
Abstract
Background
Malaria infection remains one of the major global and national public health threats, affecting millions of people yearly by causing substantial morbidity and mortality. In developing countries, higher proportions of poor malaria prevention and control measure both regionally and nationally, particularly in pastoral community areas of southern Ethiopia.
Objective
The study aimed to assess malaria preventive practices and associated factors among households of pastoral communities in Borena zone, Oromia regional state, Southern Ethiopia, 2022.
Methodology
A community-based cross-sectional study design was used from March first to 30, 2022, among 421 selected simple random sampling households in pastoral communities of the Borena zone. Data were collected through face-to-face interviews with a structured pretested questionnaire and visual observation for household malaria prevention practices. Then, the data were analyzed using SPSS version 25. Bivariate and multivariable logistic regression analyses were used to identify factors associated with malaria preventive practices. Finally, adjusted odd ratio (AOR) together with 95% confidence intervals was used, and a P value of less than 0.05 indicated an overall statistical association.
Result
The overall malaria prevention rate among pastoral community households was 31.6%(133) [95%; CI = 27.2–36.4]. The factors significantly associated with malaria prevention practice were malaria prevention knowledge [AOR = 1.6, 95% CI = 1.1–2.5] and the absence of plasmodium parasites among children [AOR = 4.3, 95% CI = 2.8–8.7]. However, households staying outdoors at night [AOR = 0.5, 95% CI = 0.3–1.0] were negatively associated with household malaria prevention. A total of 200 (47.5%) households had used insecticide-treated mosquito nets (ITN) and 5(1.2%) households had indoor residual sprays (IRS).
Conclusion
The study revealed lower malaria prevention practices among households of the pastoral community. The government and other concerned bodies should contribute to malaria prevention measures in pastoral remote areas. Health extension workers should have to create awareness in the communities to avoid incorrect use of the ITN.
Background
Malaria is a major infection affecting resource-constrained countries, particularly in tropical regions throughout the world. Ethiopia is one of the countries at a high risk of malaria epidemics due to climate and topography. The climatic fluctuations and drought-related nutritional emergencies cause a broad range of epidemics to occur every 5–8 years in some areas. Plasmodium falciparum and P. vivax are the two predominant species in the country, accounting for 60% and 40% of malaria cases, respectively, transmitted by inoculation of mosquitos (Anopheles species, including Anopheles arabiensis).1–4
Malaria transmission is mostly based on altitude and rainfall, with a lag time varying from a few weeks before the beginning of the rainy season to more than a month after the end of the rainy season. This coincides with the major growing season and harvest time, so malaria diminishes agricultural productivity. Nearly half of the total population living between altitudes of 1500 and 2500 meters above sea level is at risk of epidemic malaria in Ethiopia. 5
The Ethiopian National Malaria Elimination Program (ENMEP) developed a five-year national strategic plan from 2021–2025, intending to attain 100% coverage of the population at risk of malaria with one type of globally recommended vector control intervention by 2021. Toward this, new interventions such as malaria case investigation, classification, and response and malaria foci investigation, classification, and response have been recently started. 6 However, communities such as nomadic pastoralists may constitute an important barrier to malaria elimination efforts in some regions. The mobility of pastoralists and their residence distally from health facilities may challenge malaria control and elimination initiatives that have been initiated nationally. Mobile pastoralists may also reintroduce malaria into malaria-eliminated areas/localities. Pastoral communities are generally marginalized concerning all social services, including health care, and effective malaria control interventions in pastoral communities might have been lacking. 7
The ENMEP launched subnational malaria elimination in 2017 and planned to expand the elimination program to all malarial areas of the country endeavoring to zero indigenous malaria in the country by 2030.
6
However, the movement of malaria parasites by human migration can quickly undermine efforts to suppress or interrupt transmission.
8
On the other hand
Although several interventions have been implemented in Ethiopia, they are ineffective because not based on the local realities and knowledge of factors that affect malaria distribution and malaria preventive practice. 11 Hence, a better understanding of the current household-level preventive practice and its associated factors has paramount importance to scale up and design appropriate interventions in the remotest Ethiopian communities, such as pastoralists, which are vulnerable due to their nature of mobility. Therefore, this study fills this gap by identifying current household prevention practices and associated factors among households in pastoral communities of Borena, South Ethiopia.
