
Abstract
Background
Adverse neonatal outcomes have a significant effect on perinatal and neonatal survival and the risk of developmental disabilities and illnesses throughout future lives. Hence, the objective of this study was to identify adverse neonatal outcomes and associated risk factors.
Method
Institutional based unmatched case-control study was conducted among 206 neonates. Neonates who had adverse outcomes were cases with their index mothers and those neonates who hadn’t had adverse outcomes were controls with their index mothers. Sociodemographic, potential neonatal risk factors, and clinical data were taken from the mothers and medical records. Data were entered into Epi Info v7 and analyzed using SPSS v23. Bivariate and multivariable logistic regression analyses were used to adjust for confounding factors of adverse neonatal outcomes. Frequencies, means, standard deviations, percentages, and cross-tabulations were used to summarize the descriptive statistics of the data.
Results
In this study, low birth weight (61.5%), preterm birth (57.7%), and low Apgar score at fifth minutes (53.9%) were the major identified adverse neonatal outcomes. Based on the multivariable logistic regression analysis, rural place of residence (AOR = 5.992 to 95% CI [1.011-35.809]), low monthly income (AOR = 4.364), middle monthly income (AOR = 4.364), and emergency cesarean section (AOR = 9.969) were the potential risk factors for adverse neonatal outcomes.
Conclusions
The adverse neonatal outcomes & the risk factors identified in this research have the potential to harm the health of the neonates. Thus, it needs emphasis to tackle the problems and save the life of the newborn through better and strengthened ANC follow-up, accesses to health care.
Background
Adverse neonatal outcomes have a significant effect on perinatal and neonatal survival, and mortality as well as the risk of developmental disabilities throughout future lives.1-3 Adverse neonatal outcomes are the major public health concern in developing countries.2,4-6 The adverse neonatal outcome is defined as the occurrence of Low Birth Weight (LBW), preterm delivery, low Apgar score at first and fifth minutes after birth, early or late neonatal death, small for gestational age, and/or severe neonatal conditions.7-9 LBW is defined as the delivery of a live infant whose birth weight is less than 2500 g. 10 Preterm delivery is defined as the delivery of a baby less than 37 weeks of gestation. 11 A low Apgar score at 5 minutes is defined as scoring less than 7.12,13 Small for gestational age (SGA) fetuses or newborns are those smaller in size than normal for their gestational age, most commonly defined as a weight below the 10th percentile for the gestational age.14,15 Neonatal death is defined as death within the first 28 days of life. 13 And Early neonatal death (ENND), defined as the death of a newborn between 0 and 7 day after birth. 16
Early neonatal death represents 73% of all postnatal deaths worldwide. 16 In 2013, over three-quarters of the newborn deaths in the world occur in Sub-Saharan Africa (SSA) and South Asia. Sub-Saharan Africa accounts for 38% of global neonatal deaths and it was about a third of under-five deaths occurred during the neonatal period.17,18 In the same year, 10 countries alone made up for two-thirds of the total annual number of neonatal deaths (1 760 000) and Ethiopia was the sixth position having a share of 84 437 neonatal deaths).19-21
Medical costs for newborns with adverse neonatal outcomes were significant compared to those without adverse outcomes. For example, the average expenditures for premature/low birth weight infants were more than 10 times as high as uncomplicated ones. Alike, LBW, low Apgar score, prematurity, and SGA were more than twice as costly as newborns without complications.22,23
Adverse neonatal outcomes present a very stressful, emotionally challenging, and traumatic event for parents that induces feelings of anxiety, helplessness, depression, and anger. Sleep disturbances are common in the 6 months after adverse neonatal outcomes occurred and may require short-term treatment with hypnotics or sedate antidepressants. Even a mother who had a previous adverse neonatal outcome may have high psychological stress in a subsequent pregnancy. Fathers have reported self-blame, a loss of identity as a father, and a need to hide their feelings after a perinatal loss.24-28
Globally, neonatal deaths among under-five deaths have increased from about 37% in 1990% to 44% in 2012.17,29 We can save 2 000 000 neonates each year if we end up with preventable newborn deaths.30,31 Therefore, it is possible to decrease under-five mortality by reducing neonatal mortality. 20
This study intended to assess the adverse neonatal outcomes and the associated risk factors because no research addresses the adverse neonatal outcomes and the associated risk factors in the study area.
