
Abstract
Objective:
Diabetes as a silent epidemic and one of the top four causes of death in the world. This study was designed to evaluate the quality of life and depression in family caregivers of patients with type 1 diabetes in Iran.
Methods:
The study was case–control study (cases, n = 50; controls, n = 50). The cases consisted of family caregivers of patients with type 1 diabetes who referred to the endocrinology clinic of Kosar Hospital in Semnan in 2020. The controls were a random sample from among family caregivers of non-diabetic patients who had referred to the same center in the same year. Demographic and family variables, the 36-Item Short Form Survey questionnaire, and Beck’s Depression Inventory were used to collect data. Univariate and multivariable logistic regression models with receiver operator characteristic (ROC) curve were used to data analysis in STATA 14.
Results:
The multivariable logistic regression model showed a significant association between existence of a patient with type 1 diabetes with number of caregivers’ children (odds ratio (OR) = 1.77; 95% confidence interval (CI): 1.06–2.94), quality of life (OR = 0.82; 95% CI: 0.74–0.90), sex (OR = 10.04; 95% CI: 2.29–43.99), and income level of caregivers (OR = 6.49; 95% CI: 1.35–31.08); however, it did not show a significant relationship with depression (OR = 1.02; 95% CI: 0.94–1.10).
Conclusion:
The quality of life in family caregivers of type 1 diabetics is low and gender, income level, and number of caregivers’ children were the most important factors predicting it. Therefore, psychological interventions to manage stress and improve the quality of life of family caregivers are recommended.
Introduction
Diabetes, as a silent epidemic and one of the top four causes of death in the world, is the most common metabolic disease with an increasing prevalence that can reduce life expectancy by one-third.1,2 Type 1 diabetes is the most common endocrine metabolic disease in children and adolescents with significant emotional and physical consequences. 3 The disorder is characterized by the destruction of islets of Langerhans and insulin-secreting β1 cells in the pancreas by the immune response, which is treated by replacing the lack or deficiency of insulin. 4 The prevalence of type 1 diabetes in children is increasing worldwide so that about 1 in every 300–500 children and adolescents under 18 years suffer from this disease. In Iran, the annual incidence of type 1 diabetes is estimated at about 3.7 per 100,000, and among the 5–7 million patients with diabetes, 50,000 are children and adolescents with type 1 diabetes.5,6 The disease causes direct costs of 2.5–15% (58912.4096 to 353474.4576 billion) of the total health budget and indirect costs that are several times higher and cause complications such as ischemic heart disease, hypertension, retinopathy, and neuropathy. 7 Family history (presence of a person with diabetes in the family), age (especially childhood and adolescence), geographic region (areas with northern climate), and contracting some viral diseases in childhood such as measles, rubella, and mumps, are important risk factors for type 1 diabetes in Iran and the world.8,6
Diabetes can affect physical function, the development of complications, mental health, personal, family and social relationships, sexual function, and perception of health.9,10 The prognosis and quality of life of patients with diabetes are dependent on the progression and severity of chronic complications, especially cardiovascular disease. 11 In addition to financial costs, diabetes comes with intangible costs such as pain, anxiety, discomfort, headache, disability, stress, depression, infection, amputation, and nutritional problems.12,13 Various studies have shown that with the onset of diabetes, in addition to the person with diabetes, family caregivers experience decreased social activity, increased family stress, and lost work time, all of which affect quality of life. Family caregivers of patients with type 1 diabetes show significantly lower levels of quality of life than family caregivers of type 2 diabetes and the general population. Age and duration of illness, education level of family caregivers, marital status, and health level are related to quality of life of family caregivers.14,15 Kobos E et al. have also reported that the highest levels of burden in family caregivers with type 1 diabetes are related to general stress and frustration. In addition, the amount of burden is related to the patient’s age, employment status, family caregiver education level, number of night blood sugar tests, frequency of hyperglycemia episodes, and number of hospitalizations. 16
Another problem for family caregivers of type 1 diabetic patients is depression. Evidence suggests that mothers caring for a child with a chronic illness are at greater risk for depression. About one-third of mothers with children with type 1 diabetes develop depression during their child’s illness. 17 Anxiety and depression in parents can be associated with a reduced sense of responsibility for their children’s care, education, and nutrition. Depression in mothers of children with type 1 diabetes is directly related to poor psychological adjustment of the child and adherence to disease care, which can eventually lead to poor blood sugar control. 18 Considering the importance of assessing the quality of life and depression in caregivers of type 1 diabetic patients on the one hand and the limited studies conducted in Iran especially the case–control studies in this field on the other hand, this study was designed to evaluate the quality of life and depression in family caregivers of patients with type 1 diabetes in Iran.