Methods and Materials
Study Setting, Study Design, and Period
The community-based cross-sectional study was conducted on pastoral communities of the Borena zone of Oromia Regional State, South Ethiopia, from March first to 30, 2022. The Borena zone has ten districts, bordered by the Somali region to the east, West Guji to the north, Guji to the northeast, Kenya to the south, and the Southern Nation Nationalities People region to the west (Figure 1). . The Borena zone areas are known to be malaria endemic, but transmission is seasonal. Peak transmission is usually reached between February and May and September and November shortly after the large and small rainy seasons, respectively. Regarding health facilities, only 1 general hospital, 4 primary hospitals, and 44 health centers were found in the zone. In terms of the location and altitude of the three selected districts, Guchi district is situated to the southeast part of Yabelo the zonal capital at approximately 242 km and 813 km via Moyale to the south of Addis Ababa. The district is 1104 meters to 1184 meters above sea level. Gomole district is located 42 km north of Yabelo and 525 km south of Addis Ababa. The district is 1150 meters to 1230 meters above sea level, while Moyale is 200 km from the zonal capital and 771 south of Addis Ababa.12, 13

Map of Borena zone study area.
Study Population and Inclusion Criteria
Households randomly selected who had under-five children in selected administrative villages (kebeles) of selected districts in the Borena zone during the study period were included in the study, while households recently immigrated from outside the study area were excluded from the study.
Sample Size Determination
In total, 421 households sample size was calculated using single population proportion formula where the proportion of malaria prevention practice (54.4%) was taken from a previous study conducted in Hawassa, 9 with the assumption of precision or degree of error of 0.05, confidence interval 95%, nonresponse rate was assumed to be 10%.
Sampling Technique and Procedure
Multistage sampling followed by probability proportional allocation to sample size techniques were employed to reach the study participants. First stage three districts (Guchi, Gomole, and Moyale) were lottery methods from the Borena zone. In the second stage, out of 37 pastoralist kebeles in those three districts, 10 were selected using the lottery method. This means that from 18 kebeles in the Guchi district, 5 kebeles, 13 kebeles in Gomole 3 kebeles, and 6 kebeles in Moyale 2 kebeles were selected. Based on the number of households in each kabele, proportional to population size allocation (PPS) was used to allocate the calculated sample size to each Kebele. The study population was households that were residents of pastoral communities in randomly selected kebeles of the Guchi, Gomole, and Moyale districts. An updated kebele-based sampling frame of the households was obtained from the community health workers/Kebele administration office. A simple random sampling method was applied to select 421 households out of 3100 in 10 selected kebeles (Figure 2). The participants of selected households were visited at their homes, informed about the study, and invited to participate. If participants were not at home, the research teams came back a minimum of three times before replacing the non-participating household. One eligible child was selected when there were multiple children under the age of 5 in that household. 9 Children whose parents or guardians declined to give assent were excluded and replaced with those parents/guardians who gave assent. 14

Schematic presentation of the sampling procedure of household preventive practice and associated factors among pastoral communities in Borena zone. HH, households, ** ss, sample size (allocated sample size for each kebeles).
Data Collection Methods
Data Collection Tools and Procedures
The data were collected using pretested standard questionnaires by health extension workers. The questionnaires were initially prepared in English and then translated into the Afaan Oromo language. Data collectors introduced themselves and explained the objective of the study. Additionally, data collectors were given details to the study participants and verbal consent was obtained. Data were collected through face-to-face interviews. Then, a questionnaire was completed to obtain demographic information and associated factors for malaria infection, such as knowledge about malaria, family malaria history, and indoor residual spraying. Factors such as the availability of insecticide-treated mosquito nets, mosquito breeding sites near the house, home material, and design were identified by an observation checklist. 9 Blood samples were obtained through a finger prick using sterile lancets and capillary tubes by the BSc laboratory technologist from the selected child. Prepared thick and thin smears were examined through microscopy according to the National Malaria Diagnosis Guideline (NMG) of malaria guidelines. 15
Operational Definition/Definitions of Terms
Data Quality Control
Laboratory personnel and health extension workers were selected, and training was given on the objective, individual rights, informed consent, and techniques of the data collection for two days by the principal investigator. The questionnaire was translated into the local language during the interview to ensure the consistency of the questions. The questionnaires were evaluated by experts to assess their relevance, and their comments were taken into consideration. Then, 5% of the questionnaire was pretested in a community similar to the study population before beginning the actual data collection process to assess the clarity, understandability, and flow of each question, and the time to complete the questionnaire was assessed. Supervisors and principal investigators discussed the findings of the pretest. Based on the results of the pretest, the questionnaire was modified before the actual data collection. During data collection, the questionnaires were checked each day at the actual data collection time for completeness and consistency by supervisors and the principal investigator. A code was given for the completed questionnaires. Data double entry was performed to make comparisons of two data clerks and resolve if there was some difference. Standardized procedures were strictly followed during blood sample collection, smear storage, transportation, and analytical processes. Positive and negative controls were followed according to the test manual and quality assurance under five.
