
Abstract
Background. In the clinical management of diabetes, fixing metabolic variables is insufficient, and thus, health-related quality of life assessment is becoming an important indicator of the outcome of the treatment and detector of a problem in children and adolescents with chronic disease. Therefore the main aim of this study was to assess the Quality of life of children with type 1 diabetes in Addis Ababa, Ethiopia. Methods. A cross-sectional study design was included 229 study participants with type 1 diabetics aged between 8 and 18 years in Addis Ababa governmental hospitals. Samples were selected by a systematic sampling method and interviewed face to face. Health-related quality of life was determined by the pediatric quality of life inventory. Multivariable linear regression was done and a significant association was declared at P < .05. Result. The total mean score of health-related quality of life was 78.8 ± 15.6 reported by child and 61 ± 7.9 reported by parents. In this study well-controlled glycemic level (β = 11.8, 95%CI: 8.7, 14.9), health education on diabetes (β = 5.92, 95%CI: 2.9, 8.9) and frequency of hospital admission (β = −2.6, 95%CI: −4.8, −0.42) were clinically predicting factors of health-related quality of life. Conclusion. This study found that there was a somewhat reduction in school and emotional functions of health-related quality of life. The glycemic level, health education of diabetes and frequency of hospital admission was clinically significant factors of health-related quality of life. This study will recommend to the health professional to sustain a health education program on diabetes.
Background
Diabetes is becoming one of the health-related emergencies in the 21st century; type 1 diabetes (T1D) is defined as an endocrine disease characterized by a rising in blood glucose levels resulted from the autoimmune distraction of insulin-producing beta cells in the islets of the pancreas gland and requiring a lifelong insulin replacement therapy. 1
Research has confirmed that living with T1DM has numerous challenges for children, adolescents, and parents related to its management such as intensive therapeutic insulin regimes, a restrictive lifestyle, careful eating habits, and daily monitoring of blood glucose levels to avoid various complications.2,3
Diabetes has a psychological impact on children and adolescents. They have an increased risk of depression, worries, and an eating disorder.4,5 Children with chronic illness have experienced a greater frequency of peer rejection and asocial behavior compared with healthy peers. It has a potential impact on their future development and mental health outcomes. 6
Thus all hurt the daily life of children and adolescents, and it has an impact on their health-related quality of life (HrQoL). 7 Previous studies have confirmed that HrQoL is an important indicator of the outcome of treatments and is also used to describe the impact of the diseases on the child.8,9 Even though there is no universal definition regarding HrQoL, it is used to describe the impact of the disease in terms of physical functioning, psychological functioning (emotional and cognitive), level of independence, personal beliefs, and social function. 10
Traditionally, the management of T1DM has been dedicated to achieving a target glycemic level to prevent the complications of the disease. However in current Medicine, health is not merely the absence of the clinical parameters or markers of disease but it is holistic to all the domains of health, and it recognizes the importance of treating all dimensions of patient health. 11 As such, previous studies have recommended a regular measurement of HrQoL in children and adolescents with diabetes.8,9
Generally, evaluation of the HrQoL and addressing its determinant factors should have been 1 part of diabetes management for a better outcome of the disease in addition to medical management. Despite this, until recently as per the knowledge of the investigator, studies on the quality of life of children and adolescents with diabetes have not been conducted in the local area and only a few studies have been done on adults. Most of the studies had done in other foreign countries. Since there is a great difference in the health care delivery system, religion, culture, and family dynamics in different societies, a study is needed on quality of life in different communities to address different determinant factors.
Therefore, this study aimed to assess the health-related Quality of life and its associated factors of diabetes among children and adolescents in Addis Ababa governmental hospitals.