Materials and methods
Study design and subjects
This case–control study was designed to evaluate the quality of life and depression in family caregivers of patients with type 1 diabetes in Semnan city (Iran). The study was conducted as a census so that all patients with type 1 diabetes who visited the endocrinology clinic of Kausar Hospital during the first 6 months of 2020 were examined. Then, one control was selected for each type 1 diabetic patient. The controls were a random sample from among family caregivers of non-diabetic patients who had referred to the same center in the same time. Therefore, after 6 months, the case group (diabetes caregivers) consisted of 50 family caregivers of patients with type 1 diabetes who referred to the endocrinology clinic of Kosar Hospital of Semnan, in other words, first 50 patients with type 1 diabetes were identified then one of their family was selected as the family caregiver. The control group also included 50 family caregivers of non-diabetic patients who had referred to the same center for periodic and routine examinations. A family caregiver was a member of the patient’s family or relatives who cared for the patient and did not charge for his or her care. In married and single patients, spouse and parents were considered as family caregivers, respectively. The sampling method was convenience sampling. Inclusion criteria for family caregivers consisted of age 18–59 years and informed consent of the caregivers and patients to participate in the research. Exclusion criteria include alcohol use, smoking/drug use, psychedelics, and unfortunate family experiences in the last 6 months such as death, history of mental and chronic illness.
How to conduct the study
After the approval of the ethics committee, first, type 1 diabetes patients who had visited the endocrinology clinic of Kausar Hospital in Semnan city in 2018 for periodical examination were identified. Then, the patients were asked to ask their family caregivers to attend the present study at Kausar Semnan Hospital on a certain date. After the presence of diabetic patients and their caregivers, the objectives of the research were first explained to them, then, if they wanted to participate in the study, informed and written consent was obtained from them. Then, to select the control group (non-diabetes caregivers), people without type 1 diabetes (diseases such as thyroid disorders and goiter) who visited the endocrinology clinic of the same hospital in 2018 for periodical and routine examinations were identified, and the same procedures that were done for diabetes caregivers were repeated for them. The current study lasted for 6 months from writing the proposal to data collection.
Data collection
In addition to demographic and family data, the 36-Item Short Form Survey (SF-36) questionnaire and Beck’s Depression Inventory were used to collect data. The SF-36 questionnaire, which assesses health-related quality of life, consists of eight scales: 1—Physical function (PF, 10 questions), 2—Role limitation due to Physical Health (RP, 4 questions), 3—Role limitation due to Emotional Problems (RE, 5 questions), 4—Energy/Fatigue (EF, 4 questions), 5—Emotional Well-being (EW, 3 questions), 6—Social Functioning (SF, 2 questions), 7—Pain (P, 2 questions), and 8—General Health (GH, 6 questions). The answers to the questions are based on the Likert scale of 5 points and are scored from 1 to 5. Raw domain scores for the SF-36 were transformed to a 0–100, then total score that represents the mean of the total of the eight subscales was calculated and then it was divided into four levels: poor quality of life ⩽ 40; moderate = 40–60; good = 61–80, and excellent = 81–100. The validity and reliability of the SF-36 questionnaire in Iran have already been evaluated and confirmed. 19
The Beck Depression Inventory consists of 21 questions designed to assess the feedback and symptoms of depressed patients. Each item will receive a score between 0 and 3, and the total score of the questionnaire will range from 0 to 63. In all, 21 items of this questionnaire are classified into three groups: emotional (8 questions), cognitive (8 questions), and physical (5 questions) symptoms of depression. By adding the scores in each of the items, the individual score is obtained directly (0–13: No or minimal depression −14 to 19: Mild depression −20 to 28: Moderate depression and 29–63: Severe depression). This questionnaire has already been validated and reliable in Iran. 20
Statistical analysis
Data were analyzed using Stata software version 14.0 (Stata Corp, College Station, TX, USA). Mean, standard deviation (SD), and frequency (%) were applied for descriptive analyses. Then, univariate and multivariate logistic regression models were used to determine the relationship between type 1 diabetes with quality of life and depression in their family caregivers and crude and adjusted odds ratio (OR) with 95% confidence interval (CI) were reported. OR is an epidemiological index that is used to measure the strength of association between two events, A and B. The OR is defined as the ratio of the odds of A in the presence of B and the odds of A in the absence of B, or equivalently (due to symmetry), the ratio of the odds of B in the presence of A and the odds of B in the absence of A. If the OR = 1, that is, the odds of one event are the same in either the presence or absence of the other event. If the OR > 1, then A and B are associated in the sense that, compared to the absence of B, the presence of B raises the odds of A, and symmetrically the presence of A raises the odds of B. Conversely, if the OR < 1, then A and B are negatively associated, and the presence of one event reduces the odds of the other event. Also, the area under the ROC curve was used for assessment discriminative ability of the multivariable logistic regression model.
