
Abstract
Non-identification of serious bacterial infection (SBI) in febrile infants is a common occurrence in clinical practice, culminating in catastrophic presentations. Six infants who initially presented to the clinician with fever without a focus, and were lately diagnosed with bacterial meningitis were analyzed for clinician-related factors contributing to the non-identification of meningitis. In a febrile neonate and a febrile young infant, lack of comprehensive evaluation was contributing to the non-identification of SBI; in four infants above the age of 3 months, meningitis was missed in spite of clinicians practicing treatment guidelines. Inadequate symptom characterization in two febrile infants and inappropriate interpretation of hemogram in three febrile infants also contributed to the non-identification of meningitis. Except for one, all infants developed complications. We conclude that the characterization of clinical features of SBI-like meningitis, interpretation of lab data, and adherence to the treatment guidelines are crucial in the management of an infant presenting as fever without a focus.
Keywords
Introduction
Fever is one of the commonest causes of outpatient and emergency room visits in children. Among young children with fever, 5%–10% have a serious bacterial infection (SBI) like meningitis, urinary tract infection, pneumonia, or bacteremia. 1 Delayed identification of SBI-like meningitis in febrile children is a common occurrence in clinical medicine which usually culminates in catastrophic presentations in tertiary centers. There are not many studies on factors contributing to the delayed diagnosis of bacterial meningitis in children, especially those who present with fever without a focus. During the clinical discussions, we noted that in many infants with complicated SBI-like meningitis, the diagnosis was missed during the initial consultations. We selected infants with meningitis who were presenting to the physician initially, as fever without a focus. There were six such infants over a period of 6 months in 2022. We collected the details regarding the symptomatology and immunization status from the parents. The documented clinical features, lab data, and prescription patterns during the initial consultations were collected from the prescriptions and lab reports. Subsequently, we tried to find out the factors contributing to the delay in the identification of meningitis in these babies, by analyzing the extent of clinician adherence to the various components of existing management guidelines of fever without a focus in children.2,3 Our institution follows Indian Academy of Pediatrics guidelines which recommends the following management for well-appearing infants presenting as fever without a focus. (i) In well, as well as sick babies ⩽28 days of age, hospitalization and comprehensive evaluation including a cerebrospinal fluid (CSF) study, (ii) in infants between 30 and 90 days, perform a complete blood count (CBC), C-reactive protein (CRP), urinalysis, urine, and blood cultures, with chest X-ray if the total count (TC) is >20,000/µL and lumbar puncture only selectively, and (iii) in infants >90 days, perform a CBC, CRP, urinalysis, urine culture, and blood culture with no mandatory CSF study. 2 Written informed consents were obtained from the parents for publishing the data and institutional ethics committee clearance was obtained accordingly (Ref. No. GMCKKD/RP/2022/IEC/63).
