
Abstract
Background. Despite numerous life-saving measures, neonatal mortality remains high. This research aims to investigate the incidence and predictors of early neonatal mortality among newborns admitted to intensive care units in public hospitals in Hadiya Zone, Ethiopia. Methods. A retrospective cohort study was conducted on 689 neonates admitted to the neonatal intensive care unit. Cox proportional hazard regression by STATA was used. Results. This study followed for 3439 person-days found an incidence rate of 16.9 deaths per 1000 person-days. Birth weight [AHR = 4.4, 95% CI; 1.29, 14.94], APGAR score at the fifth minute 4 to 6 [AHR = 0.42, 95% CI; 0.2, 0.87], hypoglycemia [AHR = 8.1, 95% CI; 2.17, 30.43], no treated with oxygen [AHR = 2.6, 95% CI; 1.1, 5.9], and obstetric complications [AHR = 0.41, 95% CI; 0.18, 0.93] predicted early neonatal mortality. Conclusion. The study revealed a high neonatal mortality rate, necessitating increased focus on oxygen treatment for newborns and improved early diagnosis and treatment of obstetric complications.
Introduction
Neonatal mortality refers to newborn deaths within the first 4 weeks of life. 1 Neonatal deaths are classified as early neonatal deaths within the first 7 days and late neonatal deaths after 7 days but before a full 28 days of life. 2
The global burden of early neonatal mortality (ENM) is enormous, accounting for 73% of all neonatal deaths in the respective age group. 3 Due to the complexity of the newborn’s adaptive system, this period is particularly vulnerable to life-threatening illnesses. It is the most vulnerable time in human life to disease, and most of it is preventable. 4 It is responsible for 44% of all deaths in children under 5% and 60% of all deaths in infants. 5 Maternal, newborn, and child health is critically important worldwide, yet millions of newborns die from preventable causes. 6 The reasons for neonatal mortality (NM) can be divided into biological and non-biological factors, including prematurity, infections, and asphyxia at delivery. Non-biological influences include socioeconomic status, gender, and maternal education. 7
Worldwide, 2.3 million children died in the first month of life in 2022. 8 Africa accounts for one-third of the global neonatal mortality rate, with sub-Saharan Africa (SSA) accounting for 41% of all newborn children worldwide. 9 Infants born in SSA or South Asia are about ten times more likely to die in the first month than infants born in higher-income countries. Ethiopia has one of the highest NM rates in the world at 30 per 1000 live births, which is significantly higher than the 27 deaths per 1000 live births on the continent and almost 9 times higher than that of developed countries (3 deaths per 1000 live births). 10 Professional doctors can help prevent health problems such as premature birth, sepsis, and suffocation during delivery. To reduce the prevalence of ENM, skilled obstetricians and emergency obstetric care must be available, accessible, and of adequate quality. 11 The Ethiopian government has made great efforts to reduce mortality and improve neonatal survival through strong neonatal life-threatening rescue measures, Child Survival Strategies and the Health Sector Transformation Plan (HSTP).12,13 Despite these efforts, neonatal mortality remains high and requires further investigation into the root causes.
In the era of Sustainable Development Goals (SDGs), reducing neonatal mortality is an integral part of SDG-3. Goal 2 is to end neonatal mortality by targeting a reduction in neonatal mortality to no >12 per 1000 live births by 2030. 14 However, given the current trend in neonatal mortality, Ethiopia needs to accelerate the current reduction rate by at least 2 times to achieve the NMR targeted in SDG 2030. Therefore, this research aims to investigate the incidence and predictors of early neonatal mortality among newborns admitted to public hospitals in Hadiya Zone.
Methods
Study Area and Period
The research was carried out from January 1, 2019 to December 31, 2021 in public hospitals in Hadiya Zone, Central Ethiopia. It included a comprehensive specialty hospital and 3 primary hospitals. Currently, each hospital offers comprehensive medical, surgical, obstetrical, gynaecological, and pediatric services. In addition, each hospital provides inpatient pediatric care and treatment services, including neonatal intensive care unit services. Data was extracted from May 15 to June 30, 2022.
Study Design
A facility-based retrospective follow up study was employed.
