
Abstract
Objectives:
To provide up-to-date data concerning hypertensive disorders of pregnancy on maternal and neonatal profiles in Indonesia.
Methods:
Retrospective clinical audit on all pregnancy-associated hypertensive women between 1 January 2020 and 31 March 2020 at Cianjur General District Hospital.
Results:
Preeclampsia accounts for 66.8% (235/352) of hypertensive disorders of pregnancy, gestational hypertension 29% (102/352) and chronic hypertension 4.3% (15/352). Compared to other pregnant women, those with preeclampsia, on average, had higher systolic and diastolic blood pressures and poorer kidney (ureum and creatinine) and liver function (aspartate transaminase enzyme and alanine transaminase enzyme) profiles (p < 0.001, < 0.001, < 0.001, 0.003, 0.033 and 0.002, respectively), and required more intensive care admission. Neonates from women with severe forms of preeclampsia (eclampsia and HELLP syndrome (haemolysis, elevated liver enzymes, low platelets)) had, on average, lower birthweight (p = 0.015 and 0.048, respectively) and birth length (p = 0.021, 0.017). Neonates from eclamptic mothers had poorer APGAR (appearance, pulse, grimace, activity and respiration) scores (p = 0.006 and 0.005, respectively).
Conclusion:
Hypertensive disorders of pregnancy exerts adverse maternal and neonatal outcomes, particularly among eclampsia and HELLP-syndrome neonates. Various challenges remain for optimal management.
Keywords
Introduction
Hypertensive disorders of pregnancy (chronic hypertension, gestational hypertension and preeclampsia) exerts significant maternal and neonatal morbidity and mortality, particularly in developing countries. 1 The maternal and neonatal morbidities range from cardiovascular, hepatic, renal to respiratory and central nervous system abnormalities. 2 In a 2013 international report involving 43,364 women, there was an 8.6% incidence rate for preeclampsia and 2.5% for eclampsia. 3 Hypertensive disorders of pregnancy has multiple risk factors: history of hypertension, pregestational diabetes, multiple gestation, prior preeclampsia, nulliparity, assisted reproductive technology and being overweight/obese pre-pregnancy. 4 Genetics is also important as history of preeclampsia in first-degree family members confers women a fourfold risk of developing preeclampsia. Men born of preeclamptic mothers are at an increased risk of fathering preeclamptic pregnancies themselves. 5
Hypertensive disorders of pregnancy may lead to long-term maternal complications such as future cardiovascular and end-stage renal diseases. 6 There is an increased vulnerability for future cardiovascular diseases, cerebrovascular accidents, venous thromboembolism, end-stage renal diseases and diabetes mellitus. 6 Neonates are at increased risk of being delivered prematurely and suffering from prematurity-related complications, including respiratory distress syndrome (RDS) and sepsis. 7 Abnormal placentation also leads to possible intrauterine growth restriction (IUGR), resulting in higher small-for-gestational age (SGA) neonates, neonatal intensive care admission, sepsis and apnea.8–10
Unfortunately, few recent data have been published on the maternal and neonatal profiles of hypertensive disorders of pregnancy in Indonesia. 11 Only few have been published for West Java and none for our district (Cianjur). We hope this study will fill that gap and stimulate further studies, particularly on improving its prevention and screening at the primary healthcare level.
Methods
This was a retrospective analytical study on women presenting with hypertensive disorders of pregnancy to Cianjur General District Hospital. The women presented to our Accident and Emergency department and outpatient clinics between 1 January 2020 and 31 March 2020 and were subsequently treated. Patients were recruited by consecutive sampling. We included all women presenting with hypertensive disorders of pregnancy. However, we excluded women under the following criteria:
Patients’ hand-written case notes were irretrievable from the medical records department.
Patients’ medical records numbers did not match those in the patient register, even after attempted secondary confirmation from the patient names and/or date of birth.
Women were not treated for hypertensive disorders of pregnancy.
Missing data for the majority of both maternal and neonatal variables.
