
Abstract
Background:
Ethiopia remains among the 5 countries with the highest under-five mortality, yet prospective multicenter data on pediatric intensive care unit (PICU) outcomes are limited.
Objective:
To determine the incidence and predictors of mortality among children admitted to PICUs in Eastern Amhara.
Methods:
A prospective observational study was conducted on 240 children admitted to tertiary-level PICUs between February and April 2025. Kaplan–Meier analysis estimated survival probabilities, and Cox proportional hazards regression identified independent predictors of mortality
Results:
Fifty-eight deaths (24.2%) occurred. Rural residence (AHR: 2.0, 95% CI: 1.2-3.5), the use of inotropic agents (AHR: 2.0, 95% CI: 1.2-3.5) consciousness level (GCS <8; AHR: 2.3, 95% CI: 1.2-4.4), presence of comorbidities (AHR: 1.9, 95% CI: 1.1-3.4) were associated increased mortality.
Conclusion:
PICU mortality was high, especially among rural children, those with severe neurological impairment, comorbidities, or requiring inotropes, emphasizing early identification and close monitoring of high-risk patients.
Introduction
The Pediatric Intensive Care Unit (PICU) delivers specialized, high acuity care to critically children with actual or impending life threating organ dysfunction. Care provided by a highly skilled multidisciplinary team aiming to stabilize vital function, prevent irreversible organ failure, and improved survival outcomes. Children admitted to the PICU commonly present with severe medical emergencies, traumatic injuries, postoperative complications, or critical infections and may be admitted directly or transferred from emergency department or inpatients ward for advanced monitoring and organ suppor.1 -3 Despite these lifesaving roles, PICUs are inherently high risk environments, where diagnostic errors, hospital acquired infections, delayed intervention, and complex medication regimens may contribute to adverse outcomes ad increased mortality. 4
Globally, preventable and treatable conditions remain the leading causes of mortality among children under 5 years of age, particularly in low resource setting. 5 In high-income countries, the establishment of well-resourced PICUs staffed with trained intensivists, and nurses has resulted in substantial improvement in pediatric survival, with reported mortality reductions ranging from 15% to 60%. 6 For instance, reported PICU mortality rates are as low as 3.6% in Japan, 7 and 2.6% in Australia and New Zealand. 8 In contrast, pediatric emergency and critical care service in many low-and middle countries (LMICs) remain underdeveloped and fragmented. 9 This disparity is especially pronounced in Sub-Saharan Africa (SSA), where PICU care is constrained by limited infrastructure, and shortage of trained personnel. Inadequate nurse to patient’s ratios, restricted access to essential equipment, and delayed referral systems.10 -12 As a result, the reported PICU mortality rates were significantly higher in resource-limited settings, ranging from 10.3% to 41.2%.13 -18
In 2018 alone, an estimated 5.3 million children died worldwide, with nearly 80% of these deaths occurring in SSA and Asia. 19 By 2020, SSA continues to shoulder a disproportionate burden, accounting for approximately 53% global under-five deaths,20,21 largely driven by severe infections, including pneumonia, diarrhea, and malaria, condition frequently necessitate intensive care when complication arise. 22 Ethiopian remains among the 5 countries with the highest under-five mortality rates globally, estimated at 59 deaths per 1000 live births.5,23 In Ethiopian PICUs and similar regional settings, septic shock, acute medical emergencies, and trauma represent the most common indications for admission.17,24,25
Previous studies have identified multiple factors associate with PICU mortality, including the younger age, patient’s clinical condition at admission, presence of comorbid conditions, altered level of consciousness, and the need for advanced life support interventions such as mechanical ventilation (MV).17,18,24 -28 However, the magnitude and direction of these associations vary across studies, reflecting differences in patient populations, health-care infrastructure, study design, and clinical practices.
Despite the high burden of critical illness and mortality, there is a paucity of high quality of prospective and multicenter data on PICU outcomes and their predictors in Ethiopia. Prior studies have largely relied on single center, retrospective chart reviews, which are limited by incomplete documentation, selection bias and restricted generalizability.24,25,29,30 The lack of robust multicenter evidence hinders the development of evidence-based clinical protocols, efficient resource allocation, and targeted interventions to improve pediatric critical care outcomes. To address these gaps, we conducted a prospective multicenter observational study in tertiary hospital PICUs of Eastern Amhara, enabling standardized data collection across multiple sites, minimizing bias, and enhancing the applicability of findings. By generating context-specific and methodologically rigorous evidence, these studies aims to inform clinical decision-making, support health-system strengthening, and contribute to reducing preventable pediatric mortality in resource-limited settings.
