The overall survival probability of pediatric burn victims as revealed by Kaplan-Meier estimate on day 1 of hospital admission is found to be maximum (99.76%) survival observed with a standard error of .0024 (95 CI:.9829, .999). This probability decreases as follow-up time increases. The overall probability of survival of pediatric burn victims was 78.34% with a standard error of .04 (95% CI: .67, .85; Figure 1).
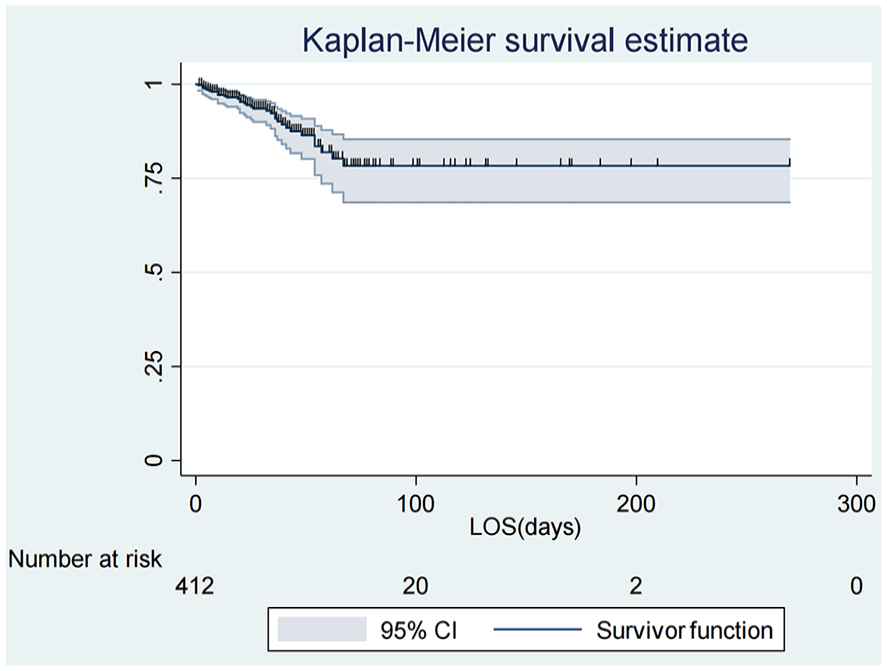
Overall Kaplan-Meier survival estimate among pediatric burn victims admitted to the burn centers from 2016 to 2019, Addis Ababa, Ethiopia, 2020.
The study employed a log-rank test to assess the presence of significant differences among categorical predictor variables. Covariates listed in the table below demonstrated statistical significance (P-value < .25), indicating their potential impact on the outcomes under investigation. This statistical approach helps identify influential factors that may contribute to variations in the study’s outcomes, allowing for a more nuanced understanding of the relationships between predictor variables and outcomes (Table 5).
Log-Rank Test And Median Survival Time for Predictors Among Pediatric Burn Victims Admitted to Burn Centers from 2016 to 2019, Addis Ababa, Ethiopia, 2020.

Predictors of Mortality Among Pediatric Burn Patients
Initially, we determined the nature of the data; the Kaplan-Meier curve and life tables were used for data description. A bivariate analysis was conducted, and variables with a p-value of less than 0.25 were included in the final model for confounder adjustment after performing the model fitness and multi-collinearity tests. Then, those variables in the acceptable range were included in the multivariate analysis. Finally, children who had neck burns and full-thickness burn injuries showed a significant association with mortality among pediatric burn-injured patients at a 95% confidence level. The multivariate analysis result showed that the hazard ratio for pediatric burn victims admitted to the burn centers whose neck burned was 2.8 times more likely to die when compared to pediatric burn victims whose other body areas burned (AHR: 2.8 (95% CI: (1.04, 7.68). Having a full-thickness burn are 2.5 times at risk for mortality (AHR: 2.5 (95% CI: (1.12, 5.62))) when compared to partial-thickness burn depth pediatric burn victims (Table 6).
Bivariate and Multivariate analysis of Cox Proportional Hazard Model for Predictors of Mortality among Pediatric Burn Victims Admitted to Burn Centers, Addis Ababa, Ethiopia, 2020.

Abbreviations: NB, *Statistically significant at P-value at < .05; AHR, Adjusted Hazard Ratio; CHR, Crude Hazard Ratio; TBSA, total body surface area.
Discussion
This study was conducted to determine the survival status and predictors of mortality among pediatric burn injury patients. The incidence rate of mortality among pediatric burn injuries was 2.4 per 1000 person-days of observation. Identifying the factors contributing to the increased mortality of pediatric burn patients would allow us to implement evidence-based interventions and reduce the mortality of pediatric patients. Having a full-thickness burn injury and having a neck burn were reported as predictors of mortality among pediatric patients who were injured with burns.