Data Processing and Analysis
All completed checklists were checked for completeness and consistency, and double data entry was made using Epidata version 3.5.1 software. Then, the data were exported to SPSS version 25 for further analysis. Descriptive statistics such as percentage and frequency were computed, and the mean with standard deviation or median with interquartile range was used to summarize the continuous variables accordingly. Different types of graphs or charts and tables were used to present the data. Bivariate and multivariable logistic regression analyses were used to identify factors associated with prevention measures. The variables in bivariate analysis with a p value less than 0.25 (p < 0.25) were included in multivariable analysis. Multivariable logistic regression was performed to control for potential confounders. The model fitness was checked using the Hosmer-Leme goodness-of-fit test. Finally, the strength of associations between outcome and determinant variables was expressed using adjusted odds ratios (AORs) with 95% confidence intervals, and the significance of associations was declared at a p-value of less than 0.05.
Ethical Approval and Consent to Participate
The ethical approval of this study was reviewed and approved by the Bule Hora University institutional review board (BHU/IRB/14). Official letters were written to the districts. Informed, voluntary, written and signed consent was obtained from study participants. Participation in the study was voluntary, and participants informed themselves of their right to quit/refuse their participation at any stage of the study if they did not want to participate. To ensure participant confidentiality, participants were given a code and then disassociated from their personal information, the questionnaires were anonymous, and were interviewed alone to maintain privacy.
Results
Sociodemographic and Socioeconomic Characteristics
Of the total number of households enrolled in the study, 192 (45.6%) were from Guchi districts, followed by Gomole 125 (29.7%). The children's ages ranged from 6 to 59 months, with a mean (SD) age of 22.6 (± 9.7) months. Out of the study participants, only 30 (7.1%) were able to read and write. Regarding the income of the households, the majority, 240 (57%), received 1001 ETB (19 USD) to 2575 ETB (49 USD). In addition, 56 (13.3%) households were from urban areas, and 223 (53%) mothers were housewives (Table 1).
Sociodemographic and Socioeconomic Characteristics of the Households.

Malaria Knowledge Characteristics of Study Participants
Out of the study participants, more than half 252(59.9%) of study participants knew about malaria disease, the majority 349(82.9%) knew about the signs/symptoms of malaria, and only 129(30.6%) knew the mode of malaria infection transmission. In terms of mosquito prevention measures, nearly half of the study participants knew malaria preventive methods, and the majority 303(72%) knew the uses of ITN (insecticide-treated net) (Table 2).
Study Participants’ Mosquito and Malaria Characteristics Knowledge.

House Conditions and Mosquito Prevention Practices
In the total, only 5 (1.2%) households used indoor residual spraying in the last year, and 200 (47.5%) used ITN in the house. 129 (30.6%) households practiced traditional preventive such as firewood smoke, applying body Vaseline, and sleeping with clothes. Regarding house conditions, the majority (347, 82.4%) of houses were made of thatch roofs, and 317 (75.1%) of houses had holes and crack walls that favored mosquito rest (Table 3).
House Conditions and Mosquito Prevention Measures of the Households in the Study Area.
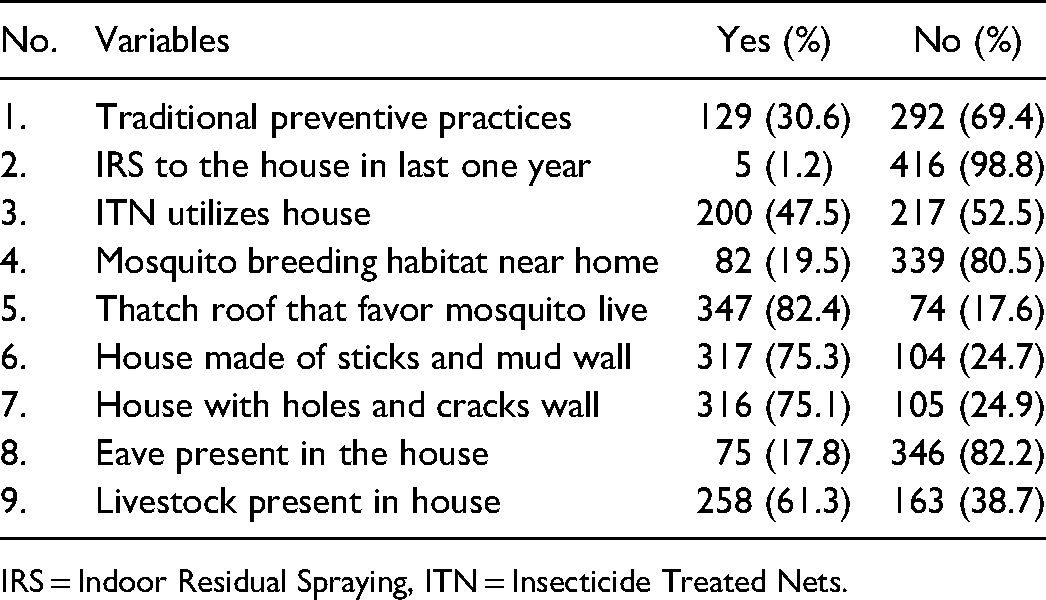
IRS = Indoor Residual Spraying, ITN = Insecticide Treated Nets.
