
Abstract
Our objective was to evaluate the accuracy of risk stratification criteria for febrile neonates in the emergency department. This was a retrospective study of febrile neonates ≤56 days of age. Patients were low risk for serious bacterial infection (SBI) if all test results were within normal ranges. Three hundred thirty-eight patients were enrolled with a mean age of 32 (±14) days, and 78 (23%) had SBI: 26 (8%) with bacteremia, 48 (14%) with urinary tract infection, 3 (1%) with meningitis, and 11 (3%) with pneumonia. Risk stratification criteria identified 47 (14%) as low risk, 2 of whom had SBI (both with Group B Streptococcus bacteremia). The sensitivity was 97.4% (95% confidence interval = 91.0% to 99.7%), and the negative predictive value was 95.7% (95% confidence interval = 84.8% to 98.9%). The risk stratification criteria have high sensitivity and high negative predictive value for identifying infants at low risk for SBI. Care must be taken to assure reliable follow-up.
Introduction
With an estimated 1.4 million neonatal deaths each year attributed to invasive infections, 1 and up to 10% of infants less than 2 months of age with fever having serious bacterial infection (SBI), 2 diagnosis and rapid treatment of SBI in febrile infants is critical in the emergency department (ED). Over the past 2 decades, the microbial agents causing SBI in febrile neonates have been changing, with decreasing rates of Group B Streptococcus (GBS) and Listeria monocytogenes and increasing rates of Escherichia coli.3-5
Most evidence-based protocols recommend an evaluation for sepsis including examination of blood, urine, and cerebrospinal fluid (CSF) for all febrile infants 28 days of age or less and for all ill-appearing febrile infants between 29 and 56 days of age to evaluate for SBI, as well as administration of empiric antibiotics. For well-appearing febrile infants between 1 and 2 months of age without a source of infection on physical examination, criteria to identify infants at low risk for SBI have been developed.6-8 Utilizing the white blood cell (WBC) count, band count, urinalysis, CSF cell counts, chest X-ray, and stool smear, these criteria have been found to have good sensitivity (92% to 98%) and negative predictive value (NPV; 99% to 100%) in identifying low-risk infants who can be safely discharged from the ED without antibiotic treatment.6,8,9 Most hospitals have established protocols for infants 1 to 2 months of age based on these criteria, 10 and there does not appear to be significant differences in diagnosis or clinical outcomes associated with variations in hospital protocols.11,12 However, the epidemiology of SBI in infants is changing, and different organisms elicit different inflammatory responses, 13 which may change the usefulness of some of the elements of the stratification criteria such as the WBC count.
The purpose of our study was to determine if the risk stratification protocol used at our institution to identify SBI in febrile infants ≤56 days of age, based on previous evidence-based guidelines, remains accurate for identifying all cases of SBI in febrile neonates in the setting of the changing epidemiology of neonatal SBI.
Materials and Methods
This was a retrospective study of febrile neonates 56 days of age or younger who presented to 1 of 3 EDs (1 pediatric and 2 general EDs) of a larger medical center system from January 2012 to December 2014. Patients were included in the study if they had a temperature ≥38°C rectal in the ED or documented within the 24 hours prior to arrival. The medical records of identified patients were reviewed and data were extracted from the electronic medical record utilized in all 3 EDs.
Each patient’s documented ED visit was reviewed for history, physical examination, laboratory, and radiological data. Patient disposition (admit to hospital or discharge home) and return to the ED within 3 days of the initial visit was recorded. The final diagnosis for the patient based on ED and/or hospital discharge diagnoses and laboratory results was documented.
