
Abstract
Objectives:
This study aimed to assess the QoL of parents of children with type 1 diabetes mellitus.
Methods:
In this cross-sectional study, we recruited 190 parents of children with type 1 diabetes mellitus from 3 hospital in Jordan. The parents completed the PedsQL TM 2.0 FIM. We performed a descriptive analysis to describe sample characteristics and used multiple linear regression models to estimate the predictive effects of sociodemographic and clinical variables on the QoL of the parents.
Results:
The parents’ mean total PedsQL TM 2.0 FIM score was 55.75 ± 17.25. Income and area of residence were the only factors associated with this score: high income (B = 0.012 units, P = .042) and residence in Amman (B = −6.868 units, P = .017) predicted good QoL.
Conclusion:
The findings underscore the significance of an interdisciplinary, biopsychosocial, and family-centered care strategy for parents of children with type 1 diabetes mellitus.
Introduction
Type 1 diabetes mellitus (DM) is a chronic disease, also considered a family disease, when it affects children.1,2 Globally, type 1 DM is expected to represent 10% of all diabetes instances, with incidence rates are rising by 3% to 4% annually3,4
In Jordan, the incidence rate of type 1 DM among children aged 0 to 14 years is 0.6 per 1000 individuals. 5 The treatment and management regimen recommended for pediatric type 1 DM can be challenging and complex for the parents of affected children. 6 As such, these parents are often overwhelmed by not only the demands of type 1 DM care but also the complications of the disease.1,7 A parent of a child with type 1 DM may have psychological, physical, emotional, financial, and social care burdens. 2 These burdens may occur because of food management, diabetes-related family conflicts, regular blood glucose monitoring, insulin injection administration, as well as diet and physical activity monitoring, all with the final goal of parochial glycemic control. 6 Other reasons underlying these burdens may be related to the additional medical equipment and medication costs, time required for care, poor sleep, psychological strain, as well as the stigma related to having a child with type 1 DM. 1
A US study Commissariat et al 7 demonstrated that type 1 DM management places a substantial responsibility and emotional burden on families. In a Hungarian study, the mothers of children with type 1 DM reported lower resilience levels and more depressive symptoms than the mothers of healthy children. 8 In a Saudi Arabian study, the parents of adolescents with type 1 DM who were receiving interdisciplinary and family-centered care demonstrated low Pediatric QoL Inventory (PedsQL) Family Impact Module (PedsQL-FIM) scores in the emotional subscale; this finding emphasizes the importance of biopsychosocial well-being. 9 In a Lebanese study, parents reported that they experienced psychological stress and guilt and had financial burdens and social restrictions. 10
The cultural differences between Western and Middle Eastern parents are correlated with substantial differences in their QoL perceptions. Many studies on the QoL of parents of children with type 1 DM have been conducted in Western countries; however, few relevant studies have been conducted in Arab countries.9,10 Therefore, the current study assessed the perceived QoL of parents of children with type 1 DM in Jordan.
Research Questions
Our research questions are as follows:
(1) What is the perceived QoL of the parents of children with type 1 DM in Jordan?
(2) What is the relationship between this QoL and the socioeconomic and clinical characteristics of these parents and their children?
Methods
Design and Sample
In this cross-sectional study, we included parents of children diagnosed with type 1 DM at 3 hospitals in Jordan between October 2022 and January 2023.
We used Tabachnick and Fidell 11 formula to determine the appropriate study sample size: N = 50 + 8 m, where m = number of independent variables. In the present study, 17 independent variables were studied; therefore, the required sample to detect preconception care awareness at a significance level of 0.05 was 170 children and 170 parents (mothers or fathers). However, to compensate for incorrect data and incomplete questionnaires, we added 10% to the original sample size; finally, we included 190 children and 190 parents in our sample population.
We invited individuals who (1) had <18-year-old children diagnosed as having type 1 DM for ≥1 year in Jordan; (2) provided informed consent to participate in this study; and (3) could read, write, and speak in Arabic to participate in this study.
Settings
Our participants were recruited from 3 major hospitals in Jordan: 1 in Amman (the capital city; University of Jordan Hospital) and 2 in the North Region (King Abdallah University Hospital and Princess Rahma Teaching Hospital). We selected these hospitals because they are large and have inpatient and outpatient units specializing in endocrine services for pediatric type 1 DM, which involve the patients’ parents.
