
Abstract
Objective:
The aim of this was to assess cause of neonatal admission and factors associated with treatment outcome in intensive care unit in Mekelle city, public hospitals, Ethiopia.
Methods:
A hospital-based cross-sectional study was employed among study participants from November 2021 to June 2022. Data were collected using structured data extraction checklist. SPSS V-20 was used for data analyzing. Binary logistic regression model was used with a 95% confidence interval and P-values <.05.
Result:
Leading cause of neonatal admission were 83 (24.9%) sepsis followed by 59 (17.7%) respiratory distress syndrome (RDS), 31 (9.3%) meconium aspiration syndrome (MAS), and 31 (9.3%) perinatal asphyxia (PNA). Overall neonatal mortality was 38 (11.37%). Cesarean section (C/S; AOR: 2.9; 95% CI: 1.82, 4.68), breastfeeding non-initiation within 1 hour (AOR: 2.6; 95% CI: 1.09, 4.16), and neonatal resuscitation (AOR: 2.16; 95% CI: 1.70, 4.54) were factors associated with treatment outcome.
Conclusion:
The leading causes of neonatal admissions were sepsis, RDS, MAS, and PNA. Cesarean section (C/S) delivery, breastfeeding non-initiation within 1 hour and resuscitated neonate were factors associated with treatment outcome.
Introduction
Neonatal period is the most vulnerable period for childhood survival, especially in developing country. 1 A newborn admitted to a neonatal intensive care unit (NICU) faces an immediate danger of morbidity and death, as well as an emotional strain on their family and a significant financial load on the health care system. 2 Every nation has distinct neonatal causes for admitting to intensive care unit. Birth defects and congenital malformations are among the non-preventable causes of newborn hospitalization in most developed nations, but the majority of neonatal admissions in developing nations could have been prevented with the use of various strategies.3,4 Sociocultural factors and behavioral variables including education levels, societal difficulties, conventional views, and the parents’ prenatal gender-based inclinations are among the factors that related with cause of neonatal hospitalizations and mortality.2 -4
Approximately 2.3 million babies died globally in 2022, with 6300 deaths occurring every day during the first month of life on average. 1 Despite a decline in the worldwide newborn mortality rate (NMR), notable differences still exist between nations and regions. The world’s greatest neonatal mortality rate was found in Sub-Saharan Africa, with 27 deaths per 1000 live births; Central and southern Asia followed with 21 fatalities per 1000 live births. 2 In accordance with the 2019, Ethiopian mini demographic surveys in Ethiopia the neonatal and infant mortality were 30 and 43 for every 1000 live births respectively. The rate of neonatal mortality significantly reduced in the last 2 decades; however the change in neonatal mortality is not as dramatic as fall in the under-5 children mortality. 5
Globally the leading causes of neonatal mortality were premature birth, neonatal birth complications, birth asphyxia, birth trauma, neonatal infections and congenital anomalies remain the leading causes of neonatal deaths.1 -3 Infections, neonatal related mortality, and malnutrition were accounts for over two-thirds of Ethiopia’s child deaths, while prematurity, low birth weight, infections, and birth trauma account for nearly 80% of these neonatal deaths.5,6 A single study reported that the common causes of neonatal admission were perinatal asphyxia, hypoglycaemia, and hypothermia. 7 Another similar study reveals that the common causes of morbidities were prematurity, hyaline membrane disease, hemorrhagic disease, neonatal sepsis, perinatal asphyxia MAS, and neonatal seizure. 8
The Sustainable Development Goals (SDGs) rely on lowering the mortality rate of newborns to less than 12 deaths per 1000 live births by 2030. 9 Children are still dying of disease which could have been prevented and/or treated easily with low cost and effective interventions. 10 By 2025, a high coverage of prenatal, intrapartum, and postnatal quality care globally will avert 71% of neonatal deaths, saving 1.90 million newborns annually, according to the Every Newborn Action Plan (ENAP) 2014. 11 However, there are currently no estimates of cost impact of newborn death at the national level (in Ethiopia). Similar to all fatalities, neonatal mortality can significantly damage the impacted family’s emotional state. 12
World Health Organization (WHO) advises enhancing maternity care practices and essential newborn care (ENC) practices for reducing neonatal and infant morbidity and mortality. The Ethiopian government has implemented evidence-based treatments throughout a continuum of care at several levels, including the family, community, and facility levels, as well as focused on reducing newborn cause hospital admission and death through integrated health service packages. 13
Despite the fact that some research has been conducted in Ethiopia related to neonatal mortality rate, limited number of studies has been conducted on the causes of neonatal admission and factors associated with treatment outcome of neonates admitted to intensive care units. So the aim of this study is to assess cause of neonatal admission, death and factors associated with treatment outcome of neonates admitted to intensive care unit in Mekelle city, public hospitals, Northern Ethiopia.