Source Population
All neonates whose age was <7 days were admitted to the neonatal intensive care unit at public hospitals in Hadiya Zone.
Study Population
All randomly selected neonates were admitted to the neonatal intensive care unit during the study period.
Inclusion and Exclusion Criteria
Inclusion criteria
All neonates whose age was <7 days were admitted to the NICU during the study period.
Exclusion criteria
Those with incomplete medical records and those who were admitted outside of the study period were excluded.
Sample Size and Sampling Procedure
Using STATA software, the sample size was determined with respect to the following assumptions: the adjusted hazard ratio from the prior study, a power of 80%, and a confidence interval of 95%. Ultimately, 689 was the chosen sample size for this investigation. First, we determined that 4291 infant admissions occurred during the study period to the NICU of WUNEMMCSH (Ni = 3485), Shone Primary Hospital (Ni = 330), Gimbichu Primary Hospital (Ni = 192), and Homacho Primary Hospital (Ni = 284). Following that, the number of samples for each hospital was distributed in the following way, with the allocation made proportionate to the number of prior cases:

Where, nj is the sample size of the jth hospital
NJ is the population size of the jth hospital
n = n1 + n2 +. . . + nk is the total sample size, n = 689
N = N1 + N2 + . . .+ Nk is the total population size, N = 4291
Therefore, Sample size WUNEMMCSH =
Sample size of Shone primary Hospital =
Sample size of Gimbichu primary Hospital =
Sample size of Homacho primary Hospital =
Then each unit should be numbered from 1 to N for each hospital. Finally, study participants were selected from each hospital using a computer-assisted simple random sampling technique (Figure 1).

Schematic presentation of sampling procedure.
Data Collection Procedures
Data extraction checklists were developed in English based on previous studies.2,5,10 The tool includes neonatal and maternal socio-demographic characteristics, maternal and medical disorders, obstetric factors, admission and discharge dates, and neonatal outcome. Three BSC nurses were involved in data collection, and after meeting the inclusion criteria, the medical records of all randomly selected preterm infants admitted to the NICU were reviewed.
Data Quality and Management
Data collectors and supervisors received a 2-day training course. The training focused on the purpose, tools, methods, and ethical concerns of the study during the data extraction phase. The supervisor and PI carefully reviewed and verified the data extraction process, including its completeness and consistency.
Statistical Analysis
Survival time was calculated or censored in days based on the time interval between the time of birth and the time of death. STATA software was used to analyze the data after entering it using Epi-Data. Neonatal cohort characteristics using continuous data were described using median and interquartile range (IQR). The outcome of each newborn was dichotomized as censored or death. The incidence density rate was estimated for the entire study period of hospitalization. The Kaplan-Meier survival curve was used to estimate neonatal survival. To determine whether there were significant differences in survival between the different levels of categorical predictors, a long-term test was performed. The cumulative probability of survival at specific time intervals was estimated using a life table (Table 1). The assumptions of the proportional hazard model were then tested using the Schoenfeld residual test with a value of P>Chi2 = 0.1224, adjusting the model for analysis. The suitability of the model was checked. A bivariate Cox proportional hazard model and multivariable Cox regression analysis were declared with a P value < .05. The adjusted hazard ratios were calculated along with the 95% CI. In addition, texts, tables and graphics were used to present our results.
Life Table of ENM and Predictors Among Newborns.

Results
Socio-Demographic Characteristics
Among the 689 study participants, 415 (60.23%) were males. More than two-third of the participants, 464 (67.3%) came from rural areas. Most neonates, 593 (86.1%), were admitted to the NICU within 24 hours of age. The median age of the mother was 27 years and most mothers, 553 (80.3%) were belonging to 20 to 34 years and median neonatal age at admission to the NICU was 1 day (Table 2).
Socio-Demographic Characteristics.