Instruments
Demographic Characteristics Questionnaire
Through a self-reported questionnaire, we collected the participants’ sociodemographic and clinical data: their age, sex, current area of residence, highest education level, employment status, marital status, and total income, along with their children’s age, sex, and current area of residence.
The PedsQL™ Family Impact Module Scales (Version 2.0)
The PedsQL™ Family Impact Module Scales (version 2.0) was used for measuring the QoL of parents of children with type 1 DM. 12 The newly developed PedsQL Family Impact Module was created to assess the effects of chronic pediatric health problems on parents and the family unit. The PedsQL Family Impact Module assesses parents’ self-reported physical, emotional, social, and cognitive functioning, as well as communication and concerns. The Module further assesses parent-reported familial daily activities and interpersonal family dynamics. 12
It is a questionnaire comprising 36 items divided among 8 QoL subscales: physical (6 items), emotional (5 items), social (4 items), cognitive functioning (5 items), communication (3 items), worry (5 items), daily activities (3 items), and family relationships (5 items). For each item, the scores are rated on a 5-point Likert scale, ranging from 0 (Never a problem) to 4 (Almost always a problem). Next, these points were reversely scored and then linearly transformed (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0) to obtain a final product out of 100. Finally, the total scores were calculated by averaging the scores of all subscales. The higher the scores, the higher the health-related QoL or functioning. According to, 12 the PedsQL-FIM (version 2.0) has a reliability index of 0.82 to 0.97; therefore, it has been widely used in other studies.8,9,13 We also obtained the approval of James Walter Varni, one of the creators of the PedsQL-FIM (version 2.0), for use in this study.
A panel of 3 experts translated the PedsQL™ Family Impact Module Scales (version 2.0) from English to Arabic and then back-translated it from Arabic to English to ensure that the original (English) and translated (Arabic) tools measured identical concepts. The experts also reviewed the face and content validity of the translated tool. Next, to compute the reliability of this tool, we conducted a pilot study including 20 parents of children with type 1 DM; the resulting Cronbach’s α values for the total scale and subscales ranged between 0.714 and 0.888 (Table 1)—which is above the recommended value of 0.70, suggesting reasonable reliability. 14 The pilot study participants were excluded from the current study sample.
Cronbach’s Alpha for PedsQL TM 2.0 Family Impact Module.

Abbreviation: Peds QL, Pediatric Quality of life.
Data Collection Procedure
The principal investigator collected all data through face-to-face interviews using a structured questionnaire. The participants were interviewed in a private room at the study hospitals before or after their children’s consultations at the hospitals. Before conducting the interview, the principal investigator explained the nature, purpose, risks, and benefits of the study and then asked the participants to sign informed consent forms to confirm that they still agreed to participate. The principal investigator then administered a paper-based, self-reported questionnaire survey containing the demographic characteristics questionnaire as well as the translated PedsQL™ Family Impact Module Scales (version 2.0). In general, the time required to fill out the questionnaire survey was ≤15 minutes.
Statistical Analysis
All data analyses were conducted using the Statistical Package for the Social Sciences (version 28). Descriptive statistics were used to describe sample characteristics and variables and identify data distribution, whereas means and their standard deviations were used to represent the scale data. Multiple linear regression models were used to estimate the predictive effects of the participants’ and their children’s sociodemographic and clinical variables on the participants’ QoL. An α value of ≤.05 was considered to indicate statistical significance.
Ethical Approval and Informed Consent
This study was granted approval by the Institutional Review Board of the Jordan University of Science and Technology and the Jordan Ministry of Health. The researchers gained ethical approval from the Institutional Review Board (IRB) at Jordan University of Science and Technology to gather data from King Abdullah University Hospital (approved number 51/143/2021) and the University of Jordan Hospital (approval number 301/2022). Authorization was also acquired by the Jordanian Ministry of Health, with the reference number MOH/REC/2022/287, to collect data from Princess Rahma Teaching Hospital.
All participants were asked to provide written informed consent after they were informed that their participation was completely voluntary and that they had the right to withdraw from the study at any time without consequence. To maintain participant anonymity throughout the study, we assigned each participant a number as a data collection identifier.
Results
Characteristics of Participants and Their Children
Of the 190 participating parents, most were female (n = 182; 95.8%), were married (n = 185; 97.4%), were from the Central Region of Jordan (n = 71; 37.4%) and had an education level of diploma or lower (n = 128; 67.4%). The mean age of the participants was 38.0 ± 6.66 years, whereas their mean monthly income was 640 ± 286 USD (See Table 2).