Methodology
Study Setting, Period and Study Design
Hospital based cross-sectional study was conducted among neonates admitted to intensive care unit in Mekelle city, public hospitals, Ethiopia. As of 2024, the population of Mekelle city, Tigray region, Ethiopia’s is estimated to be around 611 574 residents. Mekelle has 3 governmental general hospitals, 1 specialized hospital and 9 health centers. Adult, pediatric, and neonatal intensive care units are available in all of the selected hospitals—ACSH, Mekelle General Hospital, and Quiha General Hospital, offer services with distinct staff and rooms. There are general practitioners, Interns, diploma nurses, BSc nurses, specialty physicians, and others. Nevertheless, in 1 study area (Quiha General Hospital) does not have any Interns or specialized neonatologists, but it has general practitioner (GP). The study was conducted from November 2021 to June 2022.
Source of Population and Study Population
All neonates admitted in Mekelle city public hospitals of the intensive care unit were source of population. All systematically selected neonates medical charts admitted to intensive care unit of during study period were study population.
Inclusion Criteria and Exclusion Criteria
As indicated in the neonate medical chart, age less than or equal to 28 days of neonates admitted to intensive care unit from November 2021 to June 2022 were included in the study. As indicated in the neonate’s medical chart, neonates who were referred from other study site (neonates who came by referral from other selected hospitals for study site) and admitted to intensive care unit were excluded from the study. The purpose of this exclusion for neonate’s chart was to avoid double account of participant. All incomplete neonate medical charts were excluded.
Sample Size Determination and Sampling Procedure
Single population proportion formula was to calculate the required sample size by considering the following statistical assumptions: P = proportion of neonatal mortality rate among neonate admitted in NICU, 20.2%, 14 (Z α/2 = Z score of 95% CI, d = Margin of error (5%).

=247, then after adding 5% non-response rate and adding design effect, so the final sample size was 259 × 1.3, n = 336.
Design effect was used because in this study we have 2 stages; stage 1 was selection of 3 hospitals from the total 5 public hospitals using simple random sampling lottery method, and stage 2 was selection of study participants from hospitals using systematic random sampling approach (Figure 1). And design effect was considered to account for increased variability introduced by selected hospitals, in which the setup of selected hospitals are different in several features such as number of patient follow, availability of senior neonatologist and equipment used for neonatal treatment, resuscitations and management.