Methods and Material
Study Setting, Design, and Period
This prospective observational study was conducted from February 2025 to April 2025 in tertiary-level hospitals in Eastern Amhara, Ethiopia. The study was carried out in 3 hospitals with established PICU services: Debre Tabor Comprehensive Specialized Hospital (DCSH) and Felege Hiwot Comprehensive Specialized Hospital (FHCSH) and Tibebe Ghion Comprehensive Specialized Hospital (TGCSH). DCSH serves as the main referral hospital for south Gondar and surrounding districts. The hospitals admit over 1160 pediatric patients annually and has pediatric ward with 45 beds, including 6 designated PICU beds. FHCSH is one of the largest referral hospitals in the region, with 118 pediatric beds and an 11-bed PICU. TGCSH is a tertiary teaching hospital with 459 inpatient beds, including 52 pediatric beds and 10 PICU beds.
These hospitals function as the highest level of pediatric care within the regional health system and receive critically ill children through a structured referral pathway from primary hospitals, district hospitals, and emergency departments. Children are admitted to the PICU either directly from emergency units or transferred from pediatric and surgical wards following clinical deterioration requiring advanced monitoring and organ support.
Populations and Eligibility Criteria
The source population for this study consisted of all pediatric patients admitted to tertiary-level hospitals in Eastern Amhara, Ethiopia. The study population included patients aged 14 days to 18 years who were admitted to the PICU during the study period and met the inclusion criteria. Patients with missing or incomplete baseline critical variables within the specified time window, primarily due to clinical urgency or operational constraints, were excluded from the study after attempts to retrieve the data from source document. Additionally, those who died within 2 hours of admission were also excluded, as this timeframe does not allow for optimal PICU care, and their outcomes are more closely associated with the care provided in the emergency department or before admission.
Sample Size Calculation and Sampling Technique
Sample size was determined using an events-per-variable (EPV) approach for Cox regression. With up to 10 predictors and a minimum of 10 event per variable, at least 100 outcome events were required. 31 Prior Ethiopian and SSA PICU studies report mortality rates of 30% to 50%.24,32 -34 Assuming a conservative mortality rate of 40%, enrollment 240 patients was expected to yield approximately 96 deaths (EPV ≈ 9.6), which was considered adequate for planned multivariable analysis.
Based on historical admission data, the sample was proportionally allocated across the 3 hospitals, resulting in 73 patients for DCSH, 78 for TGCSH, and 89 for FHCSH. A consecutive sampling approach was employed, whereby all eligible patients admitted to the PICU during the study period were approached sequentially until the hospital-specific sample size was achieved. A flow diagram illustrates pediatric patient recruitment, hospital-level inclusion, reasons for exclusion, and the age distribution of the final study cohort in the PICUs of the 3 hospitals. Two neonates (14-28 days) were admitted to the PICU due to full NICU capacity but were excluded because both died within 2 hours of admission. As a result, all patients included in the final analysis were older than 1 month (Supplemental Figure S1). Each patient was assigned a unique identification and questionnaire code to prevent duplicate inclusion of patient charts in the study.
Study Variables
The primary outcome of this study is time to death. Explanatory variables were socio-demographic characteristics (age, weight, caregiver occupation, etc.), presence of comorbidity conditions, hemoglobin level, admission diagnosis (septic shock, meningitis, and respiratory failure), nutritional status (Z-score), Glasgow Coma Scale (GCS), patient feeding method, interventions; use of MV, urinary catheter, central catheter, use of antibiotics, inotropes, in-PICU complication, and length of MV stay.
Operational Definitions
Data Collection Procedures and Quality Assurance
Data were collected prospectively using a structured case record form developed based on comprehensive literature review and prepared in English.17,18,24,25,28 Data were pretested on 5% of the sample at a tertiary hospital in the region, and necessary modifications were made. After obtaining written informed consent from caregivers, data were collected by trained medical interns under the supervision of treating physicians.
Baseline data were collected within 2 hours of PICU admission, including comorbidities, vital signs, oxygen saturation, neurological status evaluated using the pediatric Glasgow Coma Scale (GCS), nutritional status determined using anthropometric Z-scores, feeding method, hemoglobin level, admission diagnoses, and the need for invasive procedures such as MV, urinary catheterization, or central venous access. Early stabilization variables, documented within 12 hour, comprised vasopressor use, ventilator support, urine output, fluid balance, and evolving organ dysfunction using predefined criteria. Follow-up data were recorded daily throughout the PICU stay and included daily therapeutic exposures (antibiotics, and other drugs), duration of MV, in-PICU complications such as hospital-acquired infections (HAI; defined per World Health Organization and Centers for Disease Control and Prevention criteria as infections occurring ≥48 hours after admission), and clinical outcomes. The primary outcome, time to death, was measured in days from admission to death or discharge, with censoring at transfer, survival and other reasons.