Parents Socio-Demographical Characteristics (N = 190).

PedsQL-FIM Scores
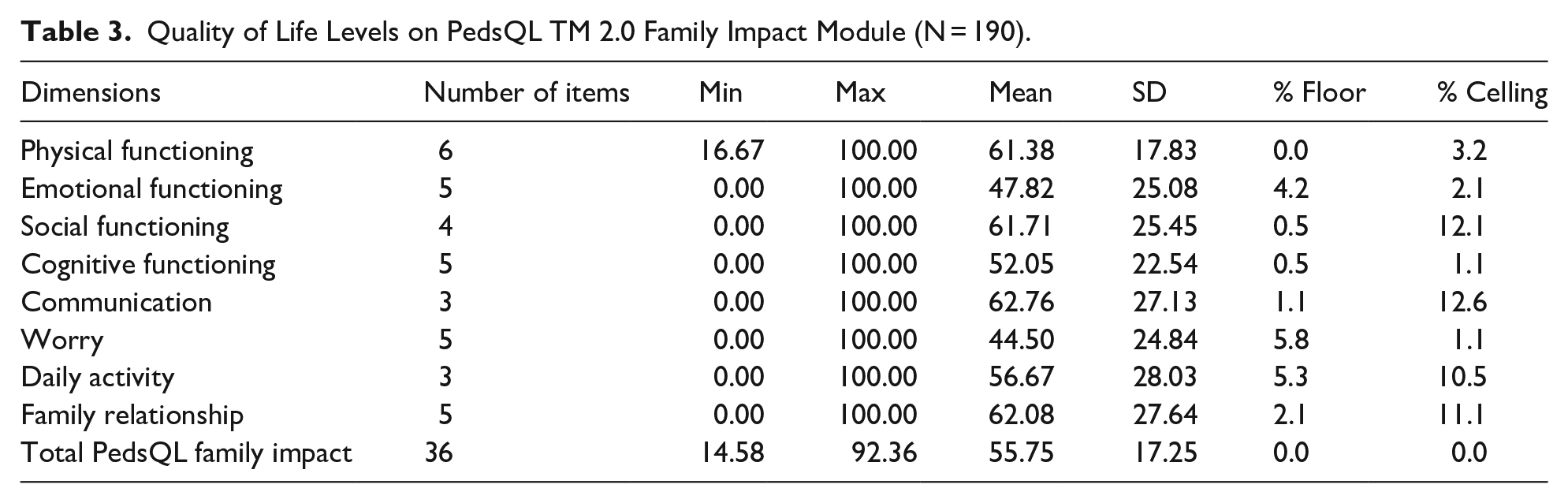
The total PedsQL-FIM scores were 55.75 ± 17.25 (Table 3). Moreover, the participants performed poorly on individual subscales. Furthermore, the mean physical, social, cognitive functioning, communication, and family relationship subscale scores were similar.
Quality of Life Levels on PedsQL TM 2.0 Family Impact Module (N = 190).
Effects of Sociodemographic and Clinical Characteristics on PedsQL-FIM Scores
To increase the validity of our multiple linear regression analysis, we excluded the participants’ sex and marital status because of a sample size imbalance. The participants’ income demonstrated a positive effect on their emotional functioning (B = 0.017 units, P = .049), explaining 1.5% of the variance. Compared with non-working participants, working participants demonstrated higher social functioning (B = 3.475 units, P = .027), explaining 2.3% of the variance. Moreover, compared with those living in Amman (Jordan’s capital), the participants living in the Central Region of Jordan (i.e., Salt, Zarqa, and Madaba) exhibited lower cognitive functioning (B = −9.828 units, P = .009) and daily activity (B = −11.40 units, P = .006), explaining 2.9% and 4.3% of the variance, respectively. Furthermore, for every 1 JOD increment in income, the family relationship subscale score increased by 0.022 units (P = .026); moreover, compared with those living in Amman, the participants living in the South Region demonstrated better family relationships (B = 11.576 units, P = .041). For every 1-year increment in participant age, the family relationship subscale score decreased by 0.719 units (P = .015), explaining 7.3% of the variance. Only 2 factors demonstrated significant correlations: high income increased the total PedsQL-FIM score by 0.012 units (P = .042), whereas living in the Central Region reduced it by 6.868 units (P = .017)—both explaining 3.3% of the total variation. Finally, the participants’ sociodemographic factors demonstrated no significant impact on their physical functioning, communication, and worry subscale scores (Table 4).
