
Abstract
Background
Regardless of its benefit in promoting maternal health, contributing to a healthy pregnancy, little is known concerning the prevalence of utilization of preconception care and its determinant in southern Ethiopia. Hence, this study designed to determine the prevalence of utilization of preconception care and contributing factors among pregnant women in West Guji Zone, Southern Ethiopia, 2021.
Methods
A community-based cross-sectional study was conducted among systematically selected 660 pregnant women in West Guji from June 15 to July 30, 2021. A pretested interviewer-administered structured questionnaire was used to collect the data. Data entry was done in Epidata version3.1 and exported to SPSS version 25 for analysis. Descriptive statistics were used to summarize the data. To identify the factors associated with the utilization of preconception care binary and multivariable logistic regression analysis was performed. Adjusted odds ratios (AOR) with 95% CI were estimated to assess the strength of associations and statistical significance was declared at a p-value < 0.05.
Results
One hundred-forty seven, 22.3% [95% CI (19.2, 25.4)] of mothers utilized preconception care. Being college and above [(AOR = 5.51 95%CI 91.43-21.19)] and secondary [(AOR = 4.46 95%CI (1.38-14.39)] in educational status, rich [(AOR = 4.23 95%CI (1.32-13.55)], having good knowledge about preconception care [AOR = 2.34 95%CI (1.05-5.28)], having a positive attitude towards preconception care [(AOR = 9.99 95%CI (4.25-23.48)] and deciding with her husband regarding maternal health services [(AOR = 4.71 95%CI (1.91-11.56)] were factors positively affecting utilization of preconception care.
Conclusions
The utilization of preconception care in the study area is low. Being college and above and secondary in educational status, rich, good knowledge, positive attitude towards preconception care, and deciding with her husband regarding maternal health services were independent factors promoting the utilization of preconception care. Information, education, and communication activities should be strengthened to increase awareness of mothers about preconception care.
Introduction
Preconception care is the providing of biomedical, behavioral, and social health interventions to women and couples before conception occurs. It comprises the care earlier the first pregnancy and the care between the succeeding pregnancies. 1
The core preconception care includes the entire range of actions intended to promote the health of the hopeful mother and her child, which contains screening for different diseases, ecological hazards and toxins, illegal drugs, nutrition and folic acid intake, weight management, genetic conditions and family history, tobacco and alcohol use, vaccinations, and, family planning. 2 It is key to lessen different risk practices, exposures that distress conception, fetal growth, and eventually reduce subsequent adverse outcomes. 3 It increases the health of women and men while decreasing the likelihoods that their offspring will experience: prematurity, low birth weight, birth defects, or other birth-related conditions that could delay optimum child development.4,5 Preconception care is considered an prior chance not just for family planning or to reduce maternal and neonatal mortality, but also to improve continuing outcomes for adolescent girls, women, and children. 6
The World Health Organization (WHO) recently identified that globally 4 out of 10 women reported that their pregnancies were unintended. As a result, 40% of pregnancies miss the essential health services required before pregnancy. 7 The Center for Disease Control (CDC) recommends risk identification and counseling for all women of reproductive age as part of primary health care visits to improve pregnancy outcomes. 8 However, unfortunately, lots of women in the world do not have access to preconception, pregnancy, health services, and childbirth with appropriate quality, especially poor, uneducated women or those in underprivileged areas. 9
In high income countries, there is a policy for preconception care, whereas preconception care in low income countries is a much disused maternal health care service that requires special consideration. Even though there are high pre-pregnancy risk factors, the intention among men and women to look for preconception care is still inadequate in developing countries.10,11 The prevalence of utilization of preconception in China, Iran, and Nepal was 40.0%, 12 47%, 10 and 51%, 13 respectively. Different studies carried out in Ethiopia found that the level of utilization of preconception care ranges from 9.6%-18.2%14,15 which is much lower than in other developing countries. Though overall health care has improved in Ethiopia still much needs to be done, for example in the cases of abnormal pregnancy consequences, specifically neural tube-related defects such as anencephaly, spinal bifida, and encephalocele, are increasing at an alarming rate. Moreover, PCC service is provided in both hospitals and health centers in Ethiopia. However, there are concerns about systematic and consistent PCC services provided for all reproductive age group mothers.16,17
Having appropriate use of preconception care declines maternal and child mortality about by 57% and maternal and child morbidity by 73%.3,18 Preconception care utilization could also reduce 71% of unintended pregnancies, thereby reducing 22 million unplanned births, 25 million induced abortions, and 7 million miscarriages.19,20 Lack of preconception care and low folic acid supplementation for women in low income countries might increase the risk of neural tube defect in newborns by four times compared with high income countries, whereas taking folic acid decreases neural tube defects up to 80%. 21
Preconception care utilization is affected by age, gender, educational status, income, marital status, family planning use, health condition, ANC visits, parity, pregnancy intention, and gravidity.13,15,22,23 It is expected that the finding of this study will deliver insight for health sector administrators and NGOs working on maternal health and co-sectors, in general, to formulate mechanisms to address preconception care for mothers before conception. In spite of its significance in improving maternal health, leading to a healthy pregnancy, little is known about the magnitude of preconception care utilization and its associated factors in Ethiopia particularly in the study area. Therefore, this study aimed to assess the utilization of preconception care and its associated factors among pregnant women of West Guji Zone, Oromia region, Ethiopia.