Standardize orientation and training sessions were conducted to ensure uniform understanding of the study objectives, variable definition, and data collection procedures. Daily supervision and verification of collected data were conducted by the principal investigator. Data were double-entered and validated to ensure accuracy. Multi-center variability was assessed through Kaplan-Meier survival curves, log-rank tests, and hospital-level frailty analysis; however, variability between hospitals was statistically insignificant, and patient-level predictors were analyzed using standard multivariable Cox regression (Supplemental File S1). Investigators accessed medical records solely for research purposes and were not involved in patient care.
Data Processing and Analysis Procedure
Data were coded and cleaned using EpiData v4.6.6 and analyzed in STATA v17. Categorical variables were summarized as frequencies and percentages, and continuous variables as median (IQR). Survival distributions between groups were compared using Kaplan-Meier curves and the log-rank test. Predictors of time to death were analyzed with Cox proportional hazards regression. Variables with P < .2 in bi-variable analysis were entered into multi-variable models, and P < .05 was considered statistically significant. Model assumptions were checked using Schoenfeld and Martingale residuals, and multicollinearity was assessed using variance inflation factors (VIF <1.3).
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board of (an institutional review board in Ethiopia [approval details withheld for peer review]), and permissions were obtained from (the relevant hospital authorities). Informed consent was secured from the legal guardians of all participants after explaining the study objectives and procedures, including the right to withdraw at any time. The study adhered to the Declaration of Helsinki, and all data were anonymized and securely stored to ensure participant confidentiality.
Result
Socio-Demographic Characteristics of Study Participants
In this study, males comprised 50.8% of the study population (n = 122). Mortality was 13.3% among males and 10.8% among females; however, survival distribution did not differ significantly by sex (log-rank P = .4). Similarly, there was no significant difference in survival distribution across age groups (log-rank P = .3). Urban residents accounted for 52.4% of participants (n = 127), and residential location was found to have significant difference in survival distribution (log-rank P = .01). The emergency room was the largest source of admission, represented 45.8% (n = 110), followed by the medical ward (n = 83, 34.6%). Although patients admitted from the emergency room had a higher cumulative incidence of death (n = 25, 10.4%), survival distributions did not differ significantly by source of admission (log-rank P = .7; Table 1).
Sociodemographic-Related Characteristics With Cumulative Incidence of Death and Survival Probability of Study Participants.

Note. Other: student, pension, and unemployed.
Indicates statistically significant results (p < 0.05).
Clinical-Related Characteristics and Diagnosis of PICU
The primary reasons for PICU admission were respiratory failure (n = 43, 17.9%), meningitis (n = 42, 17.5%), and septic shock (n = 41, 17.1%). The cumulative incidence of death was highest among children admitted with respiratory failure (n = 20, 8.3%). However, survival distribution a did not differ significantly by admission diagnosis of septic shock or meningitis (log rank P > .05). In contrast, survival distribution differed significantly according to neurological status at admission, with children presenting with GCS score of <8 (log-rank P < .001; Table 2).
Clinical-Related and Diagnostic Characteristics of the Cumulative Incidence of Death and Survival Probability of Patients.

Abbreviation: MODS, multi-organ dysfunction syndrome.
Indicates statistically significant results (p < 0.05).
Cardiovascular cases: congestive heart failure, cardiac arrest, and cardiogenic shock.
Miscellaneous: neutropenic fever, diabetic ketoacidosis, upper respiratory obstruction, and status epileptics.
Comorbid conditions were recorded in 46.7% of patients (n = 122) and were present among 40 deaths (16.7%). Of the 183 documented comorbidities, severe acute malnutrition (ICD-11:5B52) was the most prevalent, accounted for 27.7%, followed by anemia and other erythrocyte disorders (ICD-11:3A00-3A9Z), observed in 20.2%. HAI constituted the predominant in-PICU complication, occurring in 53.1% of complicated cases (Supplemental Table S1). Among 25 patients with HAI, 13 died (52.0%). Kaplan–Meier analysis showed lower survival in the HAI group, though the log-rank test did not reach statistical significance (P = .06), indicating a non-significant trend toward higher mortality (Supplemental File S2). Moreover, survival distributions did not differ significantly according to the presence of organ dysfunction (log-rank P = .20) or the administration of maintenance intravenous fluids (log-rank P = .60; Table 2).