Methods
Study Area
The study was conducted at randomly selected 5 hospitals of Mekelle city. Mekelle is the capital city of the Tigray region and is located about 783 km from Addis Ababa, the capital city of Ethiopia. Based on the census of 2007, it had a total population of 215 914 of which 104 925 were men and 110 989 women. In the same year, there were 60 998 reproductive age women groups (15-49 years). 32 The selected hospital had maternity (labor, delivery, and post-natal) and Neonatal Intensive Care Unit (NICU) services. Almost all of the hospitals are organized with Ultrasound, bags, and mask for resuscitation. Additionally, the public hospital had infant Incubators, C-PAP, Oxygen, antenatal corticosteroids, and oximetry in their neonatal intensive care units.
Study Design and Participants Characteristics
A hospital-based unmatched case-control study was conducted among 206 neonates with their index mothers in 5 randomly selected hospitals of Mekelle city. Neonates who had 1 or more adverse neonatal outcomes with their indexed mothers were included as cases and neonates who did not have adverse neonatal outcomes were included as controls with their index mothers. To assign neonates as having adverse neonatal outcomes, the medical cards were reviewed at the time of assessment and diagnosis. Since taking the newly diagnosed neonates as cases; reducing recall biases related to neonatal characteristics. 33 Sociodemographic, potential neonatal risk factors, and clinical data were obtained through face-to-face interviews with the mothers of the neonate and medical records. Those mothers of neonates who had serious medical conditions, who gave birth at home, had incomplete newborn record information, and had fetal death before 28 weeks of gestation were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined using Open Epi version 3.5.1 sample size calculator for unmatched case-control study design by taking 80% power of the test, 95% confidence level, a case to control the ratio of 1:3, and worth detecting odds ratio of 3.8 with the proportion of controls exposure of 9.3% 34 and 10% non-response rate. Based on the above assumptions, the total sample size required for this study was 208 of which 52 cases and 156 controls.
Those neonates who were diagnosed with adverse neonatal outcomes were selected consecutively until the desired sample size was obtained. For each case, 3 controls were selected (control to case ratio of 3:1) to reduce confounding in the sampling design. The selected controls were without any adverse outcomes. The phone numbers of all study participants were taken anonymously and neonatal deaths that occurred after discharge were traced back.
Measurement and Data Collection Procedure
A pretested, structured, and standard interview guide, which was adopted from different kinds of literature,7,9 was employed to collect data on the sociodemographic, obstetric, gynecologic, and postpartum information from the indexed mothers of the cases and controls in the delivery, inpatient, and postnatal units. Retrospective hospital record reviews were conducted at the delivery, post-natal, inpatient, and neonatal intensive care unit to obtain data on the newborn information relevant to the study. Ten B.Sc. nurses were recruited as data collectors and 2 M.Sc. holders were enrolled as supervisors.
Data Quality Management
To ensure the quality of data, the questionnaire was first prepared in English and translated into the local language (Tigrigna) then back to English to ensure its consistency. Three days of training were given for the data collectors and supervisors about the purpose of the study, methods of data collection, ethical issues, and sampling procedures. The questionnaire was pretested on 10% of the participants before actual data collection. Findings from the pretest were utilized to check the clarity, sensitiveness, ambiguity, arrangement, order, options, and skipping patterns of questions accordingly. Each questionnaire was checked during the data collection period by the principal investigator and supervisors on daily basis to see its completeness and clarity. Two data clerks did double data entry and the consistency of the entered data was cross-checked by comparing the 2 separately entered data. Before analysis, the data were cleaned thoroughly to check for completeness and errors during collection.