Individual patient case notes were retrieved and reviewed by the team. Maternal data were collected: patient demographics, clinical and laboratory data, diagnosis, management, complications, intensive care admission, and vital signs at discharge. Neonatal data were collected: gestation length, viability, sex, birthweight, birth length, and 1- and 5-min APGAR (appearance, pulse, grimace, activity and respiration) scores. If data on the above variables were missing, they were labelled ‘not available’.
The following definitions from the International Society for the Study of Hypertensive disorders of pregnancy guideline were used 1 :
Hypertension: systolic blood pressure (BP) ⩾ 140 mm Hg and/or diastolic BP ⩾ 90 mm Hg. 1
Chronic hypertension: hypertension existing prior to pregnancy and/or first diagnosed < 20 weeks of gestation. 1
Gestational hypertension: persistent and de novo hypertension first diagnosed ⩾ 20 weeks of gestation without features of preeclampsia. 1
Preeclampsia: gestational hypertension accompanied by at least one of the following features
1
: Proteinuria (presence of protein for at least +1 in urine dipstick test). Acute kidney injury (creatinine ⩾ 1 mg/dL). Neurological complications (eclampsia, stroke, severe headache). Haematological complication (platelets ⩽ 150,000/µL, haemolysis). Uteroplacental dysfunction (foetal growth restriction, stillbirth).
HELLP syndrome: a collection of findings constituting of haemolysis, elevated liver enzymes (alanine transaminase (ALT) and/or aspartate transaminase (AST)) and low platelets, which form a severe form of preeclampsia.
Eclampsia: a new onset of a generalised seizure during pregnancy and/or postpartum in women with signs of preeclampsia.
The ethical approval for this study was granted by the Research Ethics Committee of Universitas Padjadjaran with registration number 651/UN6.KEP/EC/2020. This study received no external funding. This study has been prepared according to the STROBE statement and checklist.
Statistical methods
The reported incidence of preeclampsia ranged from 3% to 10% according to the literature, and we predicted an incidence of pregnancy-induced hypertension of at least 3% in our population. 12 By adopting a 80% with a probability of type 1 error of 5%, we measured that at least 259 subjects would be required for this study.
Descriptive statistics were provided for both categorical and continuous variables, where appropriate. Different diagnoses of hypertensive disorders of pregnancy (preeclampsia, gestational hypertension, chronic hypertension, eclampsia, HELLP syndrome) were categorised and analysed. Analytic statistics were performed: continuous variables were compared in two groups using the Mann–Whitney U test, and in three groups using the Kruskal–Wallis test. If the Kruskal–Wallis test was significant, pairwise Mann–Whitney U tests employing the Bonferroni correction to the p-value were used to determine which groups differed. Categorical variables were analysed by Fisher’s exact test or the chi-squared test depending on minimum sample size requirements. The significance level was set at 0.05.
Data were entered into a customised database on Microsoft® Excel for Mac v16.16.3 (Microsoft®, Redmond, USA) and analysed using Statistical Product and Software Solutions (SPSS) for Mac v.23 (IBM Corp, Armonk, New York, USA).
Results
Initially, 411 women were recorded from the patient register; 37 were excluded due to irretrievable case notes, 17 were excluded as they were not treated for hypertensive disorders of pregnancy, 4 were excluded due to data mismatch in patient register, and 1 was excluded for grossly missing maternal and neonatal variables. A total of 352 women were eventually enrolled (Figure 1).
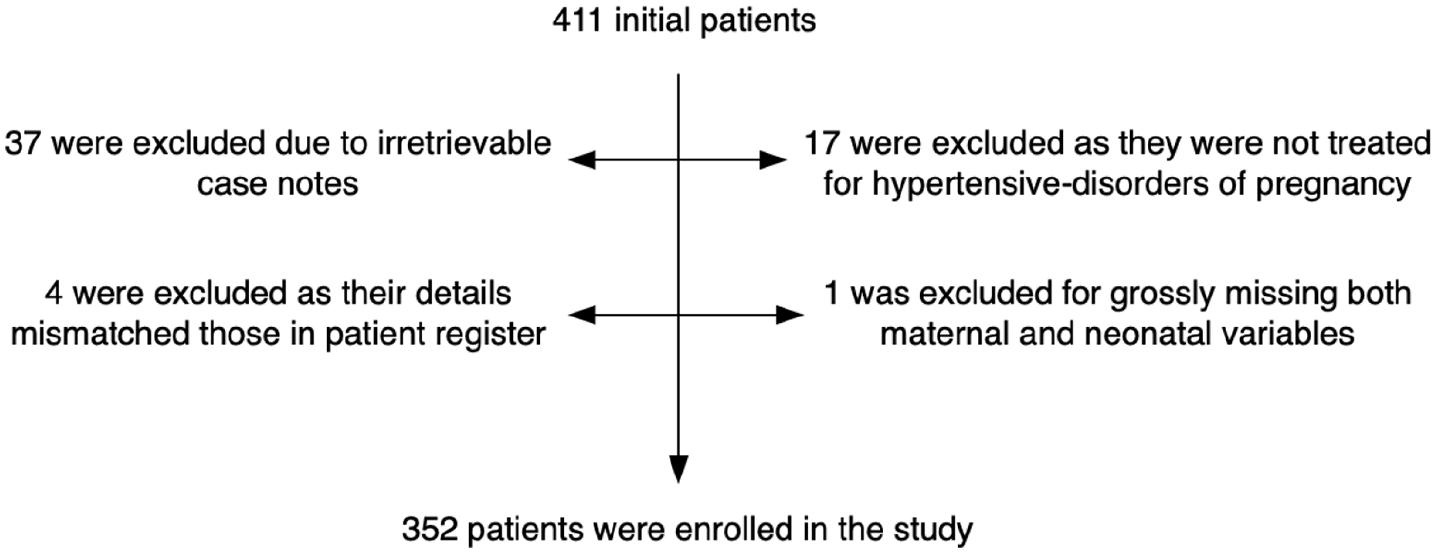
Patient enrolment chart.
Table 1 lists the demographic profile of our women and their neonatal outcomes. Of 352 women, 66.8% (235/352) suffered from preeclampsia, 29% (102/352) from gestational hypertension and 4.3% (15/352) from chronic hypertension. The median age at presentation was 30 (range: 13–49) years and there was no statistically significant difference across the different diagnoses (p = 0.319). In all, 96% (338/352) were housewives; 20.5% (72/352) had a history of hypertension and there was no statistically significant difference between preeclampsia and non-preeclampsia groups (p = 0.402); 53.3% (185/347) women had undergone at least 1 antenatal ultrasound examination (USG). While not all women had recorded the age at which they got married, of the 318 available data, the median age was 20 (range: 9–36) years; 7.4% (26/352) women were ⩽19 years and 33.5% (118/352) women were ⩾35 years.
Demographics of patients with pregnancy-associated hypertension and neonatal outcomes across three groups.

USG: ultrasonography; BP: blood pressure; ALT: alanine transaminase enzyme; AST: aspartate transaminase enzyme; SBP: systolic blood pressure; DBP: diastolic blood pressure; Hb: haemoglobin. The percentages shown are row percentages. Column percentages are not available.
Women with preeclampsia had higher median systolic and diastolic BP compared to gestational hypertension group on post hoc pairwise comparison (p < 0.001 and p < 0.001, respectively). The median Hb level was 11.7 g/dL with 32.4% (111/343) women’ Hb < 11 g/dL. The preeclampsia group showed statistically significantly higher median values for both kidney (ureum and creatinine) and liver function tests (AST and ALT) (p < 0.001, p = 0.003, p = 0.033, p = 0.002, respectively). A post hoc pairwise comparison revealed that the significant relationship was between the preeclampsia and gestational hypertension groups (p < 0.001, p = 0.005, p = 0.087, p = 0.006). Among women with preeclampsia, only 70.8% (165/233) women received MgSO4 as an anticonvulsant.
There was no significant association between preeclampsia and the method of delivery (p = 0.536). The median systolic and diastolic BPs at discharge were not significantly different across the different diagnoses (p = 0.394 and 0.116, respectively); 43.2% (152/352) women had BPs at discharge exceeding 135/85 mm Hg. The median interval between intervention and discharge was 2 days (range: 0–7 days) with gestational hypertension women spending 1 less inpatient day, on average (p = 0.045); 4.5% (16/352) women required intensive care admission and all were suffering from preeclampsia.
Among 19/352 (5.4%) women suffering from eclampsia, the median frequency of seizures was 2 (range: 1–16) with median systolic and diastolic BP during seizure being 160 (range: 140–240 mm Hg) and 100 mm Hg (range: 63–130 mm Hg), respectively. In all, 57.9% (11/19) women developed eclampsia pre-labour, 10.5% (2/19) during labour, 15.8% (3/19) post-labour while 15.8 (3/19) women did not have their seizure timings recorded.
In all, 2.6% (9/352) women suffered from HELLP syndrome. Their median ALT and AST values were 69 (range: 17–187) and 103 (range: 14–434), respectively. Their median platelet count was 110,500 (range: 49,000–254,000).
The median gestational length was 38.57 weeks (range: 20–45) with 76.1% (229/318) neonates delivered at term; 91.8% (290/316) neonates were viable (Table 2). There was no significant relationship between foetal sex and preeclampsia development (p = 0.812). The median birthweight was 3000 grammes (range: 100–5100), and the median birth length was 49 cm (range: 24–57). The birthweight and birth length were not statistically significantly different across the different diagnoses (p = 0.084 and 0.082, respectively). The median 1- and 5-min APGAR scores were 5 (range: 0–5) and 7 (range: 0–9). They were not significantly different across the different diagnoses (p = 0.202 and 0.342, respectively).
Overall neonatal outcomes.

IUFD: intrauterine foetal death; APGAR score: a neonatal assessment score consisting of appearance, pulse, grimace, activity and respiration.
Table 3 lists the neonatal outcomes of eclampsia and HELLP-syndrome mothers. Among women with eclampsia, 16 neonates were born: 7 preterms and 9 terms. The median gestation length was not different from the rest of the group (p = 0.757). Thirteen neonates were viable, 2 died intrauterine and 1 was stillbirth. Sex was recorded only for 13 neonates: 5 males and 8 females. The neonates had significantly lower birthweight (p = 0.015), birth length (p = 0.021), and 1- and 5-min APGAR scores (p = 0.006 and 0.005, respectively) than the rest of the group.
Neonatal outcomes of eclampsia and HELLP-syndrome mothers.

HELLP syndrome: haemolysis, elevated liver enzymes, low platelets syndrome; APGAR score: a neonatal assessment score consisting of appearance, pulse, grimace, activity and respiration.
Neonates from mothers with HELLP syndrome had significantly lower birthweight and birth length compared to all others (p = 0.048 and 0.017, respectively).
Discussion
Among our patients, the median age at presentation was 30 years while median marital age was 20 years. More than 40% of our women had delivered at too young and/or too advanced maternal ages (7.4% were ⩽19 years and 33.5% women were ⩾35 years, respectively). Unfortunately, there has been ample evidence that childbirth at young (⩽19 years) and advanced (⩾35 years) maternal ages is associated with increased risks for adverse perinatal outcomes, including preterm deliveries, low birthweights and preeclampsia.13,14
This is certainly contributed by the young ages at which our women got married. Adolescent marriage remains widely prevalent in Indonesia and 47.3% (150/317) of our women had married below the median age of 20 years. 15 An urgent yet long-term improvement of the district’s family planning programme to reduce such high-risk pregnancies is therefore necessary.
In our population, previous hypertension did not influence the development of preeclampsia (p = 0.402). This is unexpected and might have been due to our lack in specifying the type of hypertension in our women. 16 Another reason might have been the lack of similar rigorous standards in diagnosing hypertension. As a personal observation, some midwives would measure their women’ BP by palpation only, which would have led to gross inaccuracies in BP reading.
In all, 46.7% women did not have USG and unfortunately, the women’ arguments for not having one went unrecorded. A possible cause is the lack of agreement between World Health Organization (WHO) and our national guideline.17,18 In Peraturan Menteri Kesehatan no 97 of 2014, 17 USG was only for specific indications and the attending physician and/or midwife at the primary healthcare centre might not have recommended for a scan if routine antenatal care (ANC) visits had elicited no issues. However, most hypertensive disorders of pregnancy would have been detected in either the second or third trimester visit, prompting USG referral. Further studies examining the low USG uptake should therefore be undertaken.
More than 30% of women suffered from anaemia. While lower than the national average of 42%, anaemia in pregnancy constitutes an independent risk factor for maternal preeclampsia, eclampsia and low birthweight, prematurity and stillbirth among our neonates. 19
We did not observe any significant differences in the systolic and diastolic BP at discharge across the different diagnoses. This is expected as the definitive solution for hypertensive disorders of pregnancy is through delivery. 7 The median BPs were below the recommended BP targets of <135/85 mm Hg. 20 However, we had failed to manage the BP well in 40% of women as they were discharged with their BPs not brought under control with two women’s BPs still in hypertensive crisis range. 21
Women with preeclampsia and chronic hypertension spent more time at the hospital than those with gestational hypertension. This is an expected finding but we fell short of observing the women for ⩾72 h post-intervention as they remained at high risk for complications. 22
All 16 women requiring intensive care were suffering from preeclampsia and 62.5% (10/16) were admitted due to eclampsia. This matches Lal et al.’s 23 study in which eclampsia significantly outnumbers preeclampsia for maternal intensive care admission.
Across the different diagnoses, there was no statistically significant difference in the gestational lengths, birthweights, birth lengths, and 1- and 5-min APGAR scores. This is unexpected as abnormal placentation in preeclampsia may cause IUGR. Despite lacking such information, this might have been due to the majority of preeclampsia being late-onset preeclampsia (LOP) rather than early onset preeclampsia (EOP). EOP is associated with poor placentation and unremodelled spiral arteries while in LOP, congested placenta amid normal placentation. 24
There was no foetal sex influence on the development of preeclampsia. This is in agreement with Jaskolka et al. 25 This suggested that race-specific factors, rather than merely foetal sex, influence preeclampsia-eclampsia development.
Neonates from mothers with eclampsia had significantly lower birthweight, birth length and poorer APGAR scores than the others. This is due to eclampsia being a more severe form of preeclampsia with eclampsia neonates being delivered earlier, had lower birthweight, more acidic cord arterial pH, poorer 5-min APGAR score, more neonatal intensive care admission, respiratory distress and seizures. 23
HELLP syndrome is a continuum of preeclampsia. Our hospital lacked lactate dehydrogenase (LDH) measurement and could only diagnose partial HELLP syndrome from elevated liver enzymes and/or thrombocytopenia. 26 Partial and complete HELLP syndrome produce similarly adverse maternal and neonatal outcomes as HELLP-syndrome placentas had more vascular and villous lesions consistent of placental malperfusion.26,27 Partial HELLP-syndrome neonates had lower birthweights and birth lengths compared with the rest. Upon further analysis among only neonates from mothers with preeclampsia, partial HELLP-syndrome neonates still had significantly lower birth length.
There were 17 intrauterine foetal deaths (IUFDs) with 70.6% (12/17) deaths from preeclampsia group. Our results are in agreement with a Norwegian cohort in which chronic hypertension, gestational hypertension and preeclampsia are respectively associated with increasing risks of foetal death. 28
The APGAR scores are conveniently used for a standardised assessment for neonates after delivery. 29 A 5-min APGAR score of 7–10 is reassuring, 4–6 moderately abnormal and 0–3 low. 29 Our median 5-min APGAR score is 7 but out of 139 neonates in the reassuring group, only 1 reached 9. Ninety-six neonates were moderately abnormal. This odd APGAR scores distribution warrants further questions. It is suspected that the attending nurse/midwife might not have adhered strictly to the standardised APGAR scoring system. Instead, they may have arbitrarily assigned a particular set of APGAR scores based on a quick glance of the neonate’s condition at birth. Such assumption is worrying.
The challenges of our study are common to those in other developing countries, such as India. India also suffers from lack of studies on preeclampsia. 30 They also suffer shortage of real-time data as their national data are reported only every 4–5 years. 30 Furthermore, India resembles Indonesia by having a similar healthcare infrastructure with primary healthcare centres forming the backbone of its healthcare system. 30 Several issues pertaining to hypertensive disorders of pregnancy in India are highlighted below.
In India, ANC non-attendance and hence, lack of proper ANC is a huge risk factor for preeclampsia. 30 From our 46.7% USG non-attendance rate, many of our women may not have had proper ANC themselves. In India, many midwives also measured BP by palpation alone and this would only measure the systolic BP. 31 Worryingly, this practice is similar to our findings. We also noted a terminal digit preference (TDP) from observing our nurses and midwives when they measured the patients’ BPs. 32 TDP distorted the patients’ true measurements. 32
Sachan et al. 33 discovered that preeclampsia and eclampsia women were more likely to have higher BP measurements, more maternal complications and adverse neonatal outcomes, similar to ours.
This study has several strengths. First, we are the first to study hypertensive disorders of pregnancy in our district and among the few in Indonesia in the last 5 years. Second, it is based at a large secondary hospital with >1300 cases of hypertensive disorders of pregnancy annually. Third, this audit used data from the first 3 months of 2020, representing the current disease burden and management plans for hypertensive disorders of pregnancy in our district.
However, our study also has limitations. First, this is a retrospective study and despite examining very recent data, incomplete patient case notes reduced the quality of our data. For example, we could not analyse the impact of smoking and body mass index (BMI) in this study as many records were missing such data. Second, around 15% of women had to be excluded due to unavailable or missing case notes.
Third, there is a selection bias: we received few women from the southern part of Cianjur district due to the long distance and lengthy travel times. Fourth, our data suffered from lack of details (e.g. history of hypertension) and suspected underachievement of the clinical team (e.g. APGAR score). For example, there had been no standardised practice at our facility to gather complete information on patients’ previous history of hypertension, if such history existed. This led to scant data on previous history of hypertension, which made determining if the preeclampsia was superimposed on chronic hypertension especially challenging.
Conclusion
Hypertensive disorders of pregnancy is associated with adverse maternal and neonatal outcomes. Lack of consistency between national and international guidelines, deliveries at high-risk age groups, anaemia in pregnancy, and both hospital and clinical team shortcomings constitute some of the reasons why proper management of hypertensive disorders of pregnancy is still a huge challenge in our district.
Footnotes
Acknowledgements
The writers would like to thank Eric Jauniaux, MD, PhD, FRCOG, for his valuable input in the preparation of this manuscript.
Author Note
Aria Yusti Kusumah is now affiliated to Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia.
Author contributions
K.D.T. conceived and designed the study. K.D.T., Ar.Y.K., Az.Y.K., D.I.P., M.R.A. and S.P.S. acquired the data. K.D.T. and A.P. analysed the data and interpreted the data. T.D. contributed to data interpretation. K.D.T. drafted the manuscript. All authors contributed to the drafting of the article and agreed on the final version to be published. All authors agree to be accountable for all aspects of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study was granted an ethical approval by the Ethical Review Board of Universitas Padjadjaran under the following registration number: 651/UN6.KEP/EC/2020.
Informed consent
Written informed consent was not obtained from all subjects before the study because we used secondary data from medical records, not requiring patient consent.
Guarantor
K.D.T.