Case 1
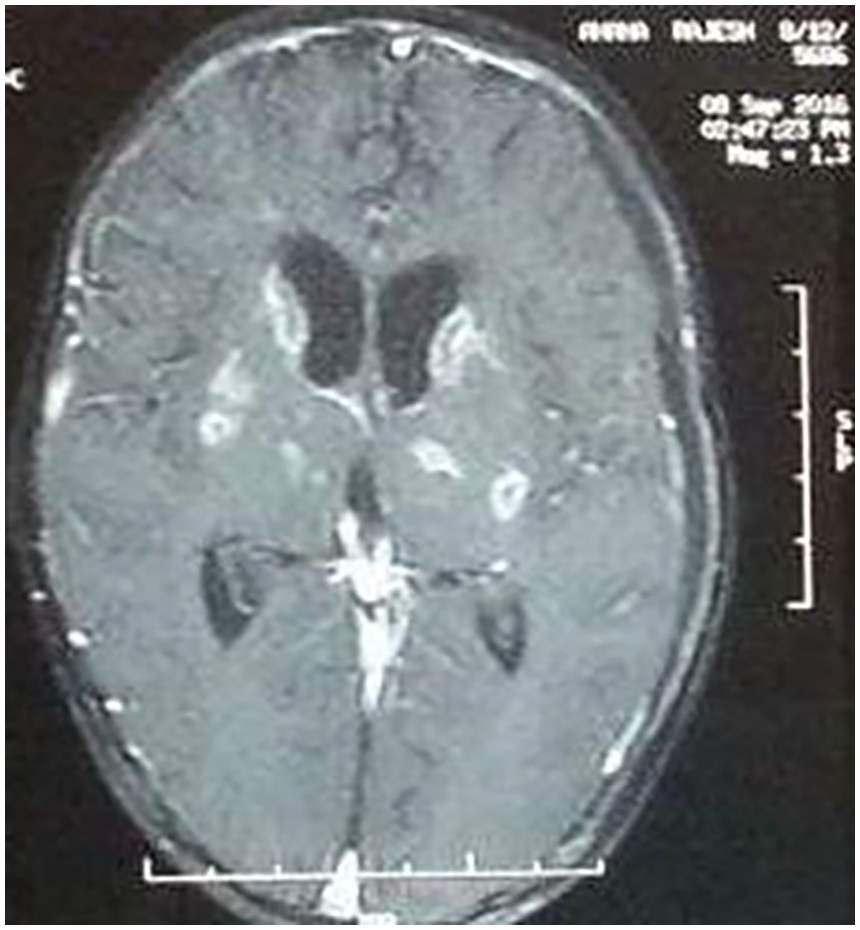
A term female baby from an upper-middle-class family with a 3.6 kg birth weight consulted to a pediatrician in a corporate hospital on the 10th day of life for fever (102.2°F). The pediatrician documented an active baby having no focus of infection. The TC was 19.6 × 109/L with polymorpho-nuclear leukocytes at 54% and lymphocytes at 40%. An oral antibiotic was prescribed and sent home. After 3 days, the baby was admitted to our institution with vomiting, lethargy, seizure, bulging anterior fontanel, suture separation, and papilledema. CSF study confirmed meningitis and the baby developed communicating hydrocephalus with bilateral subdural effusions (Figure 1) requiring 6 weeks of antibiotic therapy. No pathogen was isolated from blood or CSF.

Showing hydrocephalus and subdural collections in case 1.
Case 2
Five-month-old unimmunized male baby from an upper-middle-class family visited a pediatrician at his office practice for an abrupt onset of high-grade fever with rigor. The clinician documented the baby as active and feeding well and sent home on oral co-amoxiclav. The fever was not documented and no investigations were performed. On the third day, the baby developed poor feeding, ecchymosis, seizure, unconsciousness, and shock, and expired within an hour of reaching the hospital. On analyzing the history, the mother said that the baby’s activities and sensorium were normal during initial consultation. Post-mortem CSF study with consent showed pleocytosis with 88% polymorphs, non-detectable sugar, 155 mg/dL protein, and plenty of gram-positive diplococci.
Case 3
Three-month-old female baby, unimmunized against pneumococci belonging to a lower-middle-class family, consulted a pediatrician in an urban area at his office practice for high-grade fever (103.8°F). Baby was assessed as well appearing and sent home on oral co-amoxiclav without any investigations. Fever persisted, developed irritability and seizure by the fourth day, and was admitted to our center in a sick, drowsy state. CSF showed meningitis and the baby responded to 2 weeks of treatment with ceftriaxone and vancomycin without developing any early complications. No pathogen was isolated from blood or CSF.
Case 4
Eight-month-old female baby unimmunized against pneumococci belonging to a lower-middle-class family consulted a clinician at his clinic for high fever which was not documented. He prescribed oral antibiotics after documenting the baby as active alert (later during our evaluation obtained a history of irritability and listlessness). As the symptoms persisted, the parents consulted a pediatrician in a hospital who prescribed another oral antibiotic and sent home. During both occasions no investigations were performed. On the fourth day of illness, the baby was admitted to our institution with persisting seizures and diagnosed with meningitis with communicating hydrocephalus. Blood and CSF cultures were sterile; tuberculous meningitis workup was negative. Baby required 3 months of hospitalization and was in a vegetative state at the time of discharge.