Risk Stratification Protocol
The protocol at our institution was for all infants ≤28 days and ill-appearing infants 29 to 56 days of age to have blood, urine, and CSF studies and to be admitted for empiric antibiotic treatment. For well-appearing infants between 29 and 56 days of age, we used a stratification management strategy to identify those at low risk for SBI, and it included assessment with complete blood count with manual differential, blood culture, urinalysis, urine culture, CSF cell counts and culture (if indicated), glucose levels, liver function tests, chest X-ray for respiratory symptoms, and stool smear and culture for diarrhea. A patient 29 to 56 days of age with a reliable caregiver and follow-up available could be managed as an outpatient if he/she met the following low-risk criteria: WBC count between 5000 and 15 000/µL, manual differential of immature: total neutrophil ratio of <0.2, urinalysis with <10 WBC/high-power field, normal glucose and liver function tests, normal CSF (if obtained), negative chest X-ray (if obtained), and negative fecal leukocytes (if obtained).
Study Definitions
Serious bacterial infection was defined as bacterial growth of a known pathogen with >1000 colony-forming units/mL in blood, urine, CSF, or stool cultures. Contaminated cultures were defined as cultures with bacteria isolated that are not pathogens; a pediatric infectious disease specialist determined whether questionable isolated organisms were true pathogens or contaminants.
In order to evaluate our screening guidelines, patients were considered not low risk or low risk for SBI. Patients were considered not low risk for SBI if they had any laboratory value outside the defined normal ranges, evidence of bacterial infection on physical examination, grossly bloody CSF that was uninterpretable, or incomplete workup at the time of the ED visit. All other patients who had all normal laboratory values were considered low risk for SBI.
Data Analysis
Data were analyzed with SPSS Statistics (IBM, Armonk, NY). Descriptive statistical analyses, including mean and standard deviation (SD), were used for continuous data, and frequencies were used for categorical data. Test performance characteristics, including sensitivity and negative predictive value, were calculated. Two-sample t tests were used to compare means for continuous data between 2 groups with a significance of 0.05.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Montefiore Medical Center (Reference # 002539).
Results
The charts of 338 patients who presented to the ED with fever were analyzed. Two hundred sixty-three (78%) patients were evaluated in the pediatric ED, and 75 (22%) were evaluated in the 2 general EDs. Demographic information and disposition of the study population are included in Table 1.
Demographic Information and Disposition, N = 338.

Abbreviations: PED, pediatric emergency department; GED, general emergency department; SD, standard deviation; SBI, serious bacterial infection.
Seventy-eight patients (23%) were found to have SBI, including 39 with urinary tract infection, 17 with bacteremia, 11 with pneumonia, 9 with urosepsis, and 3 with bacterial meningitis (one patient had E coli bacteremia and E coli meningitis). Of the 77 positive cultures, E coli bacteriuria was the predominate cause of infection, with 39 (51%) cases, followed by GBS bacteremia with 9 (12%) cases and E coli bacteremia with 8 (10%) cases (Table 2).
SBI by Source of Infection and Microbiology.

Abbreviations: SBI, serious bacterial infection; CSF, cerebrospinal fluid; GBS, Group B Streptococcus; MSSA, methicillin-sensitive Staphylococcus aureus.
Three urine cultures were positive for >1 pathogen.
The risk stratification results versus SBI and test performance characteristics for all 338 patients are shown in Table 3. Overall, of the 78 cases of SBI in the study population, 76 were correctly identified as not low risk, with a sensitivity of 97.4% (95% confidence interval = 91.0% to 99.7%). Of the 47 infants identified as low risk, 45 did not have SBI, with a NPV of 95.7% (95% confidence interval = 84.8% to 98.9%). All 30 febrile neonates 28 days of age or less with SBI were correctly identified as not low risk.
Risk Stratification Results Versus SBI and Test Performance Characteristics With 95% Confidence Intervals a .