Management of Pediatric Patient Admitted to the PICU
Upon admission, antibiotics were administered to 91.3% patients (n = 219). MV was required in 29.2% patients (n = 70). Survival distribution differed significantly between ventilated and non-ventilated patients (log-rank P < .001), with the approximately 12.5% higher cumulative incidence of death among ventilated patients. Among those receiving MV, ventilation lasting >7 days was observed in 5.8% deaths (n = 14). Inotropic agents were administered to 30.8% patients (n = 74), and survival distributions differed significantly according to inotrope use (log-rank P = .01), with 12.9% deaths (n = 31) occurring in this group (Table 3).
Types of Treatments Given for Patients Admitted to PICU.
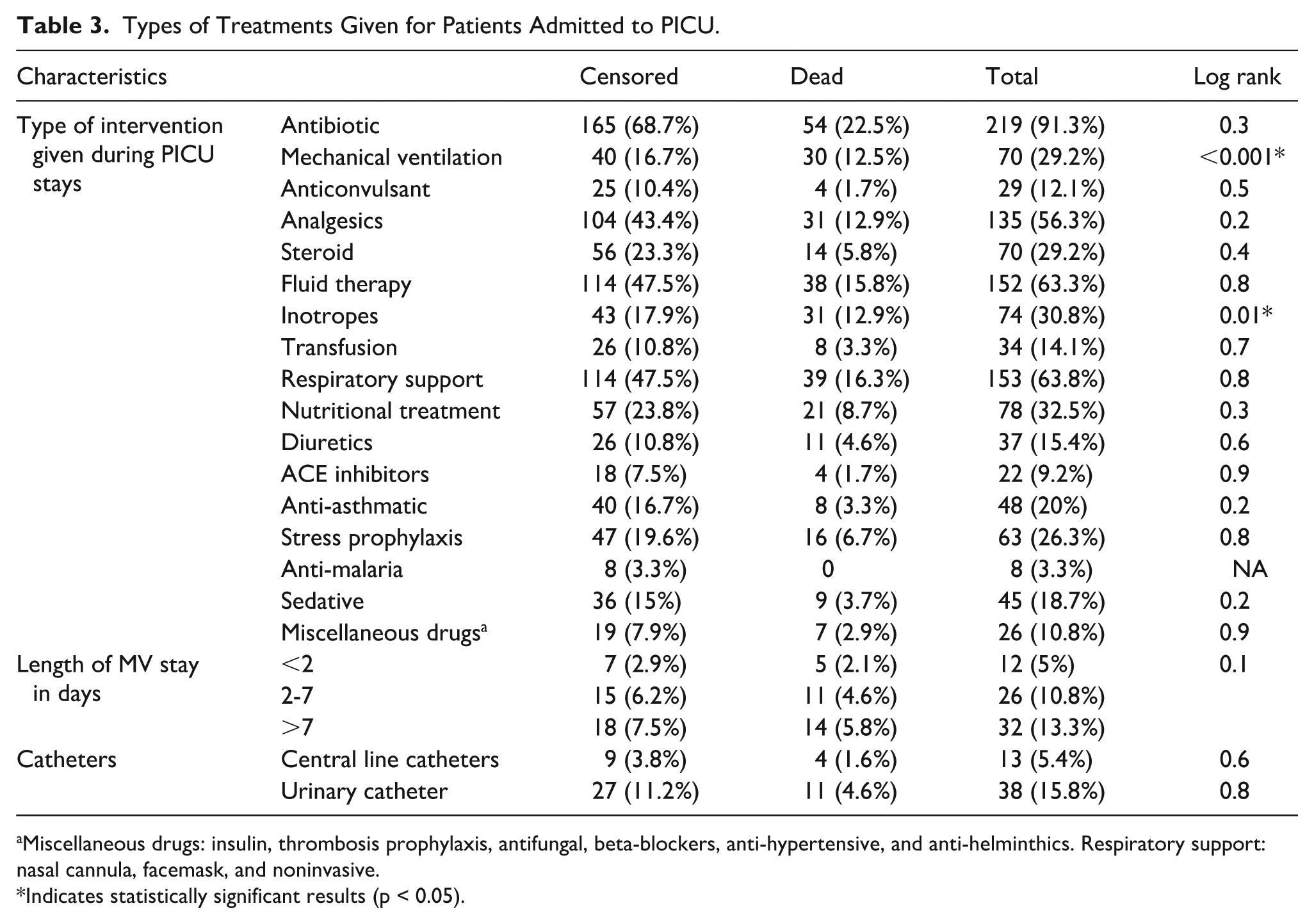
Miscellaneous drugs: insulin, thrombosis prophylaxis, antifungal, beta-blockers, anti-hypertensive, and anti-helminthics. Respiratory support: nasal cannula, facemask, and noninvasive.