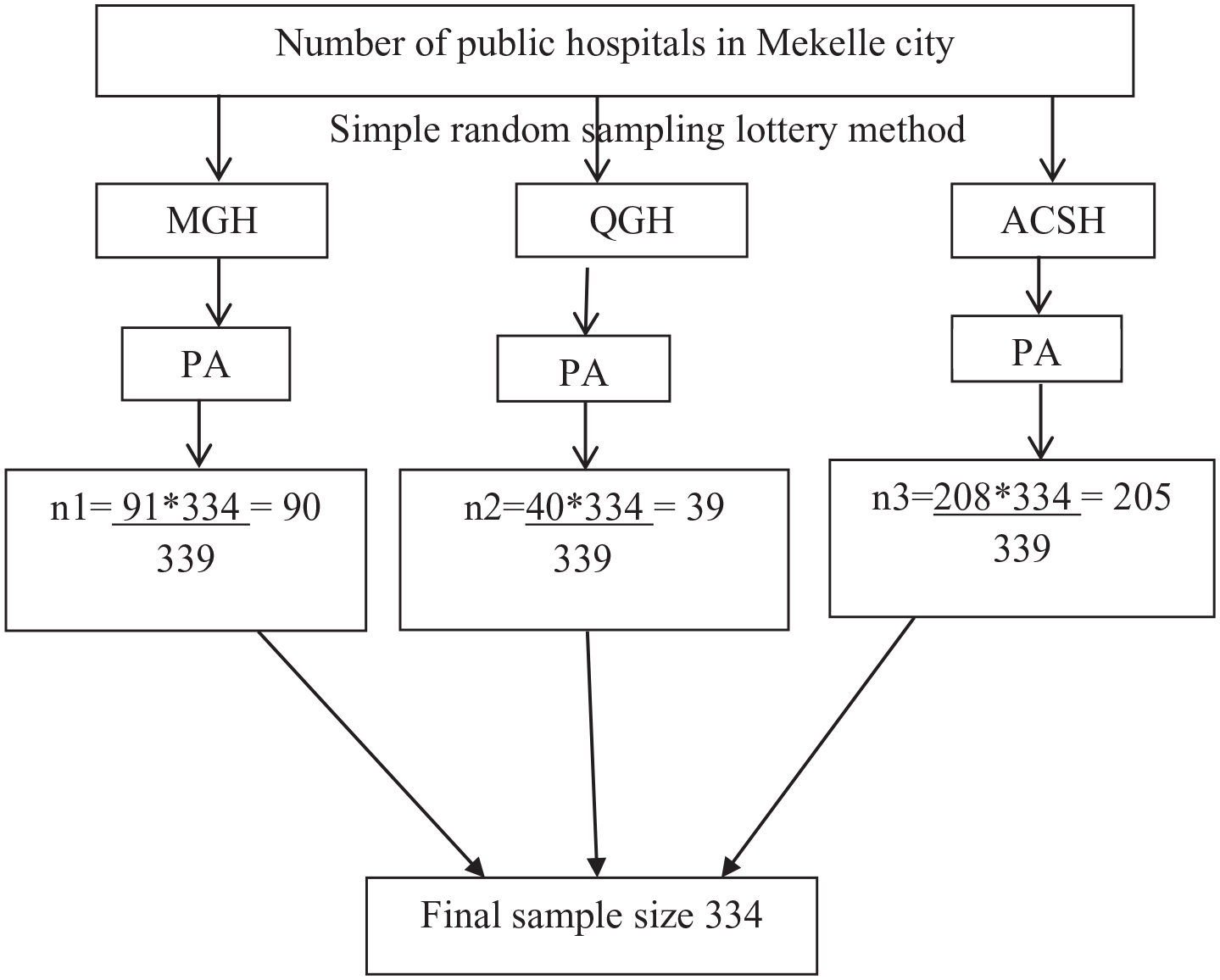
Flow diagram of sampling procedure to assess cause of neonatal admission and factors associated with treatment outcome in NICU in Mekelle city, public hospitals, Ethiopia, 2022.
Neonatal intensive care units are available in 5 government hospitals in Mekelle, City. From these hospitals using simple random sampling lottery method 3 site were selected. The sample size was distributed proportionately to each of the chosen hospitals according to the total number of NICU admissions during the preceding year. The charts of study participants were chosen via systematic random selection from each of the hospitals that were chosen (K = 678/334 = 2nd). Then a participants charts were selected every second intervals of charts participants from registry after 1 chart was chosen using simple random sampling. Hence included were 39 from Quiha General Hospital, 205 from ACSH, and 90 from Mekelle General Hospital.
Figure 1 shows the schematic presentation of the sampling procedure and sampling method to select study participants from hospitals in Mekelle city.