Methods
Study Design and Setting
The institutional-based cross-sectional study design was used to conduct a study in Tikur Anbesa Specialized Hospital, Yekakit 12, and Zewuditu hospitals at Addis Ababa, these are government hospitals that provided diabetics services to the population. The study was conducted from March 1 to May 30, 2018. A total of 470 diabetics patients aged between 8 and 18 years had been identified in the 3 hospitals. The total population size of the town was estimated to be 3 433 999 of which 1 624 999 were males and 1 809 000 were female. 12
Source and Study Population
Source populations were all children and adolescents with their parents/caregivers who had diabetics follow up in Addis Ababa governmental hospitals. And the study population were all systematically selected children and adolescents with their parents/caregivers who had been attending the endocrine clinic. A child aged between 8 and 18 years who had been diagnosed with diabetes for at least 3 months was included in the study.
Variables
Dependent variable
Quality of life in children and adolescents with diabetes
Independent Variables
Sociodemographic variable
Age of children/adolescent
Gender
Maternal education
Father education
Socioeconomic status of a family
Number of children in a family
Clinically related variable
Metabolic control
Duration of illness
Drug regimen/injection per day
Number of hospital admission
Family history of diabetes
Operational Definition
Well-controlled FBS level:
For age group (8-12): 90 to 180 mg/dl
For age group (13-18 years) :90 to 130 mg/dl
Poor glycemic control:
For age group (8-12) :<90 or >180 mg/dl
For age group (13-18 years) <90 or >130 mg/dl
Age group from 8 to 12 years considered as children.
Age group from 13-18 years considered adolescents.
Sample Size Calculation and Sampling Procedure
The sample size was calculated by the Single population proportion formula with the following assumption: about 50% of the population proportion had good quality of life, 95% confidence interval, 5% margin of error (absolute level of precision) which gives 384. The sample size was adjusted to 213 by correction formula. About 10% of none respondent’s rate was considered and the final sample size becomes 234.
After the proportional allocation of the sample size in each hospital, the study participants were selected by a systematic sampling method. The sampling interval “K” was calculated. So to calculate, The Source population was 470. Then K = N/n, 470/234 = 2. The first eligible study subject was selected randomly. Then every two-interval of children and adolescents with diabetes respective to their parents/caregivers who had been visiting the Endocrinology clinic during the data collection period were selected.
Data Collection Tool and Procedure
Data were collected by pretested, structured, interviewer-administered questionnaires. The questionnaires had two-part;
(I) socio-demographic question and medical-related question which was developed from different literature
(II) The pediatric Quality of Life Inventory 4.0 Generic Core Scale (PedsQL4.0 GCS) was used to measure HrQoL. It was adopted from mapi-trust. 14 It was available for the age group (5-7, 8-12, 13-18, and > 19 years). The 2 age-appropriate instruments respective to the child age (8-12 and 13-18) were used in this study. It has a 23-item, multidimensional quality-of-life instrument. Items in each 4 sub Scales were Physical functioning (8 items), Emotional Functioning, Social Functioning, and School Functioning (5items for each). It was reported with both children and parents. They had been asked to rate the problem on 5 Likert scales from 0 to 4. (0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem, and 4 = almost always a problem) in the last 1 month. Then each items were reversely scored and linearly transformed to a 0-100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0), so that higher scores indicate better HrQOL. Scale scores were computed as the sum of the Items divided by the number of items answered. If > 50% of the items in the scale are missing, the scale score is not computed.
Both instruments were prepared in English and translated to Amharic. It was translated back to English by an independent translator to maintain consistency of the tool.
Data collection was started by obtaining permission from Tikur Anbesa Specialized Hospital, Yekakit 12, and Zewuditu hospitals. The purpose of the study was explained and confidentiality was assured then, children and adolescents with their respective parents were interviewed separately. Six diplomas data collectors and 2 BSC supervisors have participated.