Case 5
Eight-month-old unimmunized female infant from a lower-middle-class family was evaluated in the emergency room of our institution for a high fever of 104.4°F and rigor. The resident doctor documented an active alert baby and normal anterior fontanel. The TC was 13.2 × 109/L, polymorphs 64%, lymphocytes 31%, erythrocyte sedimentation rate (ESR) 90 mm/first hour, and CRP 22 mg/dL. Baby was sent home on antipyretic. The resident doctor who was posted in the emergency room on the second month of his joining course, failed to discuss the case with the senior resident before sending the patient home. Two days later, got admitted for persisting fever and multiple seizures. The CSF showed meningitis and yielded salmonella typhimurium growth from the CSF and blood. Contrast enhanced computed tomography (CECT) scan showed ring-enhancing lesions and hydrocephalus (Figure 2). Baby required 4 weeks of antibiotics but developed right hemiplegia as sequelae.
Showing ring-enhancing lesions with hydrocephalus in case 5.
Case 6
Ten-month-old male baby from an upper-middle-class family unimmunized against pneumococci consulted a physician at his clinic for high fever who prescribed oral antibiotics without any lab investigations. The fever was not documented. A normal sensorium was documented at that time (later during the interview, mother gave a history of baby having irritability and reduced activity). Next day consulted a pediatrician as symptoms persisted, who did blood tests which showed a TC 14.9 × 109/L, neutrophils 70%, lymphocytes 28%, and CRP 39 mg/dL. Following this, the baby was treated with intramuscular ceftriaxone on an ambulatory basis without performing any further investigations or procedures. No documentation of clinical features was noted. As the fever persisted and irritability worsened baby was hospitalized at our center and diagnosed with meningitis. No pathogen was grown in CSF or blood and tuberculous meningitis workup was negative. Baby was treated with 3 weeks of antibiotics but developed hydrocephalus, spastic quadriplegia, deafness, and visual impairment.
Discussion
In this series, all febrile infants with SBI were having bacterial meningitis; except one, all had complications and one baby expired. We found many variations in the clinician practice during the management of infants presenting as fever without a focus, regarding the comprehensive evaluation, performing a CSF study, characterization of clinical features, and interpretation of hemogram, leading to non-identification of meningitis. There are many studies addressing missed diagnosis and delayed diagnosis of meningitis in children4,5 and many of them were looking at demographic and disease-related factors. In a retrospective study conducted in children >2 months of age with bacterial meningitis, initial presentation to an outpatient clinic, preceding or coincident illness, and language barrier were the factors contributing to the delayed diagnosis and more than 8 hours was the cut-off for delayed diagnosis. 5 In another study with 2 hours being the cut-off for delay, there was a prevalence of 61% delayed diagnosis and, comorbidities, suspicion of infection other than meningitis as well as other diagnoses were associated with a delayed diagnosis. 6 In contrast to these, our study looked at the factors related to clinician practices and healthcare delivery system. To our knowledge, no such study has been conducted in India. The delay in the diagnosis we observed was between 2 and 4 days.
On five occasions, that is, 3-month, 5-month, 8-month (by two clinicians), and 10-month infants who presented with fever without a focus were treated with oral antibiotics without a mandatory comprehensive lab evaluation as recommended by the guidelines, 2 precipitating the delayed identification. Even though all the guidelines recommend hospitalization and comprehensive/selective evaluation like lumbar puncture in febrile infants <3 months, marked variation in practice among clinicians has been reported.7–9 The socioeconomic conditions of the patients and the infrastructure at the point of care were in favor of optimum evaluation in all these occasions we analyzed; the lack of awareness seems the contributing factor in the above-mentioned practices.