Maternal Obstetric Characteristics
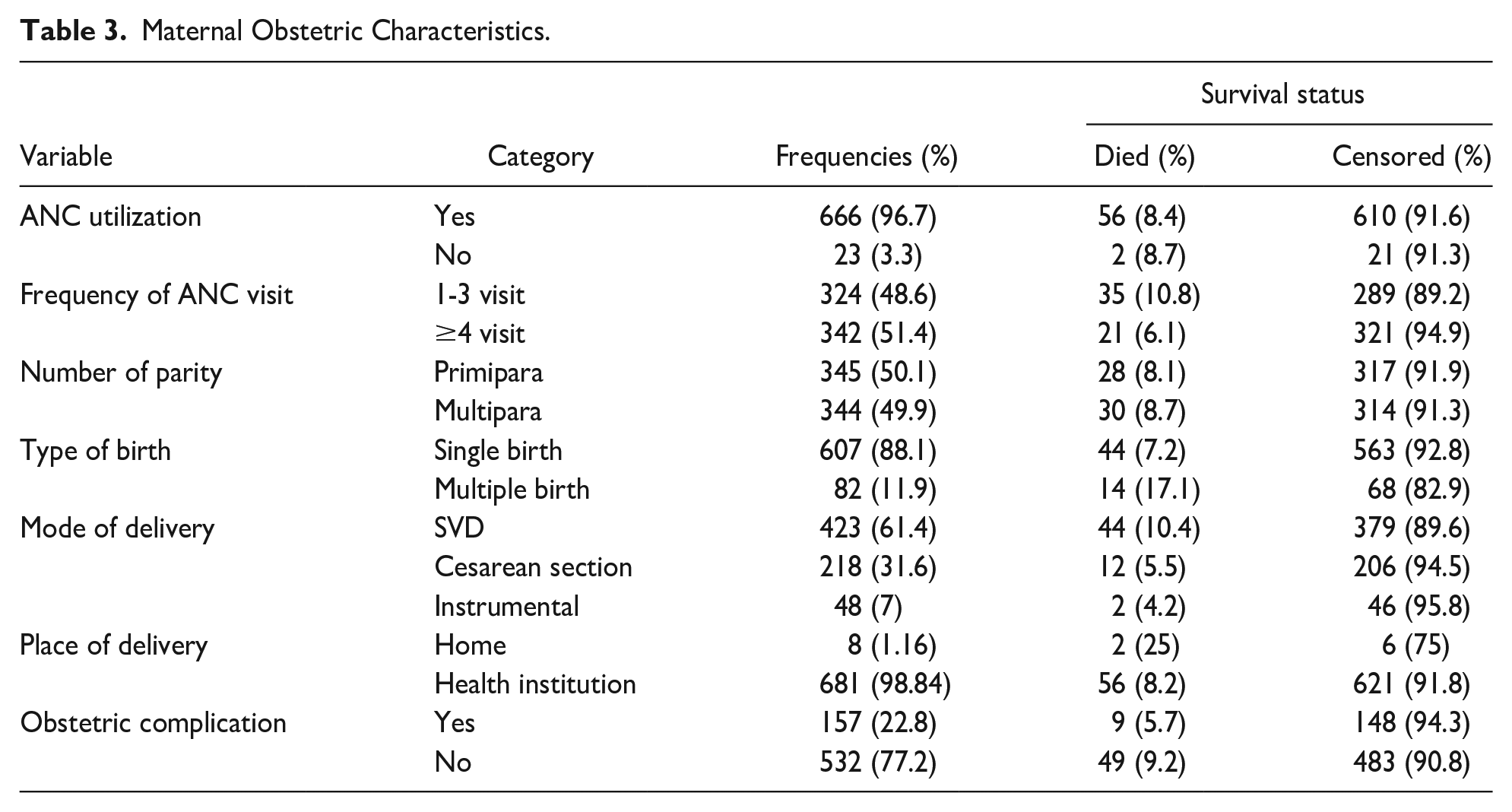
Of the 689 newborns, 666 (96.7%) of their mothers attended ANC services, and of them, 342 (51.3%) received >4 ANC services. Of the 58 neonates who died, 28 (8.1%) died because their mother’s parity was <2. Of 157 (22.8%) mothers of newborns who had an obstetric complication, 9 (5.7%) had died (Table 3).
Maternal Obstetric Characteristics.
Neonatal Characteristics
Among 689 neonates, 69 (10%) of them were in the GA group of ≤32 weeks (very preterm), and 166 (24.1%) were in the GA group between 33 and 36 weeks, of which 20 (29.0%) and 19 (11.4%) of their neonates died, respectively (Table 4).