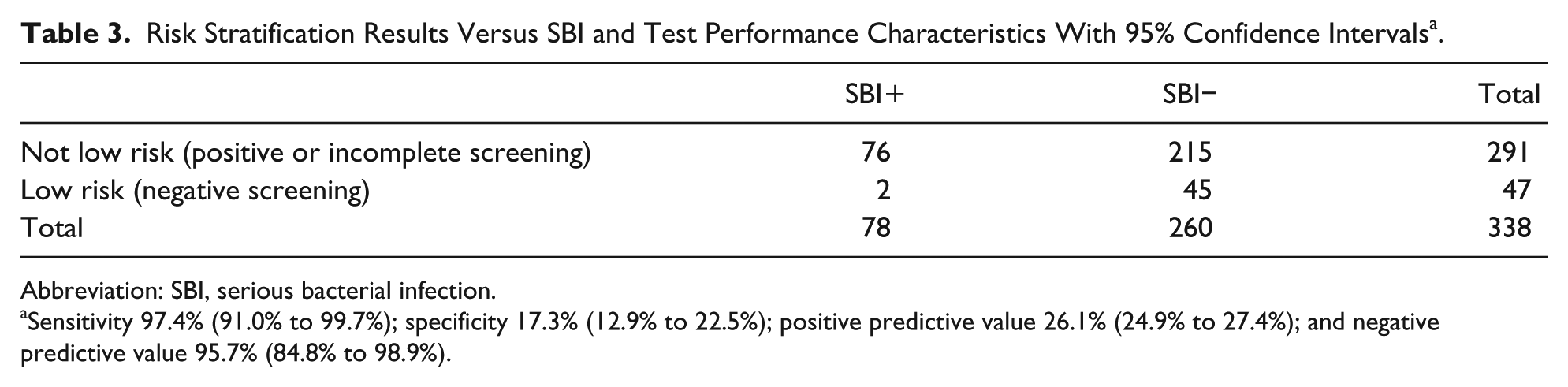
Abbreviation: SBI, serious bacterial infection.
Sensitivity 97.4% (91.0% to 99.7%); specificity 17.3% (12.9% to 22.5%); positive predictive value 26.1% (24.9% to 27.4%); and negative predictive value 95.7% (84.8% to 98.9%).
There were 2 infants identified as low risk that were found to have SBI, and both patients had blood cultures positive for GBS. The first patient was a 47-day-old ex-40-week female with fever for 6 hours prior to arrival, while the second patient was a 50-day-old ex-36-week female with fever for 7 hours prior to arrival, and both infants were recalled, admitted, and treated after blood cultures became positive. Both patients had no progression of symptoms on reevaluation and an uneventful recovery.
One hundred fourteen patients had incomplete evaluations in the ED. Ninety-two (81%) did not have a manual differential performed and therefore could not have an immature–total neutrophil ratio calculated. Eleven (10%) were 28 days or younger and did not have a lumbar puncture performed. Six (5%) did not have a manual differential and were 28 days or younger and did not have a lumbar puncture. Five (4%) did not have a urinalysis obtained.
The mean WBC count overall was 11.9 (SD = 5.1). The mean WBC count for patients with cultures positive for E coli was 14.7 (SD = 5.8), and the mean WBC count for patients with cultures positive for GBS was 11.6 (SD = 5.3). There was no significant difference between the mean WBC count of patients with E coli and GBS infection (P = NS).
Discussion
It is critical for emergency clinicians not to miss the diagnosis of SBI in neonates due to the significant potential morbidity and mortality associated with untreated SBI. Up to 10% of febrile infants less than 2 months of age will have SBI, with about 3% having bacteremia or meningitis. 2 For febrile infants less than 1 month of age, there may be a higher incidence of SBI, with up to 20% of infants 28 days of age or younger having infection. 11 In our study, the incidence of SBI was 23% overall, with 30/143 (21%) in infants 28 days of age or younger and 48/195 (25%) in infants 29 to 56 days of age.
Febrile neonates may not be managed according to established standards of care or institutional clinical practice guidelines. In one study, one third of pediatric EDs did not have clinical practice guidelines for the evaluation and management of febrile infants less than 2 months of age. 10 For infants ≤28 days with fever, recommended management for complete evaluation with blood, urine, and CSF studies is not followed in 28% to 33%.11,14 In our study, 114 (34%) febrile infants had incomplete evaluations according to our protocol, due to not having a manual differential performed, a lumbar puncture not performed on a patient under 1 month of age, or a urinalysis not obtained. In the ideal setting, all tests would be obtained; however, in practice, it may not be possible to have every test completed on every patient. At the time of this study, our institution’s laboratory did not routinely perform manual differentials on all patients 56 days of age or younger. In addition, in some cases, not enough urine was obtained from a catheterized specimen for a complete urinalysis, and only a culture or urine dipstick was obtained. In this study, we considered patients with incomplete evaluations to be not low risk for SBI.