In well-appearing febrile children >3 months, the Indian Academy of Pediatrics and the American Academy of Family Physicians recommend partial or selective evaluation by using blood culture and urine investigations; a CSF study is not recommended unless there are neurologic signs.2,3 These recommendations are formulated based on the decline in the incidence of central nervous system infections following the introduction of vaccination against Hib and pneumococcal infections. 2 The 5- and 8-month-old infants who were bacteriologically diagnosed as salmonella typhimurium and pneumococci meningitis were unimmunized, and both were documented as well appearing during the initial consultations. Though the clinicians were following the existing guidelines, meningitis was missed. This suggests that, in the context of suboptimal vaccination coverage against pneumococci as well as reports of uncommon pathogens such as Salmonella spp. causing invasive infections in immuno-competent children,10,11 practicing a selective evaluation in well-appearing febrile infants >3 months can lead to non-identification of SBI-like meningitis. Moreover, as there are no separate recommendations for the management of unimmunized febrile infants in the existing guidelines, our report of pneumococcal meningitis in an unimmunized infant is relevant—highlighting the importance of assessing the immunization status against pneumococcal infections during the management of febrile infants.
Two infants above the age of 3 months (8 and 10 months) were managed as well-appearing febrile babies; accordingly, a CSF study was not performed on them. But on reviewing the history we found that both the babies had poor activity and persistent irritability. The advantage of symptom characterization possible in older infants is one of the rationales for recommending selective CSF study in febrile children above 3 months of age. 2 Our observations throw light on the fact that the characterization of symptoms and signs may not be possible uniformly when the clinical features become nonspecific as in infants with meningitis. The importance of characterization of clinical features needs to be highlighted in the medical curriculum. The data on how early a child with meningitis develops specific symptoms like seizures is varying; Chang et al. reported the interval between onset of meningitis and seizure as 1–20 days with a mean of 4 days 12 whereas, Ataei Nakhaei et al. showed 34.3% of children having a seizure before the hospitalization and 77.6% developing seizure before third day of the illness. 13
During the initial consultations of the newborn, 8- and 10-month-old babies, the clinicians did not consider SBI after interpreting the CBC reports, which were suggestive of bacterial infection. Various factors can affect the characterization of lab results in clinical practice. The lack of awareness among clinicians about the characteristics of various screening tools, especially the discriminative role of simple tests such as hemogram for identifying SBI has been highlighted by Mahajan et al. 2
In this case series, all the patients were belonging to the middle-class family and initial evaluation of febrile infants was carried out by clinicians representing different categories of healthcare delivery systems like corporate hospitals (newborns), office practice (patients 3 and 8 months), small hospitals (8 and 10 months) as well as medical college (8 months), and non-identification of meningitis in infants presenting as fever without a focus occurs in all categories of healthcare delivery systems.
The limitations of the study are (i) many of the data were collected by retrospectively reviewing the history and prescriptions, which might be less accurate and (ii) we couldn’t include the follow-up data on the evolution of clinical and neuroimaging findings.
Conclusions
Characterization of clinical features of SBI-like meningitis, interpretation of hemogram, and adherence to the treatment guidelines are crucial in the management of infants presenting as fever without a focus; the medical education system needs to be prioritized accordingly.
Footnotes
Acknowledgements
We thank Dr. Ajithkumar VT, HOD Pediatrics, Dr. MG Geeta, Dr. Mohandas Nair, Dr. Ashraf TP, and Geetha P for the support provided to complete the study.
Author contributions
K.C. conceptualized the study and drafted the manuscript. P.R.S.A. and M.D.F. collected the materials and managed the cases. M.S.V.K. managed the cases and assisted in drafting the manuscript. M.P.J. critically analyzed the study and revised the manuscript. All the authors approved the manuscript. K.C. will act as the guarantor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for participation
Obtained.
Consent for publication
Obtained.
Ethics approval
Institutional ethics committee clearance taken. Ethical approval to report this case series was obtained from Government Medical College Kozhikode. (Ref. No. GMCKKD/RP/2022/IEC/63).
Informed consent
We confirm that the necessary consent for publishing the information about the patient’s details has been obtained from the parents of the babies included in this study.