Data Quality Control
Data quality was ensured during collection, coding, entry, and analysis. The internal consistency reliability test for PedsQL™ 4.0 GCS was done, Cronbach’s Alpha (α = .86). A pre-test was done on 5% at Saint Paulo’s hospital which was not included in the study. The training was given to data collectors and supervisors. Regular Supervision of data collectors was done. Before data entry, the filled questioner was checked by data collectors, supervisors, and Principal investigators for completeness and clarity daily. Incomplete data were discarded.
Data Analysis
Data were entered by Epi data version 4.20 and analyzed by SPSS version 21. Data were summarized by Frequencies, Percentage, mean and standard deviation and presented by a table. A paired t-test was done to compare children’s, adolescent’s self-report and parent proxy reports. One sample independent t-test and one-way ANOVA were done to compare the mean score of children for PedsQL™ 4.0 GCS according to sociodemographic and clinical variables. Multivariable linear regression analysis was adjusted for determinant factors. Finally, both the mean difference in PedsQL™ 4.0 GCS score and statistically associated factors were declared at P < .05.
Result
Socio-Demographic Characteristics
A total of 229 participants was included in the study give a response rate of 97%, from this about 127 (55.5%) of them were males and about 102 (44.5%) of them were females. One-fourth of 58 (25.3%) of them were a member of a family having more than 4 children. The mean age of children and adolescents was 12 ± 3. About 110 (48%) of children’s mothers and 143 (62.4%) children’s fathers had secondary and above educational levels (Table 1)
Socio-Demographic Characteristics of Children and Adolescent with Diabetes, Addis Ababa, 2018.

Clinical characteristics