Data Processing and Analysis
The raw data were checked for completeness and cleanness. Then entered into Epi Info version 7 and exported to SPSS Windows software version 23 for analysis. Logistic regression analysis was performed to identify risk factors for adverse neonatal outcomes. Bivariate logistic regression was employed to see the association of each variable with dependent variables. Independent variables with a P-value of less than .2 in the bivariate logistic regression were entered into multivariate logistic regressions to control the effect of confounding factors and for further analysis. Some of the adverse outcomes are risk factors for other outcomes, so we addressed them similarly to the above. Variables having a p-value of less than 5% were considered as having a significant association with the outcome variable in multivariate logistic regressions. Frequencies, mean, standard deviation, percentage, and cross-tabulations were used to summarize descriptive statistics of the data. The results were presented using tables, charts, graphs, and result statements.
Operational Definition
Low birth weight (LBW) is weighing of newborn less than 2500 g.2,35-39
Preterm birth is live birth before 37 completed weeks of gestational age.2,35-39
Small for Gestational Age (SGA) is the birth weight of a newborn less than the 10th percentile.2,36-40
Lower Apgar score is the score of newborn less than 7 scores at fifth minutes.2,35-39
Neonatal death is the death of a newborn between 0 and 28 days of life.2,35-39
The gestational age was confirmed using LMP or/and Ultrasound of the embryo or fetus in the first trimester (up to and including 13 6/7 weeks of gestation).40,41
Results
A total of 52 cases and 154 controls with their indexed mothers were involved in the data collection with a 99% response rate. Thus, 206 participants’ data were included in the analysis.
Study Participants Characteristics