Predictions’ of PedsQL TM 2.0 Family Impact Module and Quality of Life Among Parents (N = 190).

Discussion
In this study, we assessed the perceived QoL of parents of children with type 1 DM in Jordan using the PedsQL TM 2.0 Family Impact Module; the parents demonstrated a mean total PedsQLTM 2.0 Family Impact Module score of 55.75 ± 17.25. This score is lower than the score of the study conducted other countries such as Saudi Arabia (67.3). 9 The relatively low total PedsQLTM 2.0 Family Impact Module scores noted in the current study may be related to the burden of having children with diabetes. Parents of children with type 1 diabetes mellitus face numerous burdens, including psychological, physical, and social challenges. They contended with the psychological burdens of hypoglycemic apprehension, the stress of handling their children’s requirements, as well as depression and anxiety. 6 Besides psychological issues, type 1 DM parents suffer physical ones. These include monitoring blood sugar levels, giving insulin shots, and managing disease consequences. Parents can be exhausted by managing their child’s diabetes physically. 2
In the current study, the parents demonstrated high scores on the physical, social, cognitive functioning, communication, and family relationship subscales of the PedsQLTM 2.0 Family Impact Module score but low scores on the worry subscale. This result is similar to that reported previously: Parents demonstrated the most significant differences in the worry subscale scores.9,15,16 A study indicated a weak, negative, and significant correlation between the parents’ worry subscale and total scores on the PedsQLTM 2.0 Family Impact Module score; it also indicated that the parents’ worry subscale scores were high, indicating that the parents had poor QoL. 17 This worry mainly resulted from the parents’ awareness of the challenges related to lifestyle changes required by their children; it may also be associated with their concerns regarding the short- and long-term complications and hypoglycemic episodes experienced by their children.9,16
Parents typically indicate that their family life completely changes after their children are diagnosed with type 1 DM; they also are burdened by their children’s situation and are worried about the possible complications. 6 In a study conducted to evaluate the generic health-related quality of life of young children with type 1 DM in relation to their healthy peers, considering family dynamics and maternal psychological health. Mothers of children with diabetes had diminished resilience and increased depression symptoms compared to mothers of healthy counterparts. 18 The current results were consistent with those reported previously. As such, the parents of children with type 1 DM require financial and psychological support and counseling to help them cope with the increased burden of care.
In the current study, the parents’ income and area of residence predicted their total PedsQLTM 2.0 Family Impact Module score. In particular, compared with low income, high income improved the parents’ QoL by 0.012 units; in contrast, compared with residence in Amman, that in the Central Region of Jordan (i.e., Salt, Zarqa, and Madaba) worsened the parents’ QoL by 6.868 units. The parents’ income also had a significant, positive effect on the PedsQLTM 2.0 Family Impact Module subscale scores; the higher the parents’ income, the higher their emotional and family relationship subscale scores. Families of children with type 1 DM encounter financial issues and social restrictions. 10 Chronic diseases impose a large economic burden on the affected children’s families because they require long-term care, follow-up, monitoring, and supervision. 6 According to World Health Organization, 19 type 1 DM and its complications pose a significant economic burden on individuals and their families because of the resulting health care expenditure and earning capacity loss. Nassif and Noueiri 10 reported that parents’ financial burden negatively affects the QoL of the families of children with type 1 DM. Therefore, only parents with a high income can easily bear the financial burden of chronic diseases. These results are consistent with those of the current study.
Compared with those living in the Central Region, the parents living in Amman demonstrated better cognitive functioning and daily activity. This result corroborates that of Grudziąż-Sękowska et al 20 : in children with type 1 DM, living outside urban areas is associated with decreased educational facility or health care access and worsened overall health. Decreased accessibility to educational facilities and services in the Central Region of Jordan may be the reason underlying the low cognitive functioning subscale scores; in contrast, the low daily activity subscale scores in this area may be related to sedentary lifestyle (including a lack of sport participation and movement).
In the current study, working parents demonstrated higher social subscale scores than non-working parents (B = 3.475 units, P = .027). This result is inconsistent with that reported previously: working parents have poorer QoL than non-working parents.1,21 Caring of children with type 1 DM may be influence women’ employment choices, leading some to resign or decrease their working hours to facilitate childcare from home. 22 A study in the Anatolia region demonstrated that mothers were required to rearrange their work schedules or quit their jobs to treat and manage the type 1 DM of their children. 1 These mothers also indicated that they had financial issues; according to these mothers, caregiving involves “the changes in life and running out of everything” and “always being alert.” 1
A key findings of the current study was that every 1-year increment in the parents’ age was associated with a decrease in the family relationship subscale scores by 0.719 units; this result is consistent with that reported previously: mothers aged ≥41 years have a significantly increased care burden. 1 This may be because children with type 1 DM require regular management and monitoring throughout their lives. In the case of children with type 1 DM, the diabetes management burden is placed mainly on their parents; this may negatively affect family communication, eventually leading to worsened family relationships.
Practical Implications
Parents may need direct instruction from qualified health professionals. Their challenges could be mitigated through continuous diabetes education offered by medical personnel, and they were especially keen in acquiring knowledge regarding the latest technologies, probable consequences, and comprehensive diabetes treatment, thereby potentially reducing parental stress associated with disease management. 7 This assistance would significantly reduce parental stress and improve their quality of life. The application of clinical expertise, provision of therapeutic assistance, and education regarding the child’s illness, together with accessibility, understanding, empathy, and communication, are vital components in assisting parents.
Health care organizations should update and develop existing practice protocols to enhance their use of diabetes management guidelines and close the gap between evidence-based research findings and the current care practices of children with type 1 DM and their parents.
In hospital setting, health care providers play an important role in the periodic assessment of the QoL of parents of children with type 1 DM, as well as the regular monitoring of the application of diabetes management guidelines, thereby facilitating the ongoing evaluation of the efficacy of diabetes treatment. Consequently, this will make it easier to identify the educational requirements of parents of children with type 1 DM.
Limitations
This study has several limitations. First, we employed a cross-sectional design, in which data were collected at only one time point. The current results may thus be confirmed through additional longitudinal studies exploring the QoL of parents of children and adolescents with type 1 DM. Second, we used convenience sampling, which limited the generalizability of our findings. Finally, we used a self-reported questionnaire for data collection. As such, in the current study, some responses were incomplete, and some data could not be collected; moreover, the collected data possibly included self-report bias. Additional qualitative studies with a quantitative design may aid in achieving relatively accurate results related to the QoL of parents of children and adolescents with type 1 DM. Finally, the absence of a comparison group may be considered a significant drawback of the current study. The study indicates poor scores for parents of children with type 1 diabetes mellitus; however, without a comparative analysis, it is possible that parents of children without diabetes in the same region may exhibit similar scores, suggesting that the lower results may not be attributable to diabetes at all.
Recommendations
First, additional larger-scale nationwide studies are required to obtain a broader picture of the QoL of parents of children with type 1 DM in Jordan and its association with Jordan’s diabetes management guidelines. Second, the factors underlying the differences in QoL among parents of children with type 1 DM and their diabetes management practices and guidelines remain unclear; therefore, additional comprehensive studies on the demographic and socioeconomic characteristics of the affected children’s parents are warranted. Third, qualitative, longitudinal studies focused on diabetes management guidelines and aspects of life affect in different situations and over long periods are necessary. Finally, additional comparison studies are necessary to evaluate the quality of life of parents with type 1 diabetes mellitus in relation to their healthy counterparts, in order to elucidate the disparities between these 2 groups.
Conclusion
Major hormonal, developmental, and psychological changes occur throughout childhood and adolescence. These periods are, therefore, stressful not only for children and adolescents but also for their parents. Type 1 DM treatment and care, which involves multiple lifestyle and psychosocial changes, can further increase this stress. In particular, they may improve the health outcomes of children and adolescents with type 1 DM, but worsen the QoL of their parents. Therefore, the development of diabetes management designed to address the specific challenges of parenting children and adolescents with type 1 DM is highly warranted. In other words, broad multidisciplinary approaches for comprehensive pediatric type 1 DM care in a developmentally appropriate manner and improvement of parents’ QoL should be developed.
Footnotes
Acknowledgements
We would like to express our gratitude to all individuals who helped us with data collection at King Abdullah University Hospital, the Ministry of Health, Princess Rahma Hospital, and Jordan University Hospital. We also thank all the parents who participated in this study.