Indicates statistically significant results (p < 0.05).
Incidence Rate and PICU Outcomes
During the study period, 24.2% patients (n = 58) died in the PICU; however, 75.8% (n = 182) were censored. Of the censored cases, 47.5% (n = 114) improved and were transferred to the wards. The overall incidence rate of death was 5.37 deaths per 100 person-days (95% CI: 2.87-9.8; Figure 1).
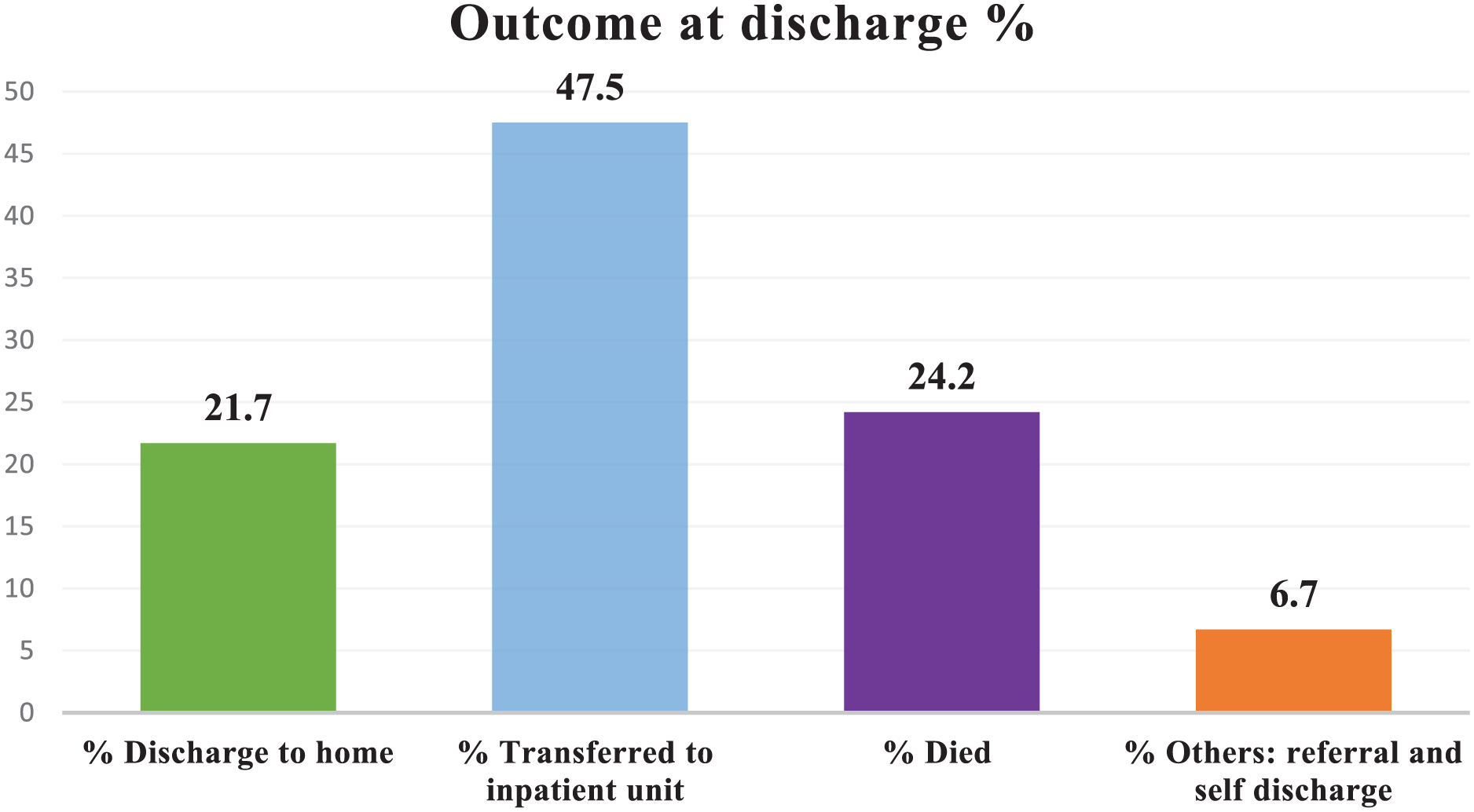
Outcome at discharge among pediatric patients admitted to the PICU.