Variables
Dependent Variable
Treatment outcome (died or survived).
Independent Variables
Mother age, neonatal age, sex and residence, ANC utilization, mode of delivery, and delivery complication at birth. First and fifth minute APGAR score, Gestational age, neonate resuscitated, birth weight, initiation of BF, RDS, sepsis, PNA hypoglycaemia, and prematurity.
Data Collection Tools and Procedure
Structured questionnaire and extraction checklist used for data collection, adapted from “verbal autopsy questionnaires” 15 and was also modified from different related studies.14,16 The questionnaire was first created in English and then translated into Tigrigna, the native language. Data extraction checklists were used by trained midwives to extract data from medical record charts. Data collectors were 5 midwives and 2 MSc holder supervisors who work in non-study locations and are fluent in the local language. These data collectors were under the supervision of the principal investigator and with assistance from the head nurse during the process. The checklist includes elements relating to the mother’s socio-demographic profile, obstetric and maternal variables, and newborn and critical care unit features.
During data collection process, data collectors examine the patient charts for recording the important variables like cause of neonatal admission (diagnosis at admission), cause of death and medical death certificate. In the patient medical chart causes of neonatal admission was diagnosed and confirmed by physicians (interns or general practitioners) signature which was written and signed in the patient chart. And the medical death certificate and cause of deaths were confirmed by the signature of physicians in the patient’s chart. In the data collection site, the 2 hospitals have interns and neonatologist; however in 1 hospital only have general practitioners (GP). So, in 2 hospitals the neonatal diagnosis at admission was made by interns, and diagnosis cause of death was made and confirmed by neonatologist, but in 1 hospital all diagnosis was made by general practitioner (GP).
In this study the questionnaires/scales used were pilot-tested before actual data collection time.
Data Quality Control
The creation of appropriate data extraction technique ensured the quality of the data. Before the study began, a pretest was conducted using a structured checklist on 5% (17 neonates chart) of the total sample size, to ensure that the variables were consistent and clear in the patient’s medical chart. Supervisors and data collectors received a 1-day instruction on the goals of the study, how to fill out a structured questionnaire, how to extract the necessary information, and how to maintain the confidentiality of the information. The supervisors were monitoring data collection process. Data was assessed for completeness, and any issues related with missed data were addressed appropriately.
Data Processing and Analysis
Epi-data version 4.4.2.1 was used for data were entering, codding and editing and were exported to SPSS version 20 for cleaning and analysis. Descriptive statistics were used to analyzes the frequencies, percentages, rates, and to calculate the mean and standard deviation after checking the distribution of the data.
The assumptions of the binary logistic regression model were verified using Hosmer-Lemeshow goodness-of-fit test and variables with a P-value >.05 were deemed to satisfy the assumption. Bivariate logistic regression analysis was performed for every explanatory variable. Consequently, the variables with a 95% confidence interval and a P-value ≤.05 in the bivariate analysis were fitted to the multivariable logistic regression model. In the multivariable logistic regression model P-value ≤.05 was considered as statistical significance. The study employed odds ratios (OR) featuring a 95% confidence interval and P-values ≤.05 to assess the degree of correlation and determine the statistical significance between the independent and dependent variables. The presence of confounding factors was assessed and addressed.
Operational Definition
Cause of Neonatal Admission
In this study it is to mean that any medical or non-medical neonatal diagnosis at admission to the intensive care unit. The diagnosis was made by physicians (Interns and general practitioner), as confirmed with signature of the physicians in the patient medical chart. 17
Cause of Neonatal Death
In this study it is to mean that any medical or non-medical diagnosis, as “cause of death” that indicated in the patient charts medical death certificate. The diagnosis cause of neonatal death was made and signed by physicians (neonatologists and general practitioner) as indicated in the medical death certificate of the patient medical chart. 17
Treatment Outcome
Treatment outcome is the final treatment outcome of NICU admitted neonates; it was categorized as either dead or survived.
Survived
Treatment outcome was categorized as survived, as indicated in the patient medical charts, those neonates discharged home, and transferred to other health institution and others rather than death.