The mean age for diabetes onset was 7 ± 3 (mean ± Standard deviation) years and the median duration of participants with diabetes was 5 years. All participants were used only injectable insulin. They had 185 ± 81 mean levels of fasting blood sugar (FBS). About 55(24%) children and adolescents had a history of admission in the last 6 months and 30 (13.1%) of children and adolescents had a family history of diabetes (Table 2).
Clinical Characteristics of Children and Adolescent with Diabetes, Addis Ababa, 2018.

Comparison of Child- Self and Parent Proxy Report of PedsQL™ 4.0 GCS
The paired sample t-test was revealed that there was a statistically significant difference in child self-report and parent proxy report in all subscales and total PedsQL™ 4.0 GCS. The total PedsQL™ 4.0 GCS mean score reported by the child was 78.8 ± 15.6 compared to parent proxy report 61 ± 7.9 (t = 24.67, P ≤ .001).
There was a relatively lower score in the school function and emotional function of children and adolescents. About 34.5% of study participants in school functions and 35.8% in emotional functions had scored more than 1 standard deviation (>1 SD) below the total PedsQL™ 4.0 GCS mean score of self-report (Table 3).
Comparison of Child Self-Report and Parent Proxy Reports of HrQoL (Mean ± Standard Deviation), Addis Ababa, 2018.
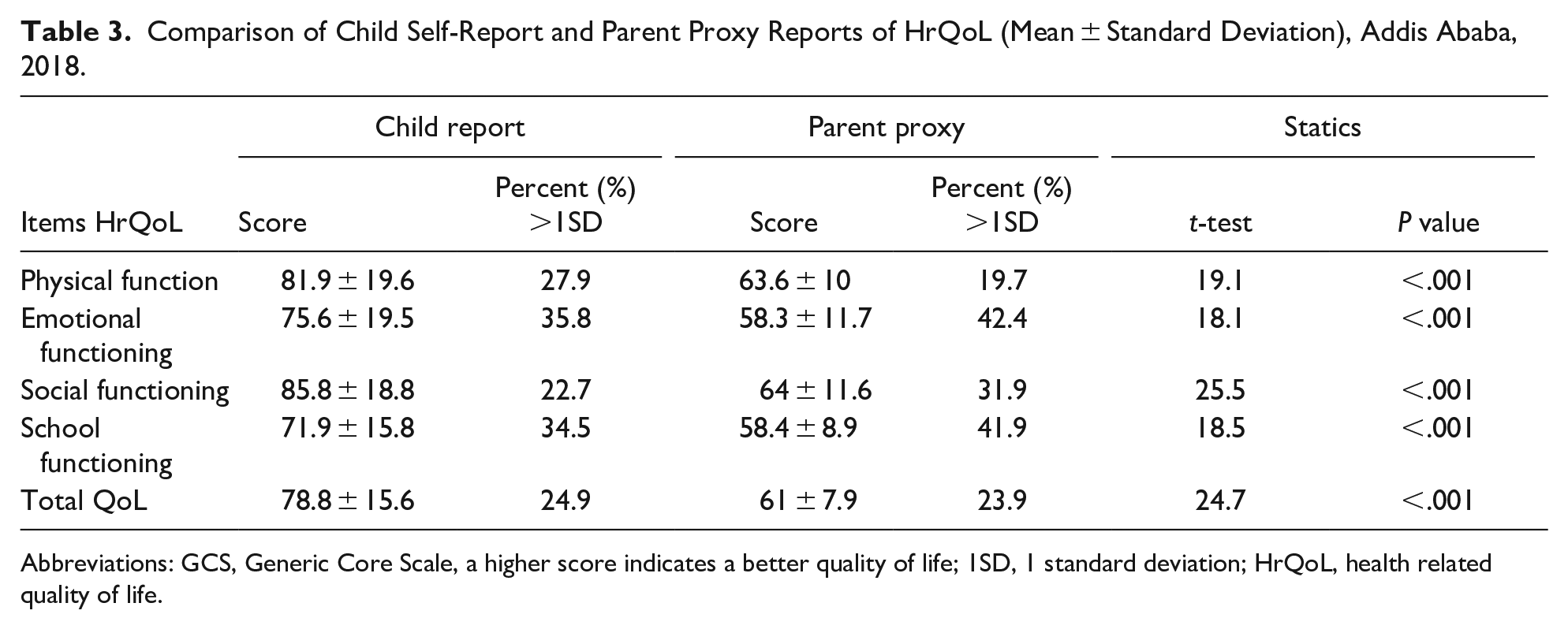
Abbreviations: GCS, Generic Core Scale, a higher score indicates a better quality of life; 1SD, 1 standard deviation; HrQoL, health related quality of life.
HrQoL Scores According to Sociodemographic Variables
According to the sociodemographic variables, the total HrQoL mean score of study participants were statistically deferent within age group (t = 4.2, P = .001),gender (t = 2.06, P = .041), number of children in the family (t = 5.2, P = .0001), educational level of mother (t = 4.8, P = .0001), educational level of father (t = 4.9, P = .0001) and monthly incomes of parents (t = −8.04, P = .0001) (Table 4)
HrQoLitems According to Sociodemographic Variables of Children and Adolescents, 2018 (Mean ± Standard Deviation).