Kaplan-Meier Curve for Variable Groups
According to this study, pediatric patients from rural areas had shorter survival estimates compared to their urban counterparts (Figure 2). Patients with a low consciousness level (≤8) exhibited a higher probability of mortality than those with a higher consciousness level (>8; Figure 3). Additionally, the survival probability for patients who did not receive inotropic agents was better than for those who did (Figure 4). Furthermore, patients with coexisting diseases experienced shorter survival probabilities than those without such conditions (Figure 5).

Kaplan-Meier curves showing survival estimates for pediatric patients by residence.
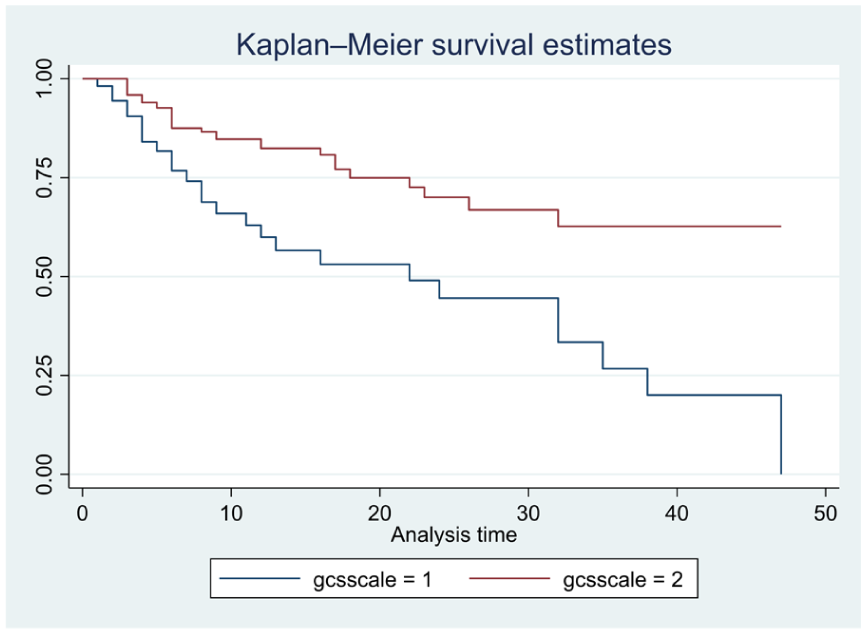
Kaplan-Meier curves showing survival estimates for pediatric patients regarding to conscious level.

Kaplan-Meier curves showing survival estimates for pediatric patients regarding to inotropic agent.

Kaplan-Meier curves showing survival estimates for pediatric patients with the presence of comorbidity.
Predictors of Mortality in the PICU
A Cox proportional hazard regression was performed to identify predictors of in-PICU mortality. Accordingly, residence, nutritional status, meningitis diagnosis, respiratory failure, the use of inotropic agents, need for a MV, consciousness level, in-PICU complications, and the presence of comorbid conditions were first assessed in bi-variable analysis. Variables with P < .20 were entered into the multi-variable model. Model adequacy was assessed using Cox–Snell residuals, which demonstrated that the observed cumulative hazard closely aligned with the expected line, indicating an acceptable fit of the Cox proportional hazards model (Supplemental Figure S2).
In the final multi-variable model, 4 variables were independently associated with an increased risk of death. Patients from rural areas had a 2.0-fold increased risk of death compared to those from urban areas (AHR: 2.0, 95% CI: 1.2-3.5; P = .013). The use of inotropic agents was associated with a 2.0-fold higher risk of mortality compared to those who did not receive them (AHR: 2.0, 95% CI: 1.2-3.5; P = .012). Unconscious patients (GCS < 8) had a 2.3-fold increased hazard of dying compared to conscious patients (AHR: 2.3, 95% CI: 1.2-4.4; P = .011). The presence of comorbidities increased the mortality risk by 1.9 times compared to patients without comorbidities (AHR: 1.9 95% CI: 1.1-3.4; P = .033; Table 4).
Bivariate and Multivariable Cox Proportional Hazard Regression to Identify Predictors of In-ICU Mortality at PICU.

Note. The martingale residuals goodness-of-fit test shows χ2(1) = .1 and P-value = .5, indicating a good fit for the multivariate model. The global Schoenfeld test results are chi χ2(8) = 3.9 with a P-value of .9. There is no multicollinearity concern, with a maximum VIF of 1.24.
Indicates statistically significant results (p < 0.05).