Among the total mothers, 17 (32.7%) from the cases and 56 (36.4%) from the controls were in the age groups of 25 to 29 years with a mean age of 26.6 years and SD of ±6.153 years from the cases and 27.9 ± 5.265 years from the controls respectively. More than half of the cases, 28 (53.8%) and controls, 138 (89.6%) were urban dwellers and 24 (46.2%) cases and 16 (10.4%) controls were from the rural areas. Most of the mothers (96.2%, 98.1%, 73.1%, and 100.0% from the cases and 88.3%, 96.1%, 62.3%, 98.1% from the controls) were orthodox religion followers, married, housewives, and Tigray in ethnicity respectively. Above one-third of the cases (38.5%) and 47 (30.5%) of the controls didn’t attend formal education (Table 1).
Socio-Demographic Characteristics of the Study Participants in Hospitals of Mekelle City, Tigray Ethiopia, 2015 (n = 206).
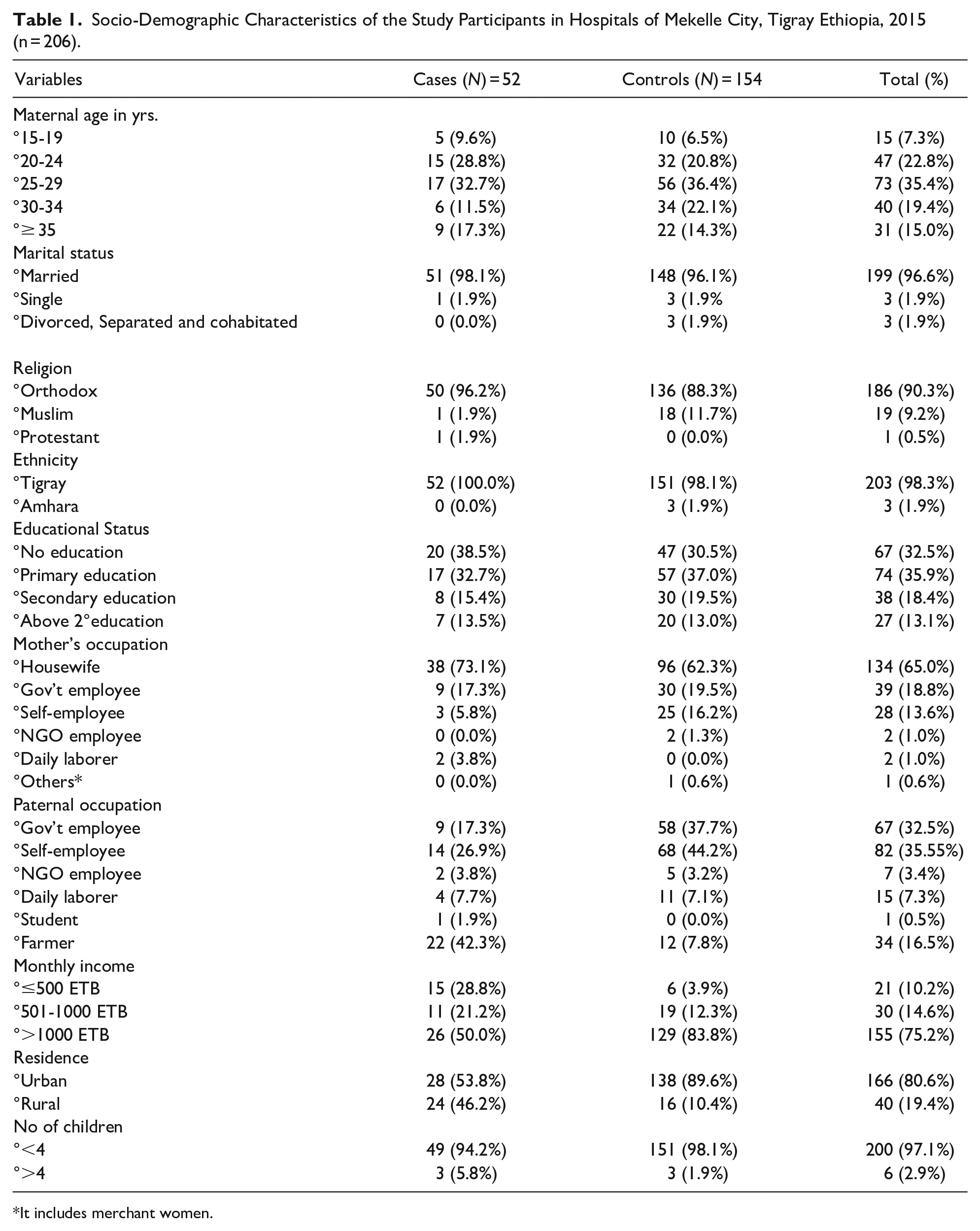
It includes merchant women.
Medical History of the Study Subjects
Respondents of 18 (34.6%) cases and 30 (19.5%) controls had experienced medical complications during the index pregnancy. Before the current pregnancy, the history of adverse neonatal outcomes was higher in the cases (6 [11.5%]) than the controls (4 [2.6%]). Likewise, history of STI (7.7%), syphilis (5.8%), and Urinary Tract Infection (UTI) (5.8%) were greater in the cases than controls ([7.1%], [4.5%], and [3.2%]). Among the total respondents, 5 (9.6%), 3 (5.8%), and 2 (3.8%) of the cases and 17 (11.0%), 6 (3.9%), and 2 (1.3%) of the controls were presented with anemia, pregnancy-induced hypertension (PIH), and Diabetes Mellitus (DM), respectively during the index pregnancy (Table 2).
Maternal Medical History of Cases and Controls in Hospitals of Mekelle City, Tigray, Ethiopia 2015. n = 206.

Px = Pregnancy to ANO = adverse neonatal outcome, BMI = Body mass index, Kg = kilogram to m2 = square meter, STI = sexually transmitted infection.
Pregnancy and Obstetric History of the Respondents
About 23 (44.2%) cases and 63 (40.9%) controls were primigravidas and 21 (40.4%) cases and 60 (39.0%) controls had a birth interval of 1 to 3 years. Multiple pregnancies have been reported in 8(15.4%) cases and 13 (8.4%) controls on the indexed pregnancy. Seven (13.5%) cases and 25 (16.2%) controls had unplanned pregnancies. The majority of respondents, 51 (98.1%) cases, and 149 (96.8%) control had a history of ANC visit but only 16 (30.8%) cases and 51 (33.1%) controls had 4 or more than 4 ANC follow-up (Table 3).
Pregnancy and Obstetric History of the Respondents in Hospitals of Mekelle City, Ethiopia, 2015. n = 206.