Ethics considerations
Before data collection, the aims of the research were explained to the caregivers and patients, then written informed consent was obtained from them. This study was approved by the Deputy of Research and Ethics Committee of Semnan University of Medical Sciences (Iran) (ID: SEMUMS.REC.139288).
Results
This case–control study was designed to determine the relationship between existence of a person with type 1 diabetes with quality of life and depression in their family caregivers in Semnan city (diabetes caregivers = 50 family caregivers of people with type versus non-diabetes caregivers = 50 family caregivers of people with non-type 1 diabetes). The mean ages (±SD) in the two groups of diabetes and non-diabetes caregivers were 37.5 (±8.5) and 36.9 (±7.9), respectively.
Table 1 shows the demographic and family characteristics of patients and their caregivers in the two groups of diabetes and non-diabetes caregivers. As you see, 56% of patients were male and most of them were under 25 years old. Also, the majority of patents had no complications and the type of treatment received was injectable. The number (%) of female caregivers in the diabetes caregivers and non-diabetes caregivers were (58%) 29 and 37 (74%), respectively. The mean (SD) age of caregivers in two groups was 37.5 (8.5) and 37.4 (8.7) years, respectively. The majority of caregivers in both groups were married (86% versus 92%), housewives (48% versus 50%), and city dwellers (96% versus 98%) with low income level (64% versus 80%). The highest family relative of caregivers the two groups belonged to the mother. Other details of these variables are shown in Table 1.
Demographic and family characteristics of patients and their caregivers in the two groups of diabetes and non-diabetes caregivers.

Table 2 shows the descriptive characteristics of quality of life and its subscales in the two groups of diabetes and non-diabetes caregivers. The means (SD) of overall quality of life, overall physical health subscale, and overall mental health subscale for the two groups of diabetes and non-diabetes caregivers were 59 (8.5) versus 64.6 (5.3), 65.5 (11.9) versus 70.3 (7.6) and 50.2 (10.3) versus 57.8 (7.4), respectively. Also, non-diabetes caregivers (good = 96%) had better quality of life than diabetes caregivers (good = 62%).
Descriptive characteristics of quality of life and its subscales in the two groups of diabetes and non-diabetes caregivers.

Table 3 shows the descriptive characteristics of Beck’s Depression Inventory and its subscales in the two groups of diabetes and non-diabetes caregivers. The means (SD) of Beck’s Depression Inventory for the two groups of diabetes and non-diabetes caregivers were 15.6 (9) versus 8.9 (7.1), respectively. Most people in both groups also had mild depression (74 versus 92%).
Descriptive characteristics of Beck’s Depression Inventory and its subscales in the two groups of diabetes and non-diabetes caregivers.

Table 4 shows the relationship between type 1 diabetes with quality of life and depression in their family caregivers by univariate logistic regression model. As can be seen, a statistically significant difference was found between existence of a patient with type 1 diabetes with number of caregivers’ children, depression, quality of life, sex, income level, and education of caregivers (p ⩽ 0.20).
The relationship between type 1 diabetes with quality of life and depression in their family caregivers by univariate logistic regression model.