Neonatal Characteristics.

Maternal Medical Diagnosis
Among the total mothers of neonates enrolled in this study, 28 (4.1%) mothers had hypertension, and 9 (1.3%) had diabetes mellitus, of which 4 (14.3%) and 1 (11.1%) of their neonates died, respectively (Table 5).
Maternal Medical Diagnosis.

Common Medical Diagnosis of Newborn
Prematurity and Perinatal asphyxia were the leading causes of neonatal admission, accounting for 239 (34.7%) and 237 (34.4%), respectively (Figure 2).

Admission diagnosis of early neonates.
Incidence of Early Neonatal Mortality
The study followed a total of 689 neonates for 3439person-days. The median hospital stay was 5.0 days (IQR = 3). And 58 (8.4%) participants died during the period of follow-up. Overall, the incidence density rate of ENM was 16.9 deaths per 1000 person-days, with a 95% confidence interval (13.04, 21.81). The survival rate at the end of the first and seventh days of follow-up was 99.56% with a 95% CI (98.6, 99.8) and 87.3% with a 95% CI (83.28, 90.45), respectively.
Overall Kaplan-Meier Survival Function
In the Kaplan-Meier estimate, the probabilities of survival of early neonates were high during the first day of admission, and relatively fell as follow-up increased. On the first day of hospital stay, a maximum (99.56%) probability of survival was seen, and the over all probability of survival of the early neonate at the end of seventh day was 87.3% [95% CI: 83.28, 90.45] (Figure 3).

Kaplan-Meier survival curves compare neonate survival times.
Survival Probability Comparison for Different Categorical Variables
To facilitate comparisons, the estimation of the survival function for different groups of covariates is provided by the survival curve of the Kaplan-Meier estimator. As indicated below, separate plots of Kaplan-Meier survival function estimates were constructed for various categorical covariates. When one survival function lines up with another, it generally indicates that the group represented by the upper curve survived better than the group represented by the lower curve or had a more advantageous survival experience than the group defined by the lower curve. Neonates those diagnosed with very low birth weight (<1500 g) had shorter survival than those diagnosed with normal birth weight (≥2500 g). At the end of the third day of hospitalization, the overall survival rate of very low birth weight and normal birth weight neonates was 83.64% [95% CI: 70.91, 91.14] and 98.03% [95% CI: 95.91, 99.06]. Respectively, and at the end of the seventh day of hospitalization, the overall survival rate of newborns with a birth weight of <1500 g and ≥2500 g was 52.71% [95% CI: 34.71, 67.83] and 95.15% [95% CI: 91.38 and 97.29, respectively] (Figure 4). This survival time difference was significant at a P-value of <.001.
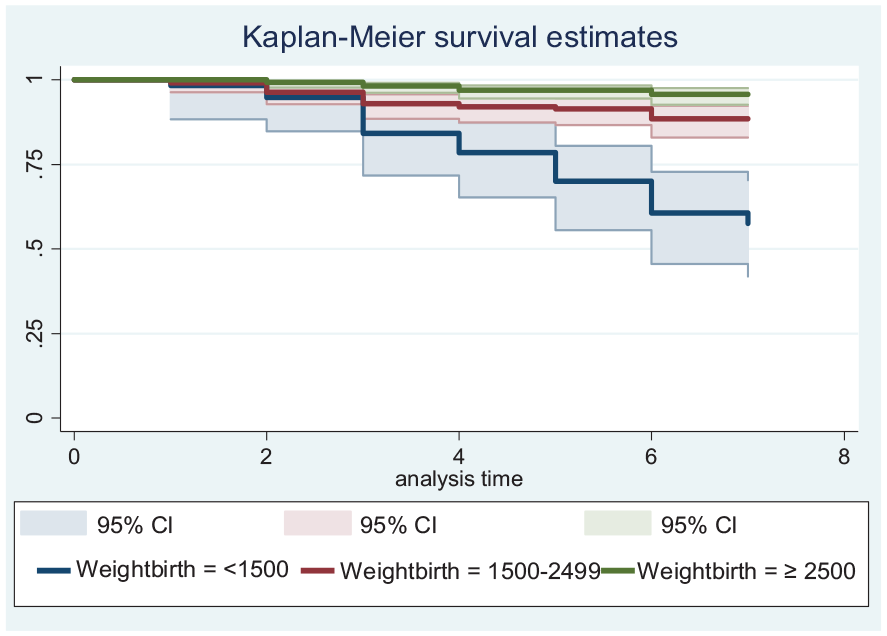
The survival curves of Kaplan-Meier compare survival time of neonate with different birth weight group.