Discussion
This multicenter prospective study provides the first comprehensive evidence on survival outcomes and predictors of mortality among pediatric patient admitted to tertiary hospital PICUs in Eastern Amhara. The main findings reveal a high PICU mortality rate, with rural residence, comorbidities, severe neurological impairment (GCS <8), and the need for inotropic support emerging as independent predictors of death. These findings highlight systemic challenge in pediatric critical care in resource-limited settings, where delayed referral, inadequate monitoring, and high infection burden contribute to poor outcomes.
The observed PICU mortality align with reports from other LMICs, including Ethiopia (32.6%), Pakistan (26.6%), and Mozambique (25%),15,30,37 but is lower than studies from Tanzania (41.4%), Uganda (40.1%), and Egypt (37.95%).14,16,38 Differences likely reflect variation in patient case mix, illness severity at admission, and the availability of critical care resources. For instance, a cohort in Jimma, Ethiopia, with a higher proportion of trauma cases, 17 reported 40% mortality, particularly severe head injuries. 39 Conversely, our mortality is higher than reports from Iran (16.5%), Nepal (12.6%), and India (14%).13,40,41 This elevated mortality in our cohort might attributed to systemic factors, including delayed presentation, limited emergency service, staff shortages, and insufficient equipment.9 -12 In high income countries, greater staffing and advanced facilities are associated with <5% PICU mortality,7,8 emphasizing the influence of systemic factors on outcomes
The elevated mortality observed in our cohorts may be partly attributable to the predominance of children under 5 years of age, who are particularly vulnerable to infection, malnutrition, and other preventable condition due to immature immune systems and lower physiological reserve. In addition, nearly half of admissions were emergencies, reflecting delayed presentation and limited access to intermediate level care, which underscores the need for early identification and timely referral.42,43 Similarly, deaths were common among children with infectious diseases, consistent with other LMICs reports,15,44 highlighting the continued burden of preventable infectious and antimicrobial resistance.
In this study, respiratory and central nervous system (CNS) disorders were the leading causes of PICU admission, consistent with previous studies.15,40,45 This conditions frequently are associated with a high deterioration risk. These observations underscore the importance of timely ventilator support, early antimicrobial therapy, and intensive neurological monitoring. The relatively prolonged PICU stays observed in this cohort, align with similar settings,33,44 likely reflect both the severity of illness at admission and development of in PICU complications such as HAI collectively contributing to the high mortality in this context.
Key predictors of mortality provide insight into both clinical severity and contextual challenges. Children from rural areas faced a higher mortality. This is consistent with the findings of studies done in another region of Ethiopia. 29 A study in Lebanon, rural-residing children had a 44% increased risk of in-hospital mortality. 46 Likewise, a study conducted in the United States found also a similar finding, partly due to increased exposure to drug-resistant bacteremia. 47 This possibly due to delays care-seeking, limited transportation, reliance on traditional healers, and higher prevalence of malnutrition and chronic infections.48,49
Underlying comorbidities independently increased mortality risk, as seen in other LMICs studies.25,50 -52 Conditions such as chronic malnutrition, HIV infection and tuberculosis reduce physiological reserve, impair immune function, and limit the ability to tolerate acute critical illness. 53 In resource limited settings, delayed diagnosis and sub-optimal management of these conditions often result in advanced diseases at PICU admission, 54 contributing to rapid deterioration and poor outcomes.
Severe neurological impairment at admission was a strong mortality predictor; consistent with prior studies.55 -57 Depressed consciousness reflects advanced diseases severity, risk of aspiration, respiratory failure and hemodynamic instability. 58 In resource limiting settings, where capacity for continuous neurological monitoring and rapid airway intervention is constrained, these risks are further amplified.54,59 Early recognition and supportive care are therefore critical.
The requirement for inotropic support was also associated with increased mortality, indicating profound circulatory compromise. This finding is supported by previous published researchs.44,60 Inotropic therapy typically reflects severe shock or cardiac dysfunction, often secondary to sepsis or advanced infection. 61 In resource constrained PICUs, delay in shock recognition, limited access to invasive monitoring, and high patient -to-staff ratios may hinder timey circulatory support.59,62 These findings highlight the importance of prompt recognition and management of hemodynamic instability
Although log rank analysis showed that survival distribution significantly differed in both children requiring MV and admitted with respiratory failure, these factors were not independent predictor in multivariable models. However, previous studies have reported both as independent predictor of mortality.17,24,33 This possibly due to limited sample size, case heterogeneity, or residual confounding. Larger multicenter studies are needed to clarify prognostic factors and guide context-specific interventions for early recognition and supportive care in PICUs.