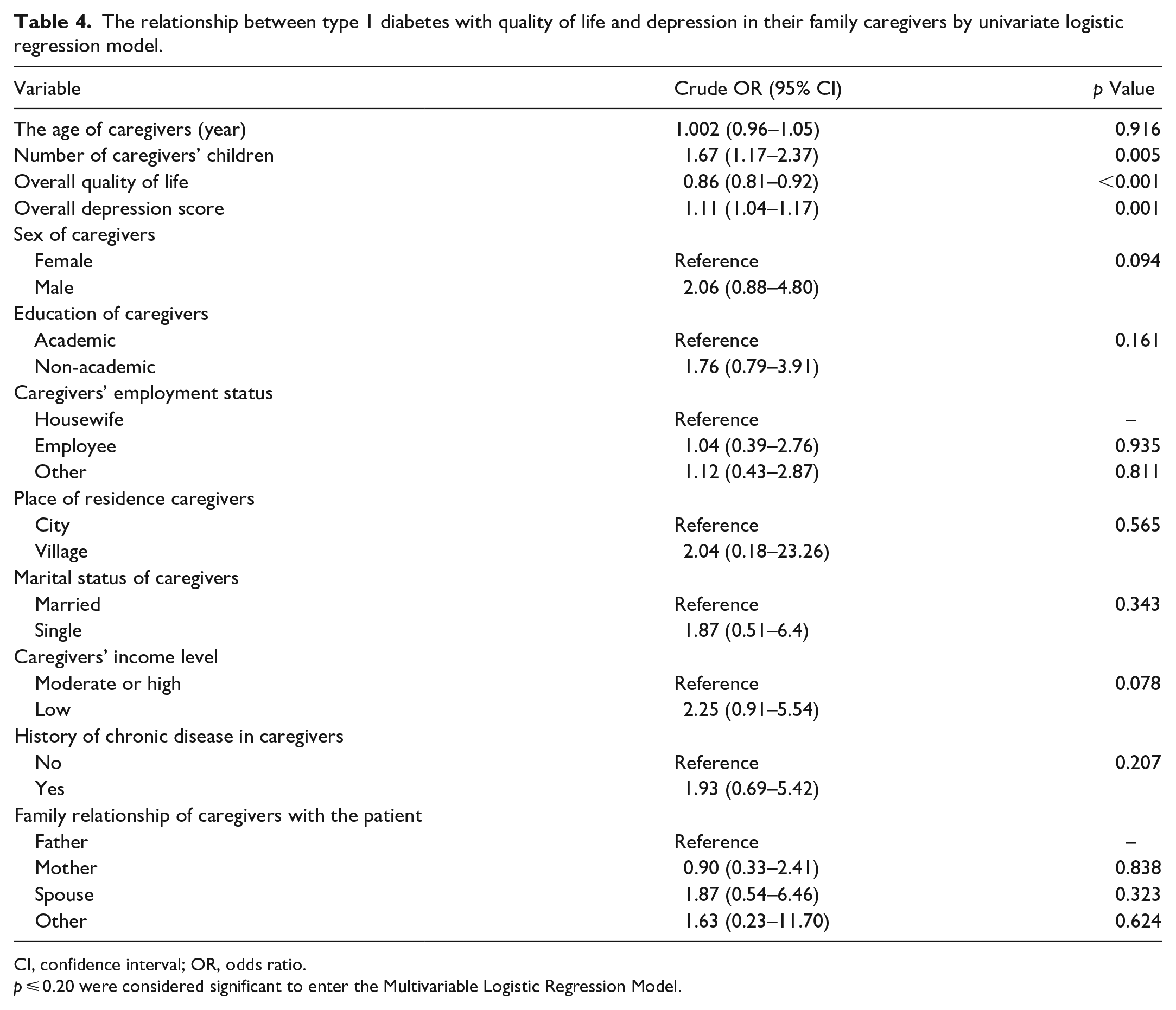
CI, confidence interval; OR, odds ratio.
p ⩽ 0.20 were considered significant to enter the Multivariable Logistic Regression Model.
Table 5 shows OR and 95% CI derived from multivariate logistic regression model for relationship between type 1 diabetes with quality of life and depression in their family caregivers. As can be seen, after adjusting for the confounding variables, a statistically significant difference was observed between existence of a patient with type 1 diabetes with number of caregivers’ children, quality of life, sex and income level of caregivers (p < 0.05). For quality of life, OR adjusted = 0.82 (95% CI: 0.74–0.90), this means which after adjusting for the confounding variables, the quality of life in caregivers of the diabetes caregivers is 0.18 units lower than the non-diabetes caregivers.
The relationship between type 1 diabetes with quality of life and depression in their family caregivers by multivariate logistic regression model.

CI, confidence interval; OR, odds ratio.
Bold indicates the significant value <0.05.
Figure 1 demonstrates the area under the ROC curve for significant variables included in the multivariable logistic regression model which the area under the ROC curve was 90.60%, which demonstrates the high discriminative power of this model.