Based on the low-risk criteria strategies and general consensus for identifying SBI in febrile neonates, for well-appearing febrile infants, a WBC count <15 000 is required to be considered low risk. 15 However, evidence suggests that WBC is not sufficiently accurate for identification of SBI in children, with low sensitivity for diagnosis of neonatal sepsis 16 and for SBI. 17 Moreover, different pathogens may cause varying immune and inflammatory responses. 13 As such, some pathogens may not cause an elevated WBC count or may not elevate the WBC count to the same extent as others, leading to a potentially missed SBI diagnosis based on current screening guidelines. Our study showed a higher WBC for E coli infections than for GBS infections that was not statistically significant. However, our 2 missed cases of SBI were both GBS bacteremia. As there were relatively low numbers of GBS and E coli infections in our study, more research is needed to investigate this question.
Additionally, the bacteriology of microbial agents causing neonatal SBI in febrile neonates has been changing over the past 2 decades, with decreasing rates of GBS and Listeria and increasing rates of E coli and other gram-negative infections.3-5,16 In accordance with current literature, our study demonstrated that E coli is indeed the most common pathogen causing SBI in this age group, causing 47 cases of urinary tract infection, bacteremia, and meningitis. GBS was the second most common pathogen, with 13 positive cultures in blood, urine, and CSF. Both infants with SBI not identified as low risk by our protocol had GBS bacteremia.
The 2 missed cases of GBS bacteremia in our study were infants 47 and 50 days old with fever for 6 to 7 hours prior to arrival to the ED. These were well-appearing infants who had complete workups done in the ED and were discharged home as they were categorized as low risk. Both were recalled, reevaluated promptly without further progression of disease, and treated without further sequelae.
Our sensitivity of 97.4% and NPV of 95.7% are similar to previous studies, with other sources citing sensitivity of 92% to 98% and NPV of 99% to 100%.6,8 We believe that our current protocol, established with current evidence, remains accurate to identify neonates at low risk for SBI.
Our study had several limitations. First, this was a retrospective chart review, limited by the data that were recorded in the medical record. However, using objective data from laboratory results minimizes this limitation, allowing for an objective diagnosis of SBI. Another potential limitation of our study was the relatively small sample size, with a total of 338 patient charts reviewed. However, we included data over 3 years taken from 3 EDs with similar populations of patients, and our incidence of SBI and the sensitivity and NPV of febrile infants at low risk for SBI is similar to that documented in the literature, indicating that our patient population is likely a representative sample.
Conclusions
Escherichia coli was the most common pathogen causing SBI in infants up to 56 days of age, followed by GBS. The current risk stratification criteria used by our institution remain useful as our criteria have both high sensitivity and NPV for identifying infants 29 to 56 days of age at low risk for SBI. Our risk stratification criteria correctly identified all infants less than 28 days of age with SBI; however, 2 infants greater than 28 days of age with SBI were missed, although they both received treatment and recovered uneventfully. Therefore, while the current risk stratification criteria serve a useful tool in the management of febrile infants presenting to the ED, care must be taken to assure reliable follow-up.
Footnotes
Author Contributions
Joni Rabiner contributed to conception and design, data analysis and interpretation, and drafted and critically revised the manuscript.
Maya Capua contributed to conception and design, contributed to acquisition, analysis, and interpretation of data, and drafted the manuscript.
Dina Golfeiz contributed to acquisition of data, analysis, and interpretation of data, and drafted the manuscript.
Jamie Shoag contributed to acquisition of data.
Jeffrey Avner contributed to conception and design, data analysis and interpretation, and critically revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.