HrQoL Scores According to Clinical Variables
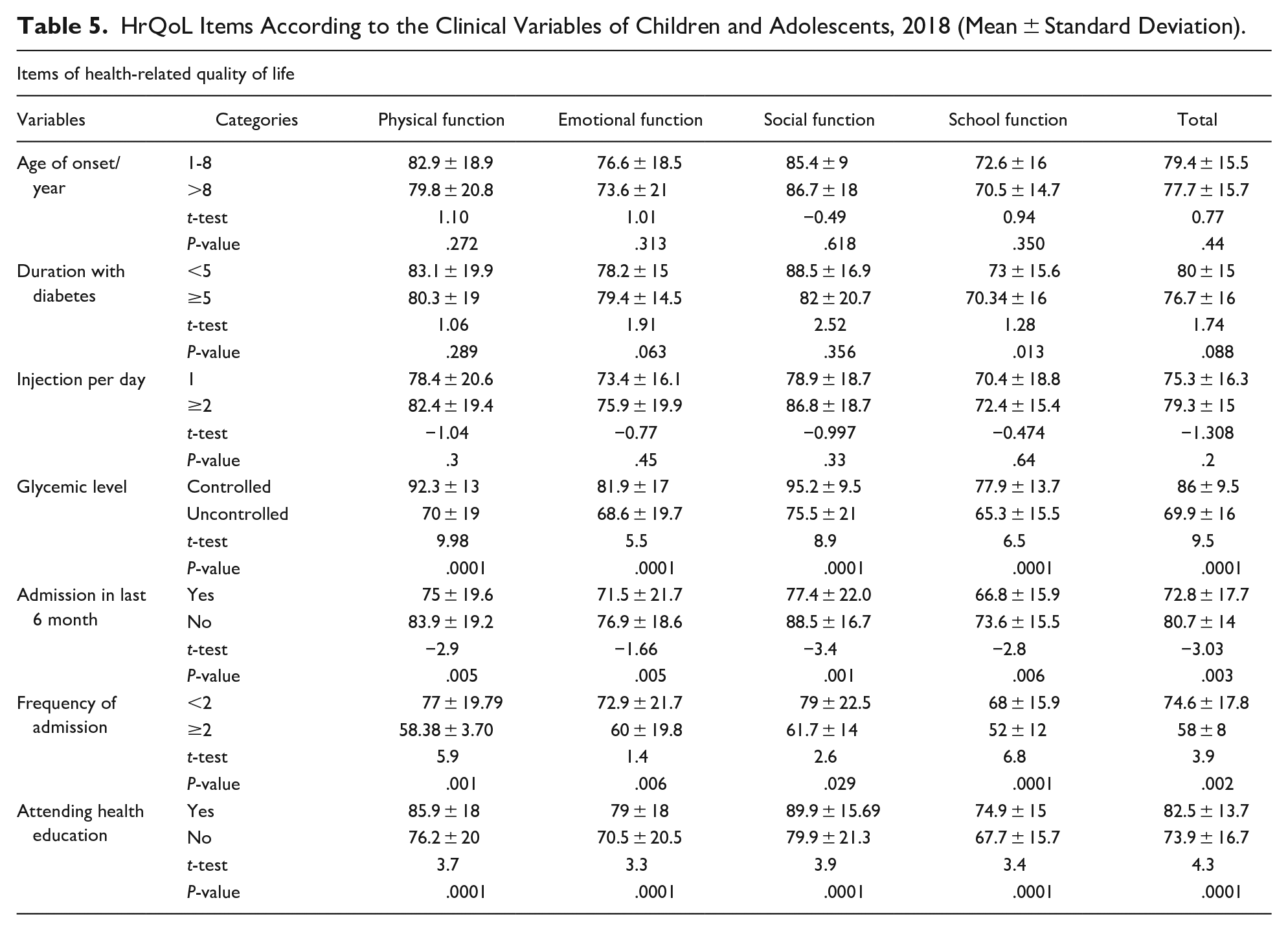
Regarding the clinical variables, the total HrQoL mean score of study participants were statically deferent within health education of diabetes (t = 4.3, P = .0001), blood glycemic level (t = 9.5, P = .0001), and frequency of hospital admission (t = 3.9, P = .002) (Table 5)
HrQoL Items According to the Clinical Variables of Children and Adolescents, 2018 (Mean ± Standard Deviation).
Predictor of quality of life
Based on multivariable linear regression analysis: female sex, number of children in the family, family income, health education of diabetes, glycemic level, and frequency of hospital admission were independent influencing factors of the HrQoL of children and adolescents. This had explained approximately half of the variability of the total HrQoL mean score (R 2 = 0.493, F = 37.910, P < .001).
Children who had well-controlled glycemic level had a better score in all subscale score of physical functioning (β = 17.6, 95%CI: 13.5, 21.7) emotional function (β = 8.4, 95%CI: 3.8, 12.9), social function (β = 13.5, 95%CI: 9.8, 17.1) school function (β = 8.6 95%CI: 4.8, 12.3) and total HrQoL (β = 11.8, 95%CI:8.7,14.9) when compare to children who had no well-controlled glycemic level.