Evidence based implication from our finding include the need for close monitoring and timely management of children with severe neurological impairment, comorbidities, or requiring inotropic support. Addressing underlying comorbidities, preventing and promptly managing HAI, and ensuring access to effective antimicrobials are supported by the data.
This study’s multicenter design strengthens generalizability and allowed assessment of variability across PICUs of Eastern Amhara. Limitation include missing caregiver socioeconomic data, inability to PIM2 score for all patients, relatively small sample size reducing multivariable power, observational design preventing causal inference, and potential residual confounding from unmeasured factors such as pre-hospital care differences or PICU resource constraints. Additionally, although vaccination records were prospectively verified, age-specific timing was not consistently available, so some children up-to-date for their age may have been misclassified as not fully vaccinated.
Conclusion
This multicenter study found a high incidence of in-PICU mortality among pediatric patients admitted to tertiary hospitals in Eastern Amhara. Mortality was independently associated with rural residence, severe neurological impairment (GCS <8), need for inotropic support, and the presence of underlying comorbidities, with children from rural areas and those under 5 years particularly vulnerable. These findings highlight the importance of early identification and close monitoring of high-risk children, timely referral from rural areas, and targeted management of comorbidities such as malnutrition and chronic illnesses. Prospective studies are warranted to evaluate interventions aimed at improving survival and clinical outcomes in PICUs in resource-limited settings.
Supplemental Material
sj-docx-3-gph-10.1177_30502225261424327 – Supplemental material for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study
Supplemental material, sj-docx-3-gph-10.1177_30502225261424327 for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study by Abel Temeche Kassaw, Eliyas Addisu Taye, Desalegn Addis Mussie, Getachew Yitayew Tarekegn, Samuel Berihun Dagnew and Tigabu Eskeziya Zerihun in Sage Open Pediatrics
Supplemental Material
sj-docx-4-gph-10.1177_30502225261424327 – Supplemental material for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study
Supplemental material, sj-docx-4-gph-10.1177_30502225261424327 for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study by Abel Temeche Kassaw, Eliyas Addisu Taye, Desalegn Addis Mussie, Getachew Yitayew Tarekegn, Samuel Berihun Dagnew and Tigabu Eskeziya Zerihun in Sage Open Pediatrics
Supplemental Material
sj-docx-5-gph-10.1177_30502225261424327 – Supplemental material for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study
Supplemental material, sj-docx-5-gph-10.1177_30502225261424327 for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study by Abel Temeche Kassaw, Eliyas Addisu Taye, Desalegn Addis Mussie, Getachew Yitayew Tarekegn, Samuel Berihun Dagnew and Tigabu Eskeziya Zerihun in Sage Open Pediatrics
Supplemental Material
sj-pdf-1-gph-10.1177_30502225261424327 – Supplemental material for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study
Supplemental material, sj-pdf-1-gph-10.1177_30502225261424327 for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study by Abel Temeche Kassaw, Eliyas Addisu Taye, Desalegn Addis Mussie, Getachew Yitayew Tarekegn, Samuel Berihun Dagnew and Tigabu Eskeziya Zerihun in Sage Open Pediatrics
Supplemental Material
sj-pdf-2-gph-10.1177_30502225261424327 – Supplemental material for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study
Supplemental material, sj-pdf-2-gph-10.1177_30502225261424327 for Predictors of Mortality Among Pediatric Patients Admitted to Intensive Care Units in Eastern Amhara, Ethiopia: A Prospective Multi-Center Cohort Study by Abel Temeche Kassaw, Eliyas Addisu Taye, Desalegn Addis Mussie, Getachew Yitayew Tarekegn, Samuel Berihun Dagnew and Tigabu Eskeziya Zerihun in Sage Open Pediatrics
Footnotes
Acknowledgements
The authors extend their sincere gratitude to the pediatric staff at Debre Tabor, Tibebe Ghion, and Felege Hiwot Comprehensive Specialized Hospitals for their invaluable cooperation and support throughout the study. Finally, we offer our heartfelt appreciation to the families of all participating patients for their trust and consent.
ORCID iDs
Ethical Considerations
Ethical approval was obtained from the Institutional Research Ethics Review Committee (IRERC) at Debre Tabor University (DTU) (Approval No: DTU/IRERC/007/2018), and permissions were obtained from the Chief Clinical Directors of all participating hospitals.
Consent to Participate
Written informed consent was secured from legal guardians after explanation of study objectives and procedures. Participation was voluntary, with the right to withdraw at any time without consequence. All data were anonymized and handled confidentially in accordance with the Declaration of Helsinki.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be disclosed on a reasonable request from the corresponding author.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.