Prevalence of Household Malaria Prevention Practices
The overall malaria prevention practices among household of the Borena pastoral community was 133 (31.6%). The utilization of at least one ITN among houses of pastoral communities was Moyale = 50 (48.1%), Guchi = 81 (42.2%), and Gomole = 69 (55.2%). The IRS to the house within one past year was Moyale = 2 (1.9%), Guchi = 2 (1%), and Gomole = 1 (0.8%) (Figure 3).

ITN and IRS coverage among households in the Borena zone.
Most of the pastoral communities observed misused ITNs (eg, kitchen sheltering, plant protection, thread making, and other purposes), while no single was observed in the houses. Such kinds of malpractise reduced mosquito control measures in the communities (Figure 4).

An observation survey of ITN misuse in the study area.
Household Member Health-Related Characteristics
Of the household members who had a fever history within one past week 152 (36.1%), and 138 (32.8%) household members were previously infected with malaria. Nearly half 195(46.3%) of the households stayed outside during the night, and 48 (11.4%) household members recently traveled to malaria-endemic areas (Table 4). The malaria parasite was detected among 117 (27.8%) under five years old children. Out of the examined species of malaria-causing agents, 80 (68.4%) were P. falciparum, 30 (25.6) were P. vivax, and 7 (6%) were mixed.
Household Member Health-Related Characteristics.

Factors Associated with Malaria Prevention Practices
Binary logistic regression was applied to analyze the independent variables against the outcome. In multivariate analysis, the factors significantly associated with malaria prevention were identified. Those with malaria prevention knowledge were 1.6 times more likely to practice good malaria prevention than those without malaria prevention knowledge [AOR = 1.6, 95% CI = 1.0–2.5]. The absence of plasmodium parasites among children was fourfold more likely to be a good malaria prevention practice than its counterpart [AOR = 4.3, 95% CI = 2.8–8.7]. However, households that stayed outdoors at night were 46% less likely to be good malaria prevention practices than households that did not stay outdoors at night [AOR = 0.5, 95% CI = 0.3–1.0] (Table 5).
Factors Associated with Malaria Prevention among Households in Three Districts of Borena Zone, Southern Ethiopia, 2022.

Statistical significance at P < 0.001 = ***, P < 0.01 = ** and P < 0.05 = *, COR = crude odds ratio, AOR = adjusted OR with CI = confidence interval, ITN = Insecticide Treated Nets, ETB = Ethiopian birr.
Discussion
The present study revealed that the overall malaria prevention practice among households was 31.6% (95%; CI = 27.2-36.04). This finding was lower than that of a study conducted in the Kilosa district of central Tanzania, which reported 53.5% of household practice malaria prevention practices. 16 The possible reason for lower prevention practices in the study area may be due to poor government intervention, community socioeconomic status, knowledge, and availability of control measures.
The findings of the current study were lower than those of studies conducted in different areas of Ethiopia: Hawassa City 54.4% 9 and Botor-Tolay district in southwestern Ethiopia 55%. 10 The possible reason for the higher prevention practice score in these studies could be that they were conducted in cities where most of the communities were educated and close to the central part of the country where intervention was higher than in remote areas. Moreover, the primary difficulties in conducting the intervention were the mobility of the pastoral community and were difficulty to access, particularly after rainstorms. 18
In this study, below half 47.5% of households utilized at least one ITN in the house. This result was lower than a study conducted in rural central Tanzania 95.5%, 19 Senegal 64%, 18 Uganda Wakiso district 64.8%, 20 Ghana municipality 60%, 21 and Hawassa city 73.5%. 9 The lower ITN utilized in the houses of the pastoral community might be due to a lack of government or nongovernment organization donations for more than a year, the poor socioeconomic status of the community after being hit by drought, and the community neglected the ITN and misuse ITN for other purposes. The possible implications could be due to lack of knowledge, the life nature of pastoral communities, insufficient resources, and materials such as ITN uses for kitchen sheltering, plant protection, thread making, selling to feed families, and other purposes in the study area.