Dead
In this study this treatment outcome was considered for death of neonate, which was confirmed on the patients chart with medical death certificate signed by physicians.
Neonatal Resuscitation
In this study, the neonatal resuscitation status was recorded and available in the patient medical charts.
Ethical Approval and Informed Consent
Ethical approval was granted from Mekelle University, College of Health Sciences, Institutional Review Board (IRB) of with the reference #of ERC 1523/2020. Subsequent permission was also obtained from hospitals. Patient informed consent was not required for retrospective data, since the hospital gave the permission. All the information was used exclusively for study purposes. All the procedure was carried out in conformity with the relevant standards and regulations as well as the Helsinki Declaration.
Results
Socio-Demographic Characteristics of Mothers and Neonates
In this study, 336 neonatal charts were selected, but 2 charts were incomplete, so a total of 334 neonate’s charts were used in final sample analysis (Table 1).
The Socio-Demographic Participants for Assessment of Cause of Neonatal Admission and Death in Intensive Care Unit of Public Hospitals, Mekelle City, Tigray, Ethiopia, 2022 (n = 334).

Maternal and Obstetric Related Characteristics
According to this study, majority 212 (63.5%) of neonate were born in hospital, and 91 (27.2%) in health center/clinic. Table 2 describes the maternal and obstetrics characteristics of participants.
Maternal and Obstetric Related Characteristics of Neonates Admitted to Intensive Care Unit in Mekelle City, Selected Public Hospitals, Tigray, Ethiopia, 2022 (n = 334).

Abbreviations: APH, antepartum hemorrhage; C/S, cesarean section; PPH, postpartum hemorrhage; PIH, pregnancy induced hypertension; PROM, premature rupture of membrane; NRFHRP, non-reassure fetal heart rate pattern, Other*indicate that precipitated labor, post term, obstructed labor, Rh incompatible, Intrauterine growth restriction (IUGR), polyhyramious and oligohydramious etc; SVD, spontaneous vaginal delivery.
Figure 2 shows the maternal complications that experienced during pregnancy and delivery time.

Pregnancy and delivery complications of mothers of neonates admitted to intensive care unit in Mekelle city selected public hospitals, Tigray, Ethiopia, 2022 (n = 334).
Neonatal and Health Service Related Characteristics
Among neonates admitted to NICU 203 (62.5%) of birth weight were ≥2500 g, birth weight was normally distributed so the mean birth weight were 2682 g and standard deviations (SD ± 782; Table 3).
Neonatal and Service Related Characteristics for Assessment of Cause of Neonatal Admission and Death in Intensive Care Unit of Public Hospitals, Tigray, Ethiopia, 2022 (n = 334).

Abbreviations: APGAR, appearance, pulse, grimace, activity, and respiration; NICU, neonatal intensive care unit.
Figure 3 describes the type of treatment the neonates received in intensive care unit.