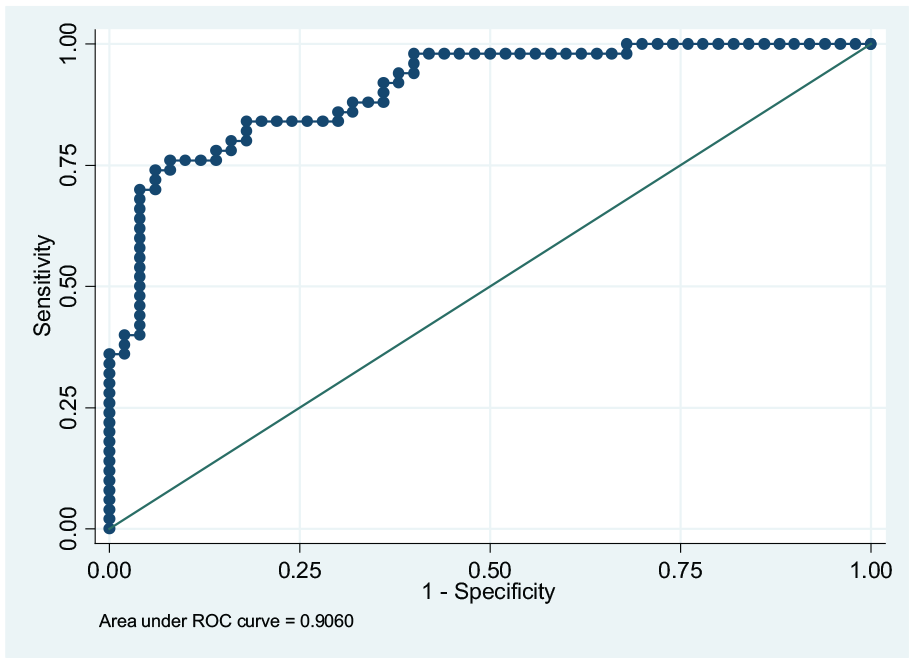
The area under the curve for variables entered in multivariable logistic regression model.
Discussion
This case–control study was designed to determine the relationship between existence of a person with type 1 diabetes with quality of life and depression in their family caregivers in Semnan city (diabetes caregivers = 50 family caregivers of people with type versus non-diabetes caregivers = 50 family caregivers of people with non-type 1 diabetes). The multivariable logistic regression model showed a significant association between existence of a patient with type 1 diabetes with number of caregivers’ children (OR = 1.77; 95% CI: 1.06–2.94), quality of life (OR = 0.82; 95% CI: 0.74–0.90), sex (OR = 10.04; 95% CI: 2.29–43.99), and income level of caregivers (OR = 6.49; 95% CI: 1.35–31.08); however, it did not show a significant relationship with depression (OR = 1.02; 95% CI: 0.94–1.10).
In our study, the quality of life of family caregivers of type 1 diabetic patients was significantly lower than the quality of life of non-diabetes caregivers, which was in line with the results of similar studies. In the study by Golfenshtein et al., aimed to examine the level of stress and quality of life of parents of children with chronic diseases, all parents were affected by stress and the consequent decline in quality of life. Also, this stress was experienced in parents with children with chronic diseases with more intensity and duration, which can expose them to physical and psychological damage, reduced quality of life and inappropriate parenting behaviors. 21 In general, the management of type 1 diabetes requires a series of intensive daily tasks that can affect all aspects of the patient’s life (including eating, sleeping, playing, going to school), especially if he (she) is a child. These tasks often conflict with the patient’s wishes and make him or her resist family caregiver requests for dietary compliance, daily blood sugar monitoring, and insulin injections. As a result, family caregivers of type 1 diabetics often face more challenges, and parents with type 1 diabetes appear to experience more stress and, as a result, a lower quality of life than parents of normal children.22,23 In addition, the results of a number of similar studies have shown that the reason for the decline in the quality of family caregivers of people with chronic diseases is a disorder in the mental health of family caregivers of these patients. 24 Quality of life is a mental and dynamic concept, the high level of stress in family caregivers of patients with type 1 diabetes, which is associated with the management of the patient’s diabetes and the resulting problems, causes them to experience negative and unpleasant emotions that ultimately leads to lower quality of life and mental health in the caregivers. 25 Also, the existence of family conflicts in the management of diabetes is another reason for mental disorders and, as a result, the low quality of life of families with patients with type 1 diabetes. These conflicts destroy family cohesion and lead to a reduction in the quality of life in the family and disrupt the performance of disease-related tasks. Therefore, providing training programs for stress management and improving the quality of life of family caregivers of people with type 1 diabetes seems necessary.26,27 Family caregivers report a very narrow range between high and low blood sugar, which is very difficult to move in. If they cannot maintain a balanced blood sugar level, they feel guilty, which also affects the quality of life of family caregivers. Patients with type 1 diabetes have a negative effect. 28
Various studies in the United States have shown that the quality of life of both patients and caregivers is inversely related to poor glycemic control, complications and diabetes, and comorbidities. 29 Another study by Julio Lopez-Bastida et al. aimed at assessing the quality of life in type 1 diabetic patients and family caregivers in Spain found the quality of life in both patients and their caregivers was associated with complications and HbA1c levels so that patients with fewer complications, comorbidities, and controlled HbA1c levels had higher quality of life scores. 30 The study of Einar B. Thorsteinsso et al. aimed to compare the perceived quality of life in two groups of mothers of children with diabetes and mothers of children without diabetes showed the mothers of children with diabetes type 1 had a lower quality of life than mothers without children. Self-efficacy, relationship satisfaction, and social support were also the most important factors affecting the quality of life of these mothers. 31