The overall mortality of pediatric burn patients was 8.25%. This study revealed that the mortality of pediatric burn injuries was in line with a study conducted in Gondar 3 and South Africa. 7 However, it is slightly higher than previously conducted in Mekele at 6.0%, 24 the USA at 3.3%, 13 and New Zealand at 3.2. 15 The discrepancy might be due to poor pre-hospital care services, a shortage of ambulance services, and a lack of burn centers with well-trained and experienced healthcare providers in our study area. This discrepancy may also reflect the difference in awareness and lack of knowledge about first aid of the community for burn care before the arrival of burn centers. In contrast, the findings in this study are lower than those in Cameron, 29%, 22 Ghana 21.3%, 5 Central Malawi 25.9%, 8 and India 31.3%. 19 Given that our study was only conducted in urban areas, the gap may be attributed to regional differences in public awareness and knowledge of burn first aid practices. In this study, the incidence rate was found to be 0.024 deaths per 100 000 person day which is lower than studies conducted in low and middle-income countries. 25 This might be due to the different sources of the population that the current study includes only health institutes found in the urban area and the previous study was done in both urban and rural areas with different burn care. The overall median hospital stay was 25 days with a minimum and maximum follow-up time of 1 and 269 days, which is lower than the study conducted in India Median length of hospital stay was 37 days (range 1-139 days). 26 This difference might be due to different criteria like the availability of resources in the hospital and the quality of care given to pediatric burn injury.
In this study, mortality in full-thickness pediatric burn victims was more likely, which was similar to studies conducted in Texas 27 and northern India. 19 This might be due to the poor quality of care services and lack of advanced equipment in the health facility that tends to expose patients to sepsis, and it might be due to health workers aren’t committed to aggressively resuscitating patients as early as possible after full-tick burn injuries and handover them to specialized burn care centers. Additionally, this study found that neck burn is an independent predictor of pediatric burn victim mortality, which is consistent with studies conducted in Texas, 27 Ghana, 5 and the USA. 28 This could be a result of the parents delaying their visit to a medical facility and the health workers’ ignorance of the increasing complications of neck burn injuries, or poor early detection of signs suggesting a compromised airway. The major complication of burn injuries might be that loss of plasma volume and electrolyte imbalance lead to shock and dysrhythmia, which leads to multi-organ failure (MOF). These complications require well-trained emergency care to increase the probability of survival among children who have burn injuries. Late resuscitation of a burn might lead to more complications due to a lack of knowledge of risk factors for mortality among pediatric burn injuries and a lack of quality emergency care services in our study area.
This study has its limitations. Hence, there was a considerable delay in burn center admission and burn wound management due to the occurrence of burn injuries. Hence, there could be an overestimation of the mortality rate. In addition, we did not evaluate the effect of pre-hospital care due to a lack of records.
Conclusion
The results of this study highlight a concerning frequency of mortality among pediatric burn injury patients. Particularly concerning is the identification of full-thickness burn injuries and neck burns as independent risk factors for death within this vulnerable population. These results highlight the critical need for heightened attention and tailored interventions aimed at reducing mortality rates among pediatric burn victims.
Recommendation
This study recommends developing specialized care protocols for pediatric burn patients, focusing on early identification and management of full-thickness burns and neck burns to minimize the risk of mortality. The study also recommends further research to better understand the underlying mechanisms driving mortality in pediatric burn injury patients, with a focus on identifying novel interventions and strategies to improve outcomes and reduce mortality rates in this vulnerable population.
Acronyms/ Abbreviations
AaBET- Addis Ababa Burn Emergency and Trauma (Hospital)
AAU-Addis Ababa University
HMIS- Health Management Information System
HIC- Higher Income Countries
LIC- Low-Income Countries
LMIC-Low and Middle-Income Countries
MOF- Multi-Organ Failure
TBSA- Total Burn Surface Area
Footnotes
Acknowledgements
We would like to express our heartfelt appreciation to Addis Ababa University College of Health Science, School of Nursing and Midwifery, AaBET Hospital, and Yekatit12 Hospital for their cooperation. We would also like to acknowledge data collectors, supervisors, the center staff, and administrators were appreciated for providing the necessary preliminary information
Authors’ Contributions
ZDB generated the concept and developed the proposal. ZDB, GS, TT, & TMA designed the study and developed the data extraction tool. TSA, TMA, & GS participated in data collection and supervision. ZDB, TSA and TMA performed the statistical analysis, interpreted the findings, and drafted the manuscript. TMA, GS, & TT edited and formatted the manuscript for publication. All the authors read, critically revised, and approved the final version of the manuscript. Finally, all the contributors agreed to be equally accountable for every aspect of the work.
Availability of Data and Materials
All relevant data are within the paper and its supporting information files.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.