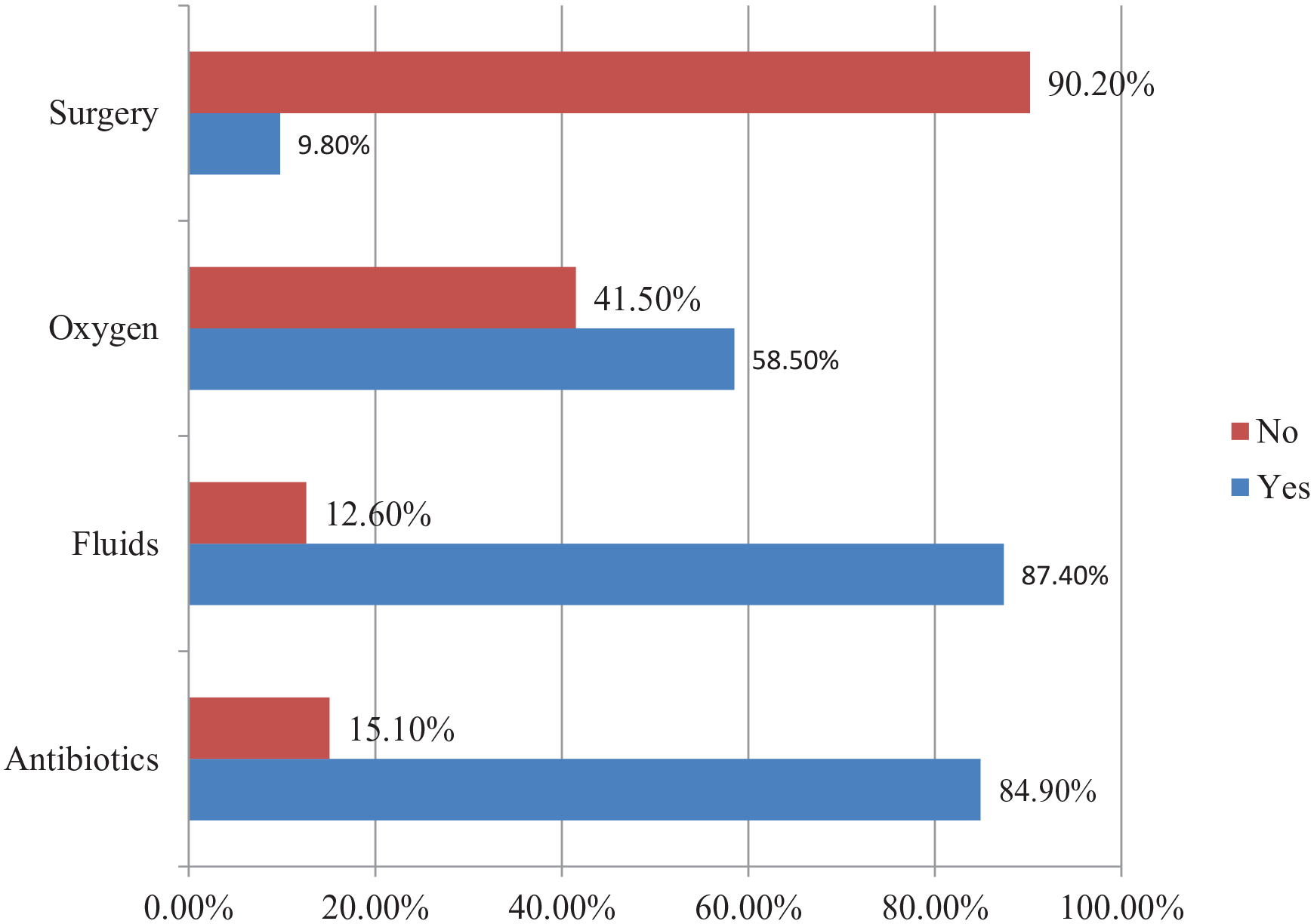
Type of treatment received among neonates admitted to intensive care unit in Mekelle city, selected public hospitals, Tigray, Ethiopia, 2022 (n = 334).
Cause of Neonatal Admission and Neonatal Death
The leading cause of neonatal admission (diagnosis at admission) was described below in Figure 4.

Leading cause of admission for neonates admitted to intensive care unit in Mekelle city selected public hospitals, Tigray, Ethiopia, 2022 (n = 334).
Figure 5 described the leading cause of neonatal death.

Leading cause of neonatal death in intensive care unit in Mekelle city selected public hospitals, Tigray, Ethiopia, 2022 (n = 334).
Factors Associated with Treatment Outcomes
Binary logistic regression model was used to analysis factors associated with treatment outcome of neonate admitted to NICU. In the bivariate analysis several variables were statistically significant at (P ≤ .05). However, on the multivariable logistic regression analysis only C/S (cesarean section) mode of delivery, breastfeeding initiation within 1 hour and neonate resuscitation status were factors associated treatment outcome at P-value ≤.05.
This study finding reveals that neonates delivered with C/S were 2.9 times more likely to die as compared with neonates born via SVD (AOR: 2.9; 95% CI: 1.82, 4.68). Current study indicated that neonates whom did not initiated breastfeeding within 1 hour of delivery were 2.6 times more likely to die as compared to those of neonates which did initiated breast feeding within 1 hour of birth (AOR: 2.6; 95% CI: 1.09, 4.16). Those neonates who had history of neonatal resuscitation were 2.16 times more likely to die as compared to those neonates who had no history of resuscitation (AOR: 2.16; 95%CI: 1.70, 4.54; Table 4).
Bivariate and Multivariable Regression Analysis for Assessment of Associated Factors with Treatment Outcome in Intensive Care Unit of Public Hospitals, Tigray, Ethiopia, 2022 (n = 334).

The effect of confounding factors was addressed by doing different methods during or after doing analysis.
Abbreviations: ANC, antenatal care; APGAR, appearance, pulse, grimace, activity and respiration; C/S, cesarean section; SVD, spontaneous vaginal delivery.
Significant at (P-value ≤.05).
Discussion
This study shows that the leading cause of neonatal admissions (diagnosis at admission) were sepsis, RDS, MAS, PNA, jaundice, and hypothermia, and the leading cause of mortality were PNA, sepsis, shock, prematurity, RDS, and MAS. The overall neonatal mortality was found 38 (11.37%) with (95% CI: 8.53, 15.81) neonates were died in NICU. Multivariable analysis finding reveals that mode of delivery with C/S, breastfeeding non initiation within 1 hour and neonatal resuscitation were factors associated with neonatal treatment outcome.
This study indicated that, the leading cause of neonatal admission (diagnosis at admission) were sepsis, RDS, MAS, PNA, jaundice, and hypothermia. This finding is consistent with a study conducted in different parts of the country in Dire Dawa, 7 Gondar, 8 Eastern Ethiopia, 18 Addis Abeba, 19 and Adama 20 and in other countries in Uganda, 17 Israel, 3 and Jordan. 21 However this finding is inconsistent with a study conducted in Gondar, 22 which was hypothermia, sepsis, and prematurity, and in Enugu State University 23 which was PNA, low birth weight, sepsis, and jaundice, Saudi Arabia, 24 which were RDS, hypoglycaemia, and jaundice were the main reason for neonatal admission.
Based on finding of this study, the leading causes of neonatal death were PNA, sepsis, prematurity and RDS. This finding is concurrent with a study conducted in Adama, 20 Gamo Gofa, 25 Sidama, 26 Jima, 27 and Nigeria, 28 but the study done in Addis abeba, 19 which was RDS and asphyxia were the leading cause of neonatal mortality. This difference might be due the difference in the study period as there were changes in treatment modality where access of health care service was increased, the health seeking and utilization behavior of the community and accessibility of trained health care providers are comparatively increased. And this could be associated with prematurity and low birth weight in which the NICU setup may not able to manage these risk factors during this period.
The result of multivariable analysis reveals that neonates delivered with C/S were 2.9 times more likely to die as compared with neonates born via SVD. This finding is in line with a study conducted in pastoral region Ethiopia, 29 Southern Ethiopia, 30 Tanzania, 31 Australia, 32 however a study done in Gondar 8 indicated that home SVD delivery were factors associated with poor neonatal outcome. Cesarean section (C/S) delivery is life-saving for the mother and newborns when it is medically indicated, however it increase the risk of newborn death due to numerous factors, particularly when carried out under unfavorable circumstances or in absence of a medical need. Other study 33 reported that compared to vaginal deliveries, cesarean section neonates are exposed to various microbial natural environments. This raises the risk of infections, such as sepsis, which can be fatal if left untreated and result in neonatal death. 33 This support our data finding that, sepsis is the second leading cause of neonatal death which accounts 21.1% of total death, the sepsis might be related with C/S delivery.