Generally, diagnosis of type 1 diabetes has significant effects on families in addition to the patient. The management of diabetes places substantial demands on families. Diabetes can have negative effects on the development of complications, psychological status, and personal, family, and social relationships. The nature of diabetes in terms of treatment and care on the one hand and the effect on employment and absenteeism on the other hand, according to the burden of the disease and its costs, can be related to the low economic level.32,33
Caregivers family are under a lot of daily stress because they have to manage the behavior and factors related to the health of their sick (monitoring patient’s mobility, dietary restrictions, regular blood sugar control, regular checking for signs of hypoglycemia, and hyperglycemia) with greater precision and sensitivity than before the disease.34,35 Therefore, it is necessary for these caregivers to have access to a network of social support (such as emotional and financial) and psychological to manage the stress and strain caused by this disease.
These studies have a number of strengths and limitations. One of the strengths of this study compared to other studies is having a control group and doing it with a case–control design. The second strength is the study of depression in caregivers in addition to quality of life. The first limitation is the study design, it is difficult to examine the causal relationship because the two variables are examined simultaneously and is unclear which one occurred before the other, in other words, the assumption of temporality is not considered; therefore, we need prospective cohort studies to overcome this limitation. The second limitation is the small sample size. Finally, factors such as genetics, nutrition, physical activity, home environment physically and mentally, etc. may have affected the quality of life of caregivers family, which have not been studied in this study.
Conclusions
The quality of life in family caregivers of type 1 diabetics is low and gender, income level, and number of caregivers’ children were the most important factors predicting it. Therefore, psychological interventions (such as psychological counseling) to manage stress and improve the quality of life of family caregivers is recommended.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221146055 – Supplemental material for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study
Supplemental material, sj-docx-1-smo-10.1177_20503121221146055 for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study by Raheb Ghorbani, Majid Foroutan, Seyed Saeed Kassaeian, Naim Sadat Kia, Babak Gholizade Bajandi, Alireza Haji Ghanbari and Elahe Ghods in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221146055 – Supplemental material for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study
Supplemental material, sj-docx-2-smo-10.1177_20503121221146055 for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study by Raheb Ghorbani, Majid Foroutan, Seyed Saeed Kassaeian, Naim Sadat Kia, Babak Gholizade Bajandi, Alireza Haji Ghanbari and Elahe Ghods in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121221146055 – Supplemental material for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study
Supplemental material, sj-docx-3-smo-10.1177_20503121221146055 for Evaluation of quality of life and depression in family caregivers of patients with type 1 diabetes in Iran: A case–control study by Raheb Ghorbani, Majid Foroutan, Seyed Saeed Kassaeian, Naim Sadat Kia, Babak Gholizade Bajandi, Alireza Haji Ghanbari and Elahe Ghods in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the staff of the endocrinology clinic of Kosar Hospital of Semnan for their cooperation in conducting this research.
Author Contributions
RGH and EGH designed the study. MF and SSK supervised the study. BGHB and AHGH processed the data. RGH did the statistical analysis. NSK and EGH interpreted the results. EGH , EGH , MF , SSK wrote the original draft. NSK and EGH review and edit the final draft. All authors have read and approve the final manuscript.
Availability of data and material
Access to the data of this study is not restricted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was performed according to the principles expressed in the Declaration of Helsinki and was approved by the Deputy of Research and Ethics Committee of Semnan University of Medical Sciences (Iran) (ID: SEMUMS.REC.139288).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Deputy of Research of Semnan University of Medical Sciences, Semnan, Iran.
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from the caregivers and patients before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.