Methods and Materials
Study Area, Design, and Period
A community-based cross-sectional study was conducted in West Guji Zone, Oromia Region. Bule Hora town is the capital city of West Guji Zone which is located 467 km from Addis Ababa, the capital city of Ethiopia, and 194 km from Hawassa. West Guji zone has nine woredas and two town administrations in the Zone. It has also 196 kebele, as the lower administrative unit; of these 166 are rural kebeles whereas 30 are urban kebeles. It has an estimated total population of 1,389,821 of whom 681,012 are males and 708,809 are females. The Zone has one General Hospital, 3 primary hospitals, 42 health centers, and 166 health posts. The total number of pregnant women as projected from the total population of West Guji Zone in 2019 was 48234.
Study Participants, Inclusion and Exclusion Criteria
The source population was all pregnant women living in West Guji Zone. On the other hand, all pregnant women living in randomly Selected Districts and towns of West Guji Zone for the period of the data collection were the study population. All pregnant women who were living in West Guji Zone for less than 6 months and those women who were seriously ill or unable to give the required information were excluded.
Sample Size Determination and Sampling Procedure
A single population proportion formula was used to determine the sample size. Considering the prevalence of preconception care utilization of 13.4% found from a previous study done in Debre Berhan Town, 23 a 95% confidence interval and a margin of error of 4%, a design effect of 1.5% and 10% non-response rate was also considered. The final calculated sample size became 461. A double population proportion was used to determine a sample size for the second objective using Epi-info version 7.1 by considering the power of the study of 80%, CI of 95%, knowledge of PCC as a significant variable as of a earlier study done in Northern Ethiopia 15 with a proportion of PCC utilization among unexposed of 11.6% and AOR of 2.21 which yields a sample size of 677. Therefore, the biggest sample size calculated from the second objective 677 has been taken.
A study participant from west Guji Zone was selected by using a multistage sampling technique. Firstly, from a total of nine districts and two town administrations of West Guji Zone, three districts and one town administration were selected by simple random sampling technique by using the lottery method. Then the study kebeles were selected by simple random sampling and for each kebele, a proportional allocation to sample size was performed. Finally, Study Participants from each kebeles were selected by using a systematic sampling technique. Every 11nth pregnant woman was questioned.
Study Variables
The dependent variable of the study was the utilization of preconception care. Independent variables were: Socio-demographic factors (the mothers age, educational status of the mother, educational status of husband, marital status, religion, ethnicity, occupation of the mother, occupation of husband, household’s wealth status and family size). Obstetric and reproductive health service utilization (Gravidity, parity, number of children, ANC visit, family planning use, place of childbirth, mode of delivery and PNC visit). Medical conditions and adverse birth outcome variables (chronic illness, history of adverse birth outcome). Knowledge and attitude related factors (knowledge regarding PCC and attitude towards PCC). Parental and health facility related factors (husband support, participants of women in a community meeting regarding maternal health, availability of essential medications and laboratory services, and distance of health facilities from home).
Operational Definition and Terms
Preconception care utilization
If women received at least one type of intervention, either advice or treatment, and lifestyle modification care (screen for any disease and get treatment, take folic acid, take vaccine, get counseling, modify diet, cessation of alcohol, cessation of cigarette smoking, stop taking of illegal drugs, plan pregnancy, create healthy environment) at least once before being pregnant will be considered as mother utilized PCC. 23
Good knowledge regarding PCC
Participants who scored above the mean score about preconception care knowledge questions were regarded as having good knowledge.
Good attitude towards PCC
Participants who scored above the mean score about attitude questions were regarded as having a good attitude.
Data Collection Procedures and Quality Assurance
A data from a pregnant woman was collected by using a structured interviewer-administered questionnaire. The questionnaire was constructed by adapting from previous literature and the questionnaire was amended to fit the research objective and the local condition. The questionnaire was initially prepared in English and then translated into Afaan Oromo (local language) by different language experts of both languages and then to English to check its consistency.
Data was collected by sixteen trained degree nurses who are fluent speakers in the local language and supervised by four master’s public health professionals. A face-to-face interview technique was conducted at the study participants’ house. The training was provided for both data collectors and supervisors on how to manage the data collection process. The questionnaire was pretested two weeks before the actual data collection with 5% of the sample size (34 pregnant women) in Borena Zone and the necessary amendment was done on the questionnaire per pretest result. The overall activities of data collection were supervised and coordinated by the investigators. