
Abstract
The adverse neonatal outcome is defined as the presence of birth asphyxia, respiratory distress, birth trauma, hypothermia, meconium aspiration syndrome, neonatal intensive care admission, and neonatal death. It is a major concern in developing countries, including Ethiopia. This study tried to identify predictors of adverse neonatal outcomes at selected public hospitals in Eastern Ethiopia. A hospital-based prospective follow-up study was conducted in three public hospitals in Eastern Ethiopia from June to October 2020. A total of 2,246 laboring women and neonates born at the hospitals were enrolled in the study. Data were collected through interviews, observation checklists, and clinical chart review. Reports were presented in relative risks with 95% CIs. The overall magnitude of adverse neonatal outcome was 20.97% (95% CI: 19.33- 22.71%). It was 24.3% for babies born through cesarean section (95% CI: 21.3%, 27.5). The presence of meconium in the amniotic fluid increased the risk for neonates delivered via cesarean section (ARR, 1.52 95% CI; 1.04, 2.22). Among neonates born via vaginal delivery, the risk of adverse neonatal outcome was higher among nullipara women (ARR, 1.42 95% CI; 1.02, 1.99) and among women diagnosed with abnormal labor or pregnancy such as APH, pre-eclampsia, obstructed labor, fetal distress, and mal-presentation at admission (ARR, 1.30 95%CI; 1.01, 1.67). The risk of adverse neonatal outcome was higher among babies born through the cesarian section than those born via vaginal delivery. Abnormal labor or pregnancy and being primiparous increased the risk of adverse neonatal outcome in vaginal delivery.
Keywords
Introduction
Globally, Nearly 2.5 million infants died in the neonatal period in 2019, with approximately 7,000 neonatal deaths every day and 1 million death on the first day of birth. 1 South Asian and Sub-Saharan countries contributed 79% to the deaths. Neonates born in those countries are nine times more likely than neonates born in high-income countries to die during the first month of life. 2 An adverse neonatal outcome such as birth asphyxia, low Apgar score, respiratory distress (RD), birth trauma, hypothermia, and meconium aspiration syndrome (MAS) significantly contribute to neonatal mortality, and mortality.3-6
The cascades of adverse birth outcome usually start with birth asphyxia, a common complication that can occur before, during, or after birth. 7 In Africa, 24% of neonatal deaths were due to birth asphyxia, 8 and it is also a leading cause of brain damage. 7 Factors related to birth asphyxia can arise in the antepartum and intrapartum periods. Conditions during pregnancy such as inadequate antenatal follow-ups, complications, low birth weight, gestational age of less than 37 weeks, and multiple births contribute to asphyxia.9-11 Premature rupture of membrane (PROM), prolonged labor, meconium stain-amniotic fluid, and fetal distress were intrapartum factors.12-14 Low Apgar scores at the fifth minute are associated with mortality and may cause an increased risk of cerebral palsy.5,15,16 Prolonged labor, low birth weight, pregnancy-induced hypertensive disorders, cesarean delivery, and meconium-stained liquor were identified determinants for low five-minute Apgar score.17,18
Nearly 10 to 15% of neonates are born through meconium-stained liquor, of which 3 to 9% develop meconium aspiration syndrome (MAS). 19 MAS predisposes neonates to severe asphyxia, severe respiratory distress, and admission to the neonatal intensive care unit (NICU). It is also a cause of death.20,21 It occurs in 8-47.6% of neonates in African countries and is the leading cause of NICU admission.22-27 Gestational age, birth weight, and CS delivery are risk factors for respiratory distress, 28 whereas induced labor, prolonged labor, and cesarean birth are the risk factors for MAS. 29
Recently, CS delivery is increasing globally, with the justification of reducing maternal and neonatal morbidity and mortality. 30 However, studies indicate that most adverse neonatal outcomes are common in CS delivery than the natural way of giving birth.28,29,31
The adverse neonatal outcomes are the major causes of neonatal mortality and mortality in developing countries. Reduction of neonatal mortality is one of the targets in the third Sustainable Development Goal in the country. Ethiopia is striving to decrease neonatal mortality by more than half from the current status. Achieving such a target is a challenge for the country in the given condition. Identifying risk factors for adverse neonatal outcomes, associated with the mode of delivery, might help in devising a strategy to reduce the burden of the problem. This study tried to assess predictors of adverse neonatal outcomes at four public hospitals in eastern Ethiopia.
Method
Study design, setting, and period
A hospital-based prospective follow-up study was conducted at public hospitals in Eastern Ethiopia from June to October 2020. The hospitals included in the study were from East Hararghe (Oromia region), Harari region, and Dire Dawa City Administration. There were nine government hospitals in the study area altogether, one specialized hospital (Hiwot Fana Hospital), one referral hospital (Dil Chora hospital), five general or secondary hospitals, and two primary hospitals. In this study, Hiwot Fana and Jegal Hospital from Harar, Dil Chora Hospital from Dire Dawa, and Bisidimo Hospital from East Hararghe were included.
Population, Inclusion, and exclusion criteria
Women who have visited the hospitals for delivery were included with their babies. Women who gave birth at home or other facilities and visited the hospitals for the management of complications were excluded. Women with critical medical conditions and those with known intrauterine fetal death were excluded from the study.
Sampling techniques and sample size determination
The sample size was calculated with the assumption of 95% CI with the power of 80, comparison of operative vaginal delivery and spontaneous vaginal delivery with the outcome of major trauma of the newborn p1 = 1.4, P = 0.2, 32 that yield a sample size of 2042. With a 5% loss to follow up, the total sample was 2,246. In the previous six months, 7,536 delivery were registered in the selected hospitals. The sample size was proportionally allocated to each hospital, and systematic random sampling was used to determine the study participants (N/n = 7536/2246 = 3.35). Every third woman was included in the study, in which the first woman was chosen using the lottery method. 33
Enrollment and Follow-up
The women who fulfilled the inclusion criteria were included after giving their written consent. The cohort identification number was given to all participants. The necessary baseline information was collected using interview and chart review at admission. Follow-up was done from entry to discharge. The follow-up was done during labor and delivery, and all neonatal outcomes were recorded. For those who were admitted to NICU, the follow-up was continued until discharged from the unit or dead. 33
Data Collection and instrument
The questionnaire contains socio-demographic characteristics, past and current obstetric history, and labor and delivery information. These include age, marital status, religion, ethnicity, residence, educational level, current occupational status, wealth index questions, parity, current and previous obstetric history, ANC, past history of previous CS, history of stillbirth, birth interval, PROM, gestational age, and mode of delivery. The wealth index was assessed using a wealth index questioner developed by the ministry of health, and different tools were used to evaluate newborn outcomes. WHO Classification of Breathing Difficulty 34 and Acute Care of At-Risk Newborns (ACoRN) Score, 35 was employed to assess Neonatal Respiratory Distress. The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) WHO definition was used to diagnose birth Asphyxia 36 and Apgar score. Acute Care of At-Risk Newborns (acorn) score was used to assess respiratory distress. 35 Other outcomes such as hypothermia, MAS, and feeding difficulty were assessed using history and physical examination. Trauma was diagnosed by senior physicians. Fetal and neonatal characteristics included mal-presentation, position, sex, and weight developed through literature review. 35 The rate of NICU admission, need for respiratory support, and hospital stay was recorded by using a checklist. Five female midwives and two neonatal nurses selected from respective hospitals collected the data. Data gathering was supervised by the research team. A structured questionnaire, translated into local languages (Amharic Afan Oromo and Somali), was used to gather the information.
Data Quality Assurance
Pretested and validated tools were used for the collection of the data. Instruction on filling the questionnaire and carrying out the interview was given to data collectors during the training. Completeness and consistency were checked daily. Trainings on data collection methods and refreshment on neonatal resuscitation were given to data collectors and supervisors for four days. The principal investigator used to check the daily data collection processes and related activities by random spot-checking of the questionnaire to ensure their reliability.
Data Processing and Analysis
Proportions of adverse neonatal outcomes were put by mode of delivery. Vaginal delivery includes spontaneous vaginal delivery and instrumental vaginal delivery, while cesarean section includes emergency and elective CS. Modified Poisson regression37,38 was used to explore the predictors. Crude risk ratios (CRRs) and adjusted risk ratios (ARRs) with 95% CI were used to report the results. The Coefficients’ covariance matrix was checked to test multicollinearity.
Adverse neonatal outcome: Neonates diagnosed with either of the following: asphyxia, RD, birth trauma, hypothermia, MAS, NICU admission, neonatal death were considered adverse neonatal outcomes.
Birth trauma is damage that occurs as a result of physical pressure during the birthing process, usually during transit through the birth canal. 39
Meconium aspiration syndrome (MAS): A condition caused by inhalation of meconium into the lung of a fetus or newborn, usually due to vigorous respiratory movements during difficult parturition or respiratory system abnormalities. 40
Birth asphyxia: - Failing to initiate and sustain breathing at birth. 40
Respiratory distress: Respiratory distress in the newborn is recognized as one or more signs of increased work of breathing, such as tachypnea, nasal flaring, chest retractions, or grunting. 41 Hypothermia: is defined by the World Health Organization as a core temperature < 36.5° C (97.7° F). 42
Ethical Consideration
Ethical clearance was obtained from the Institutional Health Research Ethical Review Committee (Ref.no. IHRERC/107/2020), at the college of Health and Medical Science, Haramaya University. The purpose, procedure and duration, possible risks, and benefits of the study were explained through the local language, Afan Oromo. Then individual informed, voluntary, written, and signed consent was obtained from each participant.
Results
Socio-Demographic Characteristics of the Participants
Muslim by religion (75.3%), of Oromo by ethnicity (73.2%), had a minimum of primary education (36.69%), and were housewives (71.6%) (Table 1). Forty-six percent of cesarean section was attended at Hiwot Fana specialized university hospital, followed by Dilchora hospital (31.90%).
Pregnant Woman Enrolled in the Socio-Demographic Study Characteristic, Eastern Ethiopia, 2020.
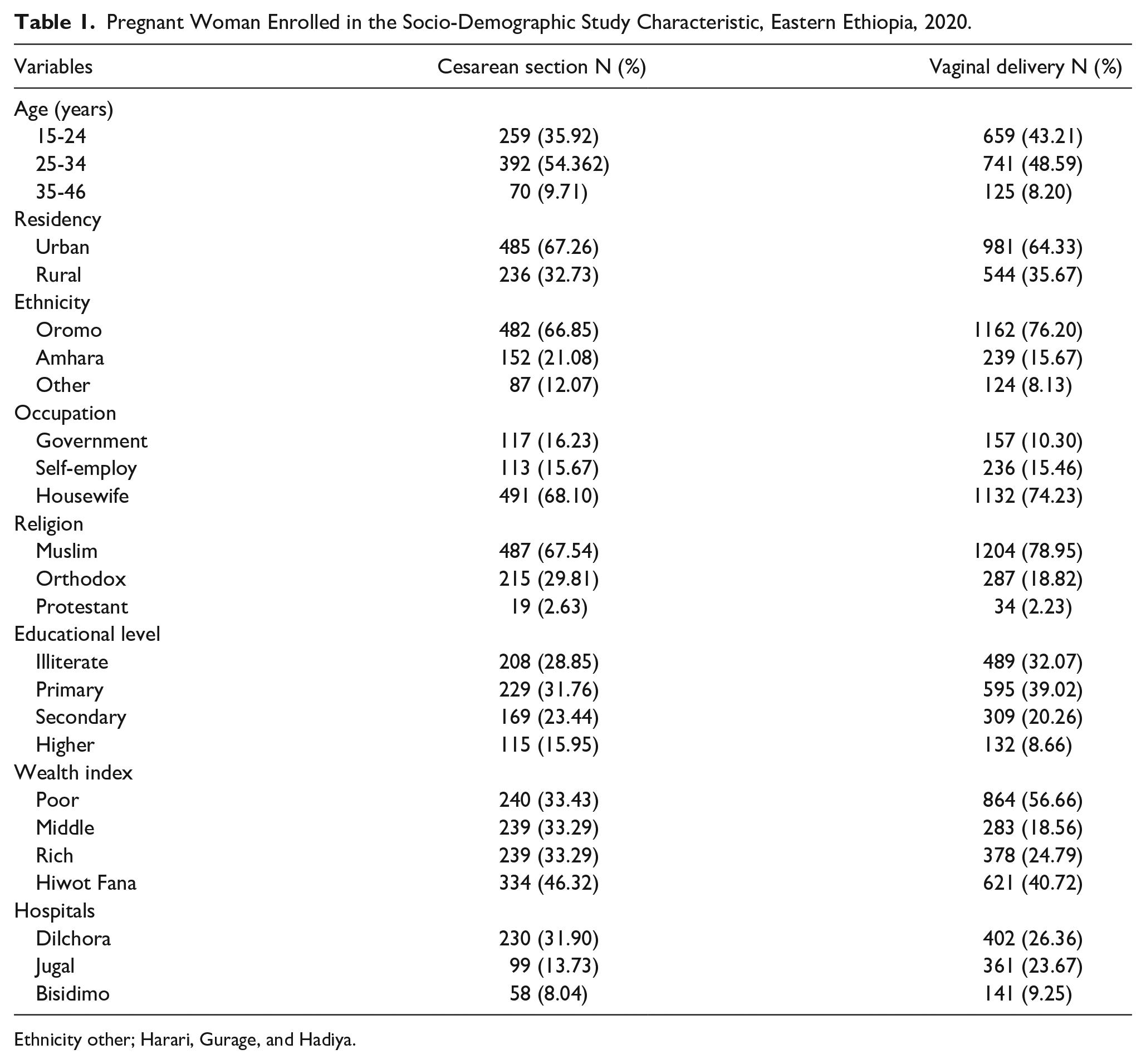
Ethnicity other; Harari, Gurage, and Hadiya.