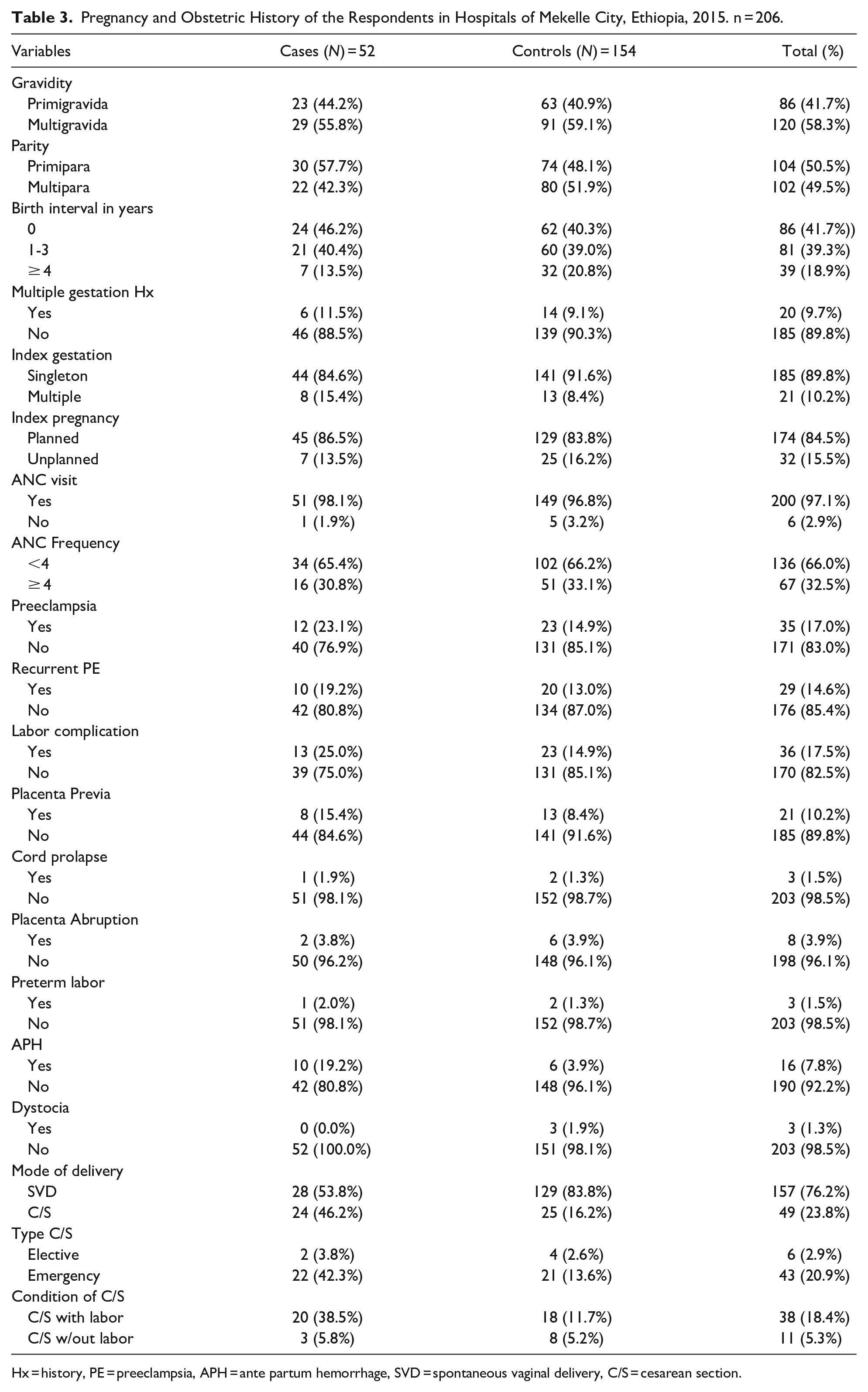
Hx = history, PE = preeclampsia, APH = ante partum hemorrhage, SVD = spontaneous vaginal delivery, C/S = cesarean section.
Labor complication, placenta previa, cord prolapse and placenta abruption had occurred among 13 (25.0%), 8 (15.4%), 1 (1.9%), and 2 (3.8%) cases and 23 (14.9%), 13 (8.4%), 2 (1.3%), and 6 (3.9%) controls respectively. On the other hand, Ante Partum Hemorrhage (APH) was observed in 10 (19.2%) cases and 6 (3.9%) controls respectively (Table 3).
Neonatal Characteristics of the Cases and Controls
Most of the cases (33 [63.5%]) and controls (136 [88.3%]) were within the age of 1 to 3 days followed by 4 to 6 days (cases 13 [25.0%] and controls 16 [10.4%]). Regarding the sex of neonates, female were higher in cases (31 [59.6%]) than controls (76 [49.4%]) but males were higher in controls (78 [50.6%]) than cases (21 [40.4%]). About 21 (40.4%) cases and 152 (98.7%) controls had a birth weight of 2.5 to 4.0 kg with mean birth weight (±SD) of 2.5 ± 0.63 to 3.14 ± 0.38 kg, respectively. An Apgar score of less than 7 at first and fifth minutes was recorded on 28 cases (53.9%). Congenital malformation has been seen among 2 (3.8%) cases (Table 4).
Neonatal Characteristics of Cases and Controls in Hospitals of Mekelle City; Tigray, Ethiopia, 2015. n = 206.

Min. = minute to Apgar = Appearance, pulse, grimace, activity, respiration; NICU = neonatal intensive care unit; SGA = small for gestational age.
Adverse Neonatal Outcomes Among Cases
In this study, different types of adverse neonatal outcomes were found in 52 cases. From them, near to two-thirds (61.5%) were low birth weight followed by preterm birth (57.7%) and a low Apgar score (53.9%). Neonatal deaths and small for gestational were observed in 5.8% to 3.9% cases respectively (Figure 1).

Adverse neonatal outcome among cases in hospitals of Mekelle City, Northern Ethiopia, 2015. n = 52.
Maternal Sociodemographics, Medical, Obstetric, and Neonatal Factors Associated With Adverse Neonatal Outcomes
In the final model (multivariate analysis), monthly family income, place of residence, and emergency cesarean section (C/S) were significantly associated with Adverse Neonatal Outcomes (ANO). On the contrary, maternal and paternal occupation, maternal educational status, previous history of adverse neonatal outcomes, and medical complications like hypertension, HIV, UTI, anemia, and malaria were not significantly associated with adverse neonatal outcomes.
Those mothers who earn monthly income ≤ 500 ETB (Ethiopian Birr) were 7.7 times more likely to have ANO (AOR = 7.647% to 95%( 1.545-37.84) than mothers who earn >1000 ETB. Likewise, mothers who earn 501 to 1000 ETB were 4.4 times more likely to have ANO (AOR = 4.364 to 95% CI (1.050-18.129) than mothers who earn >1000 ETB. Rural dwelling mothers were 6 folds more likely to have adverse neonatal outcomes (AOR = 5.992 to 95% CI (1.011-35.809) than urban dwellers. Similarly, the mode of delivery was significantly associated with adverse neonatal outcomes. In this case, neonates delivered by emergency C/S were 10 times more likely to have ANO than neonates delivered without emergency cesarean section (AOR = 9.969 to 95% CI(1.023-97.148) (Table 5).
Maternal Sociodemographic, Obstetric Health, and Neonatal Characteristics Factors Associated With Adverse Neonatal Outcomes in Hospitals of Mekelle City, Northern Ethiopia, 2015. (Cases = 52 to controls = 154).

NB. Blank space in the last column means variables not entered into final model &non-significant, reference indicated by 1, **P < .05, ***P < .0001, ****P = .001 to ANO = adverse neonatal outcome, Hx = history, Px = pregnancy, kg = kilograms.
Discussion
This study was performed to assess the adverse neonatal outcomes and associated risk factors in hospitals of Mekelle City, Tigray, Ethiopia. Adverse neonatal outcomes are the major neonatal health problem in Africa. 42 Low birth weight, preterm birth, neonatal death, small for gestational age, and low Apgar score were the adverse neonatal outcomes identified in this study. Likewise, similar findings were observed in Gondor-Ethiopia, Nkangala District-South Africa, Ontario-Canada, Mtwara regional hospital-Tanzania, and Hospital in Brisbane, Australia.43-47 The similarity might be due to the universality of the problem throughout the world population.