Due to inadequate lung development, babies born via C/S, particularly those delivered before 37 weeks of gestational age are more susceptible to RDS, which in turn RDS cause neonatal death 33 ; this report is similar with our finding that RDS is among the leading causes of neonatal mortality and accounts 18.4% of a total neonatal mortality. This presence of sepsis and RDS might be associated with C/S delivery. 33 Rarely, newborns born by cesarean section may get scratches or abrasions from the surgical tools used during the operation, which might cause serious neonatal complications. 34
Current study indicated that neonates whom did not initiated breastfeeding within 1 hour of delivery were 2.6 times more likely to die as compared to those of neonates which did not initiated breast feeding within 1 hour of birth. This study is consistent with a study done in Eastern Ethiopia, 18 Southern Ethiopia, 30 and Mogadishu Somalia. 35 For a number of reasons, breastfeeding begins within an hour after delivery, dramatically lowers the risk of newborn mortality. Firstly, it facilitates the transfer of colostrum, a rich source of nutrition and antibodies vital to the developing baby’s immune system. Early feeding promotes emotional and physical stability for both the mother and the child by strengthening the mother-infant attachment. Furthermore, nursing increases oxytocin release, which helps with uterine contraction and lowers the mother’s risk of postpartum hemorrhage. In addition to promoting improved nursing techniques, early breastfeeding helps shield neonates from diseases including hypoglycemia and hypothermia. All things considered, these elements support better health outcomes and decreased death rates.
The finding of this study reveals that neonates who had resuscitated were 2.16 times more likely to die as compared to those neonates who had not resuscitated. This result is supported with the previous study done in Southern Ethiopia, 30 Uganda, 17 and Mogadishu Somalia. 35 Although they are frequently spared from immediate danger, resuscitated newborns are nevertheless susceptible to a number of hazards that could result in death. Prematurity, congenital defects, or birth asphyxia are some of the reasons for resuscitation that may put the neonate at risk for complications that could compromise their survival. Significant hypoxia or ischemia prior to resuscitation may cause brain damage in a newborn, increasing the chance of long-term problems and fatality. Infants who have been resuscitated may be more vulnerable to infections because of their weakened immune systems, particularly if invasive procedures were used during resuscitation. Resuscitation attempts that are insufficient or delayed may result in worse outcomes and a higher chance of death.
Limitations of the study are related to the cross-sectional nature of the study, and the use of medical review charts, which may leads to some incompleteness of the data.
Conclusion
In this study we found that the leading causes of neonatal admissions (diagnosis at admission) were sepsis, RDS, MAS, and PNA. And the leading causes of neonatal death were PNA, sepsis, shock, prematurity, RDS, and MAS. Multivariate regression analysis indicated that mode of delivery with Cesarean section (C/S), breastfeeding non initiation within 1 hour of delivery and resuscitated neonate were factors associated with neonatal treatment outcome.
Healthcare professional working in delivery room and intensive care unit should give more attention for neonates delivered via C/S, neonates who had not initiated breastfeeding within 1 hour of delivery and resuscitated neonate. Neonatal nurses in NICU should give special emphasis and close follow up for neonates diagnosed with sepsis, PNA, RDS, and MAS because these are the leading cause of neonatal mortality. Future researchers further community based study should be conducted.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251324304 – Supplemental material for Cause of Neonatal Admissions and Factors Associated with Treatment Outcome in Intensive Care Unit Mekelle City Public Hospitals, Ethiopia: Hospital Based Cross-Sectional Study
Supplemental material, sj-docx-1-gph-10.1177_30502225251324304 for Cause of Neonatal Admissions and Factors Associated with Treatment Outcome in Intensive Care Unit Mekelle City Public Hospitals, Ethiopia: Hospital Based Cross-Sectional Study by Gebrhud Berihu Haile and Berhe Gebrehiwot Tewele in Sage Open Pediatrics
Footnotes
Acknowledgements
We are greatly indebted to Mekelle University, College of Health Sciences for giving us financial and administrative support. We thank to Tigray Region Health Bureau, data collectors, neonatal intensive care unit department heads for their invaluable contribution to the realization of this study.
Statements and Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.