On the other hand, only 1.2% of households had indoor residual spray (IRS) to the house in the last year. This finding was lower than a study conducted in Uganda Wakiso district 5.8%, 20 Ghana municipality 54%; 21 Hawassa city 76.7%, 9 and Botor-Tolay district in southwestern Ethiopia (69%). 10 This could be explained by the lack of availability, expense for the community, and lack of government attention to the IRS as an intervention in pastoralist areas.
Among households, 30.6% practiced traditional preventive methods to prevent mosquito bites. Some of the practices in the pastoral community of southern Ethiopia were cleaning stagnant water, smoking firewood, applying body Vaseline, covering the body, or sleeping with clothes, especially during the night. In addition, sometimes this community exercises sleeping near livestock to protect themselves from mosquito bites, although a study revealed that livestock is a significant predictor of malaria prevalence. 22
Multivariate analysis indicated that malaria prevention knowledge was significantly associated with malaria prevention practices. Having malaria prevention knowledge was 1.6 times more likely to result in good practice of malaria prevention. This finding agreed with the study conducted in Hawassa City 9 and the Botor-Tolay district in southwestern Ethiopia. 10 The Conceivable reason for this may be due to knowledge regarding the mechanism of prevention of the individual increases, the probability of practicing preventive activities, and triggers of one motive of practice. 9
Findings from this study demonstrated that malaria prevention practices were significantly associated with the absence of the plasmodium parasite among household children. The odds of malaria absences among children were 4 times higher among good prevention practice households. This result agreed with studies conducted in the Hadiya Zone, Ethiopia, 23 and the Sherkole Benishangul-Gumuz region. 11 The possible justification could be that good prevention practices reduce mosquito breeding, bite, block transmission and eliminate the burden of malaria.
This study revealed that the household staying outdoors at night was statistically significant. The household staying outdoors was 46% less likely to be a good malaria prevention practice when compared with households that did not stay outdoors at night. This could be because staying outdoors at night increases the chance of mosquito bites and easily transmits the infection from person to person. 24
The Strengths and Limitations of This Study
The study is conducted on randomly selected households in the pastoral communities among three districts. However, the study was conducted with a small sample size, which is insufficient for the generalizability of the findings. However, the study did not assess the attitudes of the pastoral community that can influence prevention practices and who slept under the net, and the knowledge of the participants not in detail studied. The cross-sectional study design effect and respondents’ bias may affect the acceptance of the results.
Conclusion
The study shows low malaria prevention practices among pastoral community households in three districts of the Borena Zone in southern Ethiopia. Lower IRS to the house and low availability of ITN and misuse of ITN were observed in the study area. The significant factors associated with malaria prevention practices were prevention knowledge, absence of malaria infection among household children, and staying the night outdoors. Even though there are existing prevention methods, these rural communities are still using traditional methods which have lower odds of reducing malaria. To achieve national and global malaria elimination goals, the government should distribute ITN, LLITN, and IRS to remote areas of pastoral communities. Health extension workers should have to create awareness for the communities to avoid incorrect use of the ITN. The researchers should be conducted on the intervention in malaria prevention in pastoralist areas with a large sample size.
Supplemental Material
sj-docx-1-hme-10.1177_23333928221144555 - Supplemental material for Pastoral Community Malaria Prevention Practice and Associated Factors Among Households in Three Districts of the Borena Zone, Southern Ethiopia
Supplemental material, sj-docx-1-hme-10.1177_23333928221144555 for Pastoral Community Malaria Prevention Practice and Associated Factors Among Households in Three Districts of the Borena Zone, Southern Ethiopia by Alqeer Aliyo, Wako Golicha and Anteneh Fikrie in Health Services Research and Managerial Epidemiology
Footnotes
Abbreviations
Acknowledgments
We would like to express our deepest gratitude to Bule Hora University for giving grants to conduct this research. Our earnest gratitude goes to the data collectors, health extension workers and Woreda heath offices. Finally, our heartfelt thanks go to Mr Alo Mamo and Mr Abdo Kampe for sharing background information.
Authors’ Contributions
Availability of Data and Materials
Data essential for the conclusion are included in this manuscript and additional data can be obtained from the corresponding author upon reasonable request.
Competing Interests
We declare that we do not have conflicts of interest on all activities pertaining to this research work.”
Consent for Publication
“Not applicable”
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.