Neonates diagnosed with hypoglycemia had a lower survival time in 7 days of follow up compared to those who had not been diagnosed with hypoglycemia. At the end seventh days of hospital stay, the overall survival of neonates with hypoglycemia and without was hypoglycemia was 67.57% [95% CI: 29, 88.32] and 87.85% [95% CI: 83.79, 90.95] respectively (Figure 5). This survival time difference was statistically significant at P-value = .034.

The Kaplan-Meier survival curves compare neonate survival time with hypoglycemia.
Predictors of Time to Early Neonatal Mortality
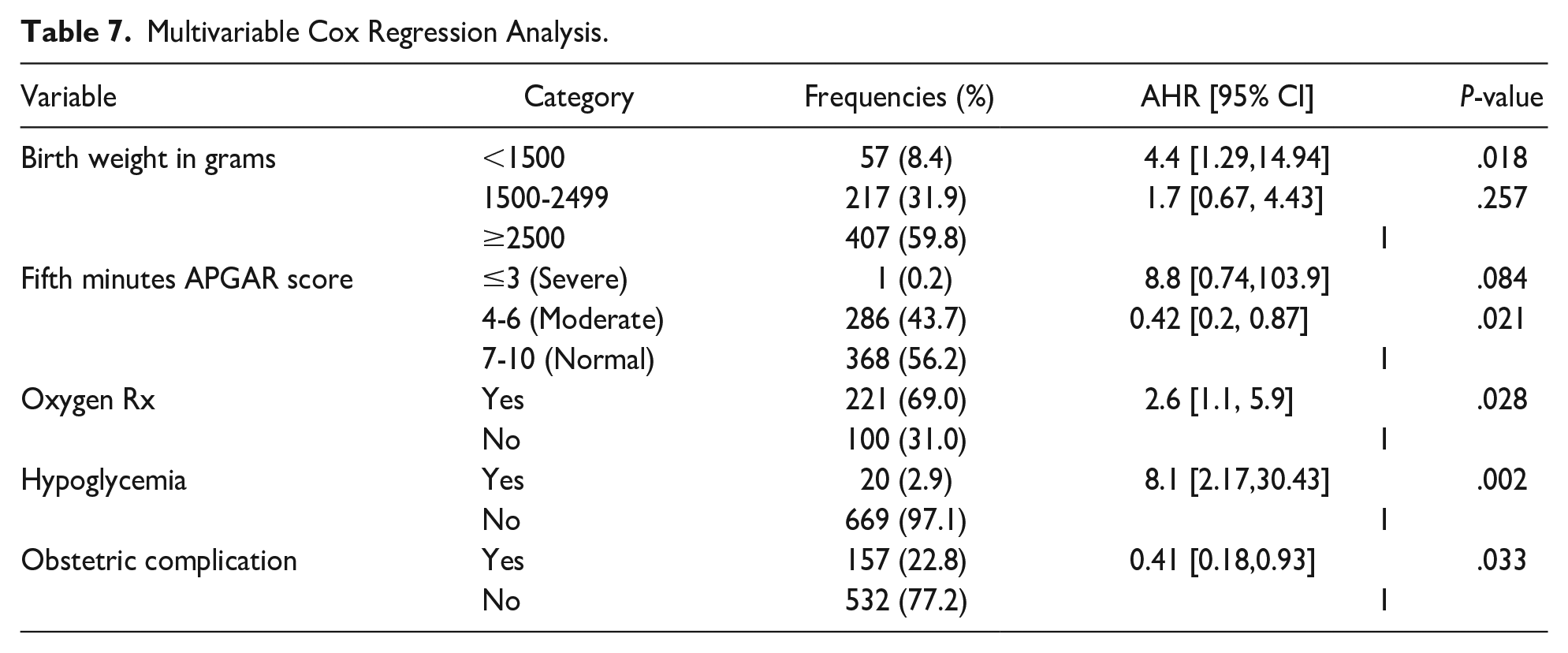
In the bivariate Cox proportional regression analysis, variables with a P value < .25 were candidates for multivariable Cox regression (Table 6). In multivariable Cox proportional hazard analysis, obstetric complications, fifth minute APGAR score 4 to 6 (moderate), birth weight less than 1500 grams, hypoglycemia, and oxygen treatment were independent predictors of early NM. The risk of death in neonates with very low birth weight (<1500 g) was 4.4 times higher than in those with normal birth weight (≥2500 g) [AHR = 4.4, 95% CI; 1.29, 14.94] at P = .018. The neonates with fifth minute APGAR scores of 4 to 6 who were treated early had a 58% lower risk of neonatal death compared to neonates who were not treated early [AHR = 0.42, 95 % CI; 0.20, 0.87] at P = .021. The odds of death were 8.1 times higher in early neonates with hypoglycemia than in neonates who did not develop hypoglycemia [AHR = 8.1, 95% CI; 2.17, 30.43] at P = .002. The risk of death in premature infants who required oxygen but were not treated with oxygen was 2.6 times higher than in those treated with oxygen [AHR = 2.6, 95% CI; 1.1, 5.9] at P = .028, and neonates born to mothers with early diagnosed obstetric complications had a 59% lower risk of neonatal death compared to those not diagnosed early [AHR = 0.41, 95% CI; 0.18, 0.93] at P = .033 (Table 7).
Bivariate Cox Regression Analysis.

Multivariable Cox Regression Analysis.
Discussion
This research aims to investigate the incidence and predictors of early neonatal mortality among newborns admitted to the intensive care unit of public hospitals in Hadiya Zone, Ethiopia. This helps apply evidence-based interventions to countries with limited resources.