Sixty-eight neonates were twins (3%); 12.32% of neonates were preterm with the gestational age of 29-36 weeks. 11.72% of neonates were low-birth weight. The mean weight was 3140.78gm with a ± SD of 605.66gm. Among enrolled neonates, 1,561 were born by vaginal delivery, and the rest 753 were delivered by cesarean section (Table 2).
Neonatal Characteristic Enrolled in the Follow-Up, Eastern Ethiopia, 2020.

Magnitude of adverse neonatal outcomes
The overall magnitude of adverse neonatal outcome was 20.97% (95% CI: 19.33-22.71%). Among naturally born babies (virginal birth), 19.41% ( 95% CI: 17.50% 21.47%) experienced adverse neonatal outcomes, whereas, among those born through cesarean section, 24.3% (95% CI: 21.3%, 27.5) experienced the problem. The inclusive finding showed that the most common adverse neonatal outcome was delayed initiation of breastfeeding (39.46%), followed by NICU admission (14.35%)). Birth asphyxia was found at the fourth rank of adverse neonatal outcome (10.72%), with feeding difficulty (10.72%). Among neonates admitted to NICU, 71% needed respiratory support at NICU (Table 3).
Neonatal Outcomes by Mode of Deliveries among Babies Born in the Study Hospitals, Eastern Ethiopia, 2020.

Abbreviations: RD, respiratory distress; MAS, meconium aspiration syndrome; NICU, neonate intensive care unit.
The mean duration of NICU admission for neonates born through CS was 4.05 days with +SD 3.27 days and 4.49 days with a +SD 3.95 days for vaginal delivery. More than one-third of neonates delivered via CS have not initiated breastfeeding within an hour. NICU admission was common among those who delivered by emergency CS(19.23%); besides, low 5 min Apgar score (13.54%) and birth asphyxia (13.37%) were higher in emergency CS, while respiratory distress was common among babies born through elective CS delivery. Birth trauma was higher among babies born naturally (5.13%). Total death was 127(5.49%) until babies were discharged from the hospitals. Among babies born through emergency CS, 7.52% died before discharged from the hospital, while only 5.1% died among babies born naturally (Table 2). Seventy neonates were self-discharged before getting a cure; 47 (67.14) were from vaginal delivery (Table 3).
Socio-Demographic Characteristic of Participants and Adverse Neonatal Outcome
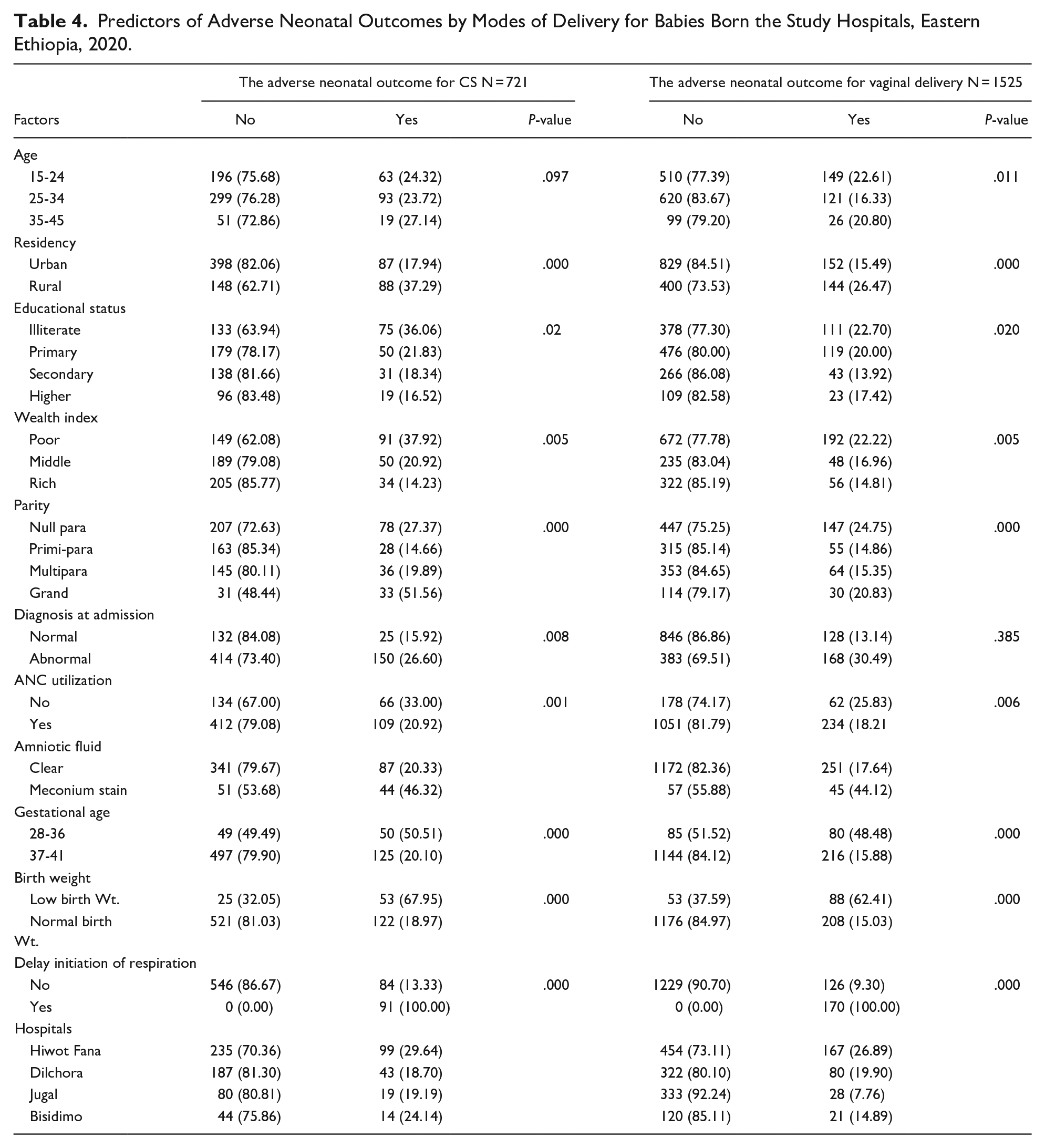
Babies born to rural women through CS had a worse neonatal outcome than babies born naturally to rural women (37.29% vs. 26.47 p-values 0.000). Twenty-seven percent of neonates born from advanced-aged women (35-45 years) through CS developed adverse neonatal outcome, while 20.8% of neonates born naturally from the same age group developed adverse outcome. The adverse outcome was common among illiterate (36%) and poor (38%) women who gave birth through CS. Similarly, it was higher among neonates born from nullipara women via CS than neonates delivered through vagina from similar women (27.37% vs. 24.75%, p-value 0.000). Among 334 neonates born through CS at HFUH, 29.64% of them developed adverse neonatal outcomes, while 18.70% of neonates delivered through CS experienced adverse outcome at Dilchora hospital (Table 4).
Predictors of Adverse Neonatal Outcomes by Modes of Delivery for Babies Born the Study Hospitals, Eastern Ethiopia, 2020.
Obstetric Related Characteristics and Adverse Neonatal Outcomes
The adverse outcome was higher in abnormal labor pregnancy such as APH, pre-eclampsia, obstructed labor, fetal distress, and mal-presentation for naturally born babies (30.49% vs. 26.60% p-value 0.001). Adverse neonatal outcome was more remarkable among women who did not attend ANC and gave birth through CS (33% vs. 25.83% p-value 0.001). Neonates that meconium-stained Amniotic fluid had a statistically higher proportion of adverse outcomes after CS than vaginal delivery (46.32% vs. 44.12%, p-value 0.000). The negative outcome was higher among premature babies (50.51% vs. 48.48%), and low birth weight (68% vs. 62.41%) for neonates born through CS than the natural delivery mode (Table 4).
Predictors for Adverse Neonatal Outcomes
For babies born through CS, birth weight, the presence of meconium in the amniotic fluid, and delayed initiation of respiration were significant predictors, while for naturally born babies, parity, diagnosis of abnormal pregnancy or labor at admission, delayed initiation of respiration, and birth weight were significant predictors. The presence of meconium amniotic fluid increased the risk for neonates delivered through CS (ARR, 1.52 95% CI; 1.04, 2.22). Among naturally born babies, the risk of adverse neonatal outcome was higher for nullipara women (ARR, 1.42 95% CI; 1.02, 1.99, and those delivered from women diagnosed for abnormal labor or pregnancy at admission (ARR, 1.30 95% CI; 1.01, 1.67).
Among babies born in both delivery modes, the risk was significantly higher for those who had delayed initiation of reparation (ARR, 5.28 95%CI; 3.76, 7.42) for CS, and (ARR, 8.38 95%CI; 6.41, 10.97) for naturally born. Similarly, the risk is higher among neonates with low birth weight (ARR, 1.530 95%; 1.08, 2.17) CS born and (ARR, 1.54 95%; 1.11, 2.14) for naturally born (Tables 5 and 6).
Predictors of Adverse Neonatal Outcome Among Babies Born by CS at Selected Public Hospitals in Eastern Ethiopia, 2020.

Predictors of Adverse Neonatal Outcome Among Babies Born Naturally (Vaginal Birth) at Selected Public Hospitals in Eastern Ethiopia, 2020.

Discussion
In this study, the adverse neonatal outcome is defined as the presence of either birth asphyxia, RD, birth trauma, hypothermia, MAS, death, or NICU admission. The overall adverse neonatal outcome was 21% (95% CI: 19.33- 22.71%). This finding is comparable with another study in eastern Ethiopia that showed neonatal mortality at 20% and birth asphyxia at 22.45%. 43 Adverse neonatal outcome was higher among babies born through cesarean section (24.3 %; 95%CI: 21.3%, 27.5) than naturally born babies (19.4%; 95% CI: 17.50%, 21.47%). This is consistent with another study conducted in Northwest Ethiopia whereby the adverse neonatal outcomes were common among CS babies. 44
Among babies born through CS, adverse neonatal outcomes were higher amid delayed breastfeeding initiation within one hour, NICU admission, low 5 min Apgar score, birth asphyxia, and respiratory distress. This is consistent with a study conducted in Canada that showed NICU admission with low 5th minutes Apgar score, and RD were higher among neonates born through CS. 32 Similarly, the result is in agreement with a recent systematic and meta-analysis in Ethiopia, in which low APGAR score, perinatal asphyxia, early neonatal death, and stillbirth were common among CS-born babies. 45
In this study, the presence of meconium-stained amniotic fluid increased the risk of adverse outcome by 52% among CS-born babies. The risk was also increased among naturally born babies, but it was not significantly associated with negative outcomes. This has resulted from 85% of women who underwent CS delivery. The women had grade II and III meconium-stained amniotic fluid compared to 57.6% among the vaginal delivery group with the same grade of meconium-stained amniotic fluid. Such phenomenon indicates a prompt delivery through cesarean section, in thick meconium-stained amniotic liquid for a better outcome.46,47 This finding is consistent with meta-analysis and other studies conducted in Ethiopia that indicated meconium stain amniotic fluid which increases the risk of birth asphyxia and RD.10,12,48-51 This could be due to aspirated meconium-stained amniotic fluid caused by a combination of airway obstruction, surfactant inactivation, and inflammation leading to asphyxia and RD.52,53
The risk of adverse neonatal outcome was 1.42 times higher among nullipara women than multipara who gave birth naturally. This result agrees with studies conducted in Australia and Nepal, which indicated that neonatal mortality was higher in nulliparous.54,55 A research report from the Netherlands also showed that the risk of birth asphyxia doubled in nullipara women than in multiparous. 56 This might be explained by the threat of anemia, CPD, pre-eclampsia, preterm births, vacuum extraction, and low birth weight which are expected in this group of women, leading them to adverse neonatal outcomes. 57
Abnormal labor or pregnancy such as APH, pre-eclampsia, obstructed labor, fetal distress, and mal-presentation increased adverse outcomes risk by 30% among naturally born babies. This result is consistent with Ethiopia’s meta-analysis and other studies that indicated non-cephalic fetal presentation. APH and obstructed labor were significantly associated with birth asphyxia, respiratory distress syndrome, stillbirth, and neonatal mortality.
Delayed initiation of respiration and low birth weight were significant predictors for both modes of delivery. The risk was 5.28 times among CS and 8.38 times among naturally born babies who had delayed initiation of respiration. The finding is supported by a study conducted in Harari region, which indicated that the threat of immediate adverse outcome was significantly associated with respiratory depression. Prolonged or obstructed labor, prematurity, infection, and MAS might have caused delayed initiation of respiration. Prompt resuscitation of initiation is needed for every birth to alleviate consequences such as low Apgar score, birth asphyxia, and respiratory distress.
Among low birth weight babies, the risk of adverse neonatal outcome was increased by 53% for CS-born babies and 54% for naturally born babies. This finding is consistent with meta-analysis and other studies conducted in Ethiopia that indicated low birth weight increased the risk of birth asphyxia and RD.10,12,48-51 The possible reason is that body organs’ maturity is not yet fine-tuned for low-birth-weight babies to respond for eventualities such as low Apgar score, asphyxia, and RD.
This study followed pregnant women from admission to birth and discharge to look into maternal and fetal factors contributing to adverse neonatal outcomes. It had very good attendance and compared naturally born and CS-born babies to attract health professionals’ attention toward averting unnecessary suffering and deaths among newborn babies. The limitation of the study to which we would like readers to pay their attention is its reliance on clinical records mainly based on signs and symptoms, and some outcomes such as asphyxia, MAS, and RD may need additional investigation like chest X-ray and blood PH to diagnose.
Conclusion
Babies born through CS experienced more risk of adverse neonatal outcome as opposed to babies born naturally. Low birth weight and delayed initiation of respiration contributed to the adverse neonatal outcome in both CS and natural delivery modes. Null parity and abnormal labor at admission were predictors of adverse neonatal outcome among babies born naturally, while meconium stain amniotic liquor was a predictor for adverse neonatal outcome among babies born by CS. Quality continuity of maternal care during pregnancy, delivery, and the postpartum period will help in reversing the occurrence of adverse neonatal outcomes to tailor obstetrical actions as needed. Health care providers should be aware of predictors to carry out interventions as early as possible to prevent complications. A continuous obstetrical skill update should be given to health professionals to capacitate them so that they could render delivery services to the standard.
Footnotes
Acknowledgements
We acknowledge Haramaya University, college of health and medical sciences, for funding. Our special gratitude goes to data collectors, participants, and health professionals who work at the obstetric ward and NICU for their unreserved commitment and support.
Authors’ Note
This article is a part of a PhD work.
Author Contributions
All authors participated in data collection, analyzed, and interpreted the data. The corresponding author drafts the manuscript; the rest authors revised the manuscript critically and incorporated intellectual input. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection from Haramaya University as part of higher education research sponsorship.
Availability of Data and Material
All the data of this study are available from the corresponding author upon request