Health education on diabetes were positively associated with to all sub scale score of physical functioning (β = 6.4, 95%CI: 2.4, 10.4), emotional functioning (β = 5.97, 95%CI: 1.5, 10.4), social functioning (β = 6.3, 95%CI: 2.76, 9.8), school function (β = 4.9, 95%CI: 1.3, 8.5) and the total HrQoL (β = 5.92, 95%CI: 2.9, 8.9).
A rising in number of children in the family were negatively associated with to all sub scales score of physical function (β = −2.4,95%CI:−4.7, −0.055),emotional function (β = −2.8, 95%CI: −5.4, −0.19), social function (β = −3.9, 95%CI: −5.9, −1.8), school function (β = −3.7, 95%CI:−5.8, −1.6) and the total HrQoL score (β = −2.9, 95%CI: −4.6, −1.3).
Female had scored lower in social function (β = −3.9, %95 CI:−7.4, −0.46), school function (β = −4.8, %95 CI:−8.3, −1.2) and in a total HrQoL (β = −3.6, 95%CI: −6.6, −0.7) than male participants. Similarly, children who had been admitted to hospital 2 or more times in the last 6 months had a poor score in the subscale of social function (β = −3.3, 95%CI: −5.9, −0.75), school function (β = −3.7 95%CI: −5.4, −0.10) and total HrQoL sore (β = −2.6, 95%CI: −4.8, −0.42) when compared to the children who had been admitted only one time (Table 6).
Multivariable Linear Regression Analysis of Predictor of HrQoL and its β Coefficients (95% Confidence Interval) of Children and Adolescents with Diabetes, Addis Ababa, 2018.

Significant at P < .05, Ref: indicates a category used as a standard reference.
Discussion
This study revealed that the emotional and school function of HrQoL of children and adolescents were somewhat low when compared to the other subscale of HrQoL. Which was in line with a study done in Turkey. 15 The impaired emotional function can be explained as children and adolescents might be worried about long-term complications of diabetes. On the other hand reduction in school function might be due to children and adolescents have missed a class for hospital follow-up or might be due to being unwell. So, health professionals, the school community, and parents must work integrally to improve the emotional and school function of children and adolescents.
In this study, the child self and parent proxy reports of total HrQoL of children and adolescents were statistically different (t = 24.7, P < .001). Parent proxy reports for children and adolescents HrQoL were lower which was similar to previous studies finding in Kuwait and Greece16,17 This might be explained by the closeness and involvement of parents in disease management forced them to perceive more likely about the impacts the diseases. This indicates that health professionals should not depend only on the information of parents/caregivers should be flexible to incorporate children’s information in clinical practice.
Even though gender did not affect the physical and emotional functions of HrQoL, it was a statistically significant predictor of the total HrQoL (β = −3.6, %95 CI: −6.6, −0.7) of children and adolescents. Females have reported lower total HrQoL scores compared to males. Which was in agreement with studies done in Saudi Arabiya and Kuwait.16,18 The possible justification might be due to that female supposed to work in the home, like caring for young children and home activities this will limit the time of peer play or it might be due to more social pressure and self-consciousness related to marriage and future birthing as girls approach puberty and adolescent.
In similar to a study conducted in Zambia 19 this study showed that health education about diabetes had significant positive associations with HrQoL of children and adolescents with diabetes (β = 5.92, 95%CI: 2.92, 8.9). Children and adolescents who had been participated in health education had a better HrQoL score. So health professionals should provide health education on diabetes self-management and diabetes care of children and adolescents to improve their quality of life (QoL).