The study found that early neonatal mortality was high. Overall, the incidence density of ENM was 16.9 per 1000 person-days. This result was consistent with studies previously conducted in Ethiopia, such as HDSS in Kersa, 15 eastern Ethiopia 19.5 and Woliat Sodo, 16 southern Ethiopia 19.8. However, it was lower than studies conducted in Jimma, 17 Southwest Ethiopia 40, and Tigray Region, 18 Northern Ethiopia 22.4. This discrepancy could be due to differences in study participants and study duration, as reported by Jimma. Study participants in Jimma included only premature babies, which had a higher risk than full-term newborns.
The difference result from Tigray Region could be due to different timing of the study as there were improvements in pregnancy and delivery care from a qualified provider, NICU was well organized and access to trained health care providers since then increased in time in the national survival strategy for newborns and children, special attention was paid to newborns. Likewise, the neonatal mortality rate of the current research was lower than other studies 19 conducted in SSA 22.51 and Uganda 30 NM. 20 This discrepancy in Uganda could be due to differences in sample size (Uganda = 341), socioeconomic status, length of study and subjects studied. Study participants in Uganda included only newborns admitted to the NICU within 24 hours and who could immediately experience complications. However, this study also included newborns admitted before the seventh full day.
The cumulative survival probabilities at the end of the follow-up period were 87.3%. It is comparable to studies from Tigray, 18 northern Ethiopia, 86.96%, and Woliat Sodo, 16 southern Ethiopia, 83.6%. The current finding was higher compared to the study 21 in Arbaminch General Hospital in southern Ethiopia with 75%, in Jimma 22 in southwest Ethiopia with 76.89%. This deviation may occur due to differences in the population. As part of research conducted in Jimma, only premature babies were recruited, those have a higher chance of dying. The inconsistency with the results from Arbaminch General Hospital could be due to variations in the study period. On the other hand, this finding was lower compared to the results in the Tigray region, 18 which was 95.6%. The difference could be due to differences in study participants. The research conducted in Tigray region only included subjects who delivered in study hospitals, while this study included those who delivered at home and were referred from other facilities. Those who came from home had a higher risk of death compared to those admitted to hospitals.