One of the adverse neonatal outcomes was neonatal death in this study. It was 5.8% which is small compared to low birth weight (61.5%), preterm birth (57.7%), and low Apgar score (53.9%).
Neonates born from mothers of rural residents were more likely to develop adverse neonatal outcomes than neonates of mothers from urban residences. This finding is analogous with Gamo Gofa Zone, Southern Ethiopia, New South Wales, and the Australian Capital Territory (ACT).48,49 This could be explained by the fact that women in rural areas are prone to laborious working during the time of pregnancy, unable to access health care easily due to geographical locations and this could lead to maternal complications and adverse neonatal outcomes.50,51
Lower and middle family incomes were also found significantly associated with adverse neonatal outcomes. Neonates born from mothers of lower family income were more likely to develop adverse outcomes than their socioeconomic counterparts. This is in line with another research done in Mtwara regional hospital, Tanzania, and Gondar, Ethiopia.46,52 The reason might be explained as lower financial capacity could be a limiting factor to afford nutritional supplements, food staff as well as visiting health care facilities that would benefit the health of the fetus during pregnancy.
The other factor that was significantly associated with adverse neonatal outcomes in this study was an emergency cesarean section. The same association has been observed in South African, Norway, India, and Australia.42,53-55 The reason might be due to obstetric complications. As obstructed labor could lead to emergency C/S and affect the outcome of the newborn.
Since this study used the newly diagnosed neonates as cases; it takes strength of reducing recall biases related to neonatal characteristics. Due to limited sample size in both comparative cases and controls, some maternal medical characteristics were not significantly associated in this study contrary to other studies. 33 A further comparative perinatal research should be done to identify possible risk factors and to come up with a solution to minimize adverse neonatal outcomes
Conclusions
The adverse neonatal outcomes and the risk factors identified in this research harm the future health of the neonate and the mothers. Thus, it needs emphasis to tackle the problems and save the life of the newborn through better and strengthened ANC follow-up accesses for health care, and income generation activities for all reproductive-age women in general and pregnant women in particular.
Strengths and Limitations
This study has a comparative strength in using incident than prevalent cases that could reduce recall bias and used a primary source of data that enable to include some baseline maternal and neonatal characteristic factors. The study tool was developed from the standardized and piloted instrument. As there was no the same study in the study area so that it can use as a baseline for other studies. It also helps to conduct an interventional study in the area.
On the contrary, there was a potential selection bias because only hospital births were included. The sample may not, therefore, be representative of all neonates in the country due to the small sample size.
Footnotes
Acknowledgements
We, the investigators, have thank to Mekelle University for the chance given to conduct this research. We would like also to thank the Tigray Regional Health Bureau and the hospitals of Mekelle City for their collaboration during the study period. We also thank the invitation of world neonatology and child care to present our paper. We are also very glad to be in a position to acknowledge Mr.Hayal Wubetu Mure for English editing to correct the grammar and flow of our manuscript. Our last but not least appreciation goes to all the data collectors, supervisors, and study participants without whom it would have been impossible to have complete work.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Availability of Data and Materials
The dataset used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Ethical clearance and approval were obtained from the research ethical review board (RERB) of the College of Health Sciences at Mekelle University. An official letter was given and permission was obtained from the Tigray Regional Health Bureau and was communicated with respective hospitals and got permission. All of the study participants were informed about the purpose of the survey, their right to participate or to terminate at any time if they want. Respondents’ information was kept confidential. Privacy was maintained and benefits like when neonates were found to be with adverse outcomes; data collectors and principal investigator facilitated and link for the care. After the purposes and the importance of the study were explained at all levels, informed oral consent, which was approved by the ethical committee, was obtained from each study subject before the interview. If participants were under the age of 16 years old, consent was obtained from the parents/guardians.
Consent for Publishing
Not applicable