In this study, children and adolescents who had well-controlled blood glucose levels had a better score in HrQoL (β = 11.8, 95%CI: 8.7, 14.9), this finding was in agreement with previous studies.16,17,20 The result of the current study can be explained by the fact that children and adolescents who had a well-controlled blood glucose level were associated with a decrease in cognitive function and associated with fewer structural changes in the brain, 21 they had better academic performance 22 and also the fact that in targeted blood glucose level the common acute complication of diabetes, like hypoglycemia, hyperglycemia and diabetics ketoacidosis will be minimized. This implies that children and adolescents should have been monitored and manage blood glucose levels at a targeted level. A health professional should strengthen health education in diabetes self-management and parents must work integrally to improve the QoL.
The other observed finding of this study was the monthly income of the parents had a statistically significant positive association with HrQoL (β = 9.4, 95%CI: 6.4, 12.4). Children and adolescents whose family members are high/medium monthly income had scored a better HrQoL. This was in line with studies conducted in Egypt, 23 this explained as having a good monthly income, enables the family to pay the requested fee for medical laboratories, medication and to purchase needed materials in diabetes self-management. So governmental or non-governmental organizations must compensate children and adolescents who are family members having low monthly incomes.
This study showed that the frequency of hospital admission was negatively associated with the total HrQoL (β = −2.6,95%CI:−4.8, −0.42). HrQoL was compromised in children and adolescents who had 2 or more hospital admission in the last 6 months. This finding was contrary to the study done Taranaki children indicated that more hospital admission was a predictor of better HrQoL. 24 The result of the current study might be during admission children and adolescents have spent more time in a hospital and missed a class, which will limit time to peer play, and also the admission might be due to an upset problem of the disease itself. So the blood glucose level should be monitored regularly, the health profession and parents must work integrity to support admitted children and adolescents.
This study shows that a rise in the number of children in the family had a statistically significant negative association with the HrQoL of children (β = −2.9, 95%CI: −4.6, −1.3). This was in line with a finding conducted in Turkey, 15 this might be due to siblings may not aware well of the impact of the disease or the rising number of children in family members may reduce parent’s support. So siblings must have been incorporated in diabetics’ health education and children and adolescents should support from all family members.
Limitation
The main limitation of this study included: 1 this study had no control group to compare with the study group, 2 other determining factors are not explored in this study such as family conflict, family relation.
Conclusion
In conclusion, this study found that there was a somewhat reduction in school function and emotional function of HrQoL of children and adolescents.
This study also concludes that well-controlled blood glucose level, medium/high monthly incomes, and health education of diabetes were an important predictor of better HrQoL
Having more hospital admission in the last 6 months and raised the number of children in the family was an important predictor of impaired HrQoL scores of children and adolescents.
Female gender was an influencing predictor of lower HrQoL scores.
Recommendations
Based on the result, this study will be recommended to:
Footnotes
Acknowledgements
We would like to pass our gratitude to the Addis Ababa University for the approval of ethical clearance and technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical clearance was obtained from the Ethical review committee of the department of nursing and midwifery from Addis Ababa University. An official letter of cooperation was written to the Addis Ababa health bureau and each health institution. After explaining the purpose of the study, written informed consent was obtained from parents of all participating children. Written consent was also requested from children over 12 years old. Participants were also informed that participation was voluntary and that they can withdraw at any time if they are not comfortable with the questionnaire. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality.
What is Already Known on This Topic?
Assessment of Health-related quality of life (HRQoL) is important to indicate the outcome of treatment and to predict the impact of disease on children and adolescents with diabetes. Measurement of HRQoL is an increasing clinical practice in a patient with chronic disease and it was recommended routinely to be done in conjunction with medical treatment.
What does This Study add?
We assessed the level of HrQoL of children and adolescents with diabetes in Ethiopia. We developed a predictive model to predict HrQoL of children and adolescents with diabetes.
Availability of Data and Materials
The data sets collected and analyzed for the current study are available from the corresponding author and can be obtained at a reasonable request.