In this finding, the risk of death in newborns with very low birth weight (<1500 g) was 4.4 times higher than in newborns with normal weight (≥2500 g). It is similar to results conducted in various regions of Ethiopia23-25 and other countries such as Nigeria 26 and Uganda. 27 The reason for a very low birth weight is because they are more likely to have premature birth, hypothermia, and become unable to suck breast milk, leading to a risk of death. This study finding showed that neonate with fifth minute APGAR scores 4 to 6 that treated early had lower the risk neonatal death by 58% as contrasted to those not treated early. However, studies in southern Ethiopia 16 and Cameroon 28 showed that lower fifth minutes APGAR scores higher the risk of NM. This could be due to a delay in identifying neonatal complications, their management and misdiagnosis. However, this study suggested that early detection and treatment of the lower fifth APGAR score reduced the risk of neonatal death, which may be related to the concentration of qualified medical professionals and the quality and availability of resuscitation materials.
In the current study, the risk of death was 8.1 times higher in premature infants with hypoglycemia compared to those who were not hypoglycemic. This is in comparison to studies from the University of Gondar, Ethiopia. 29 This could be due to the absence of adipose tissue, which serves as a basis for glucose to acclimate to extra uterine life. Another predictor of early neonatal mortality is obstetric complications. This study found that early diagnosis of obstetric complications reduced the risk of neonatal mortality by 59%. This was supported by evidence from different regions of Ethiopia,17,18,22 Africa, 30 and Indonesia. 31 This showed that delay in recognition and treatment of obstetric complications increased the risk of early NM. This could be related to the concentration of qualified healthcare professionals, the quality and availability of services and the delay in the referring system. According to this result, the risk of death was 2.6 times higher in premature babies who needed oxygen but were not treated with oxygen compared to those who were treated with oxygen. Consistent with previous research conducted in Black Lion Hospital, Ethiopia. 25 This could be because the newborns that required oxygen treatment had severe illness and were at higher risk of death.
According to various studies, meconium aspiration is a common cause of death among newborns in developing countries. Although there is considerable research supporting meconium aspiration as a major cause of neonatal death,32,33 bivariate analysis in this study identified it as a possible cause. However, in multivariable analyses, meconium aspiration was not found to be a significant predictor of early neonatal death. This could be due to various medical services provided by hospitals, such as the early decision to have a cesarean section. Most of the time, health professionals were concerned about the health of the infant and mother and therefore decided to perform a cesarean section as soon as possible if they suspected a risk to the health of the infant and mother. Limitations of this study: Data were collected from medical records (secondary source). Some predictors such as maternal nutritional status, educational status, occupational status, marital status, economic status, and birth interval were overlooked. Medical records with incomplete data were excluded.
Conclusion
The incidence rate of early neonatal mortality was considerably high. Very low birth weight, 5-minute APGAR score rated as moderate, hypoglycemia, oxygen treatment, and obstetric complications were independent predictors of time to early of NM. It is better to pay special attention and close follow-up to the early newborns because the incidence of early neonatal mortality is high, especially during the early neonatal period, and it is also better to strengthen the early diagnosis and treatment of obstetric complications. It is also better to strengthen and design effective newborn care services and develop strategies to reduce the currently identified predictors.
Footnotes
Acknowledgements
We would like to forward our gratitude to Wachemo University, study participants, data collectors and supervisors
Author Contributions
DOK, DEM, TTA, DEA, and BFB contributed equally to the conception or design, contributed to the acquisition, analysis, or interpretation of data, drafted and revised the manuscript for important intellectual content, gave final approval, and agree, to be responsible for all aspects of the manuscript We work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors reviewed, wrote, and approved the final draft for publication.
Data Availability
The data analyzed during the current study are available from the corresponding author up on a request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical clearance was obtained from Wachemo University with Reference number WCU/SGS/651/2014. Subsequently, written letters were taken from Hadiya Zone Health Department to each District Health Office, then to each Primary Hospital. Finally, permission was obtained from the relevant head person and department head of each Primary Hospital. Since the study was conducted by taking appropriate information from neonatal chart and neonatal logbook, it was not inflicted any harm on the patients. As this was a retrospective study, informed consent from participants was not asked because there is no contact with the participants and data was collected from the medical records. For ethics approval it’s waived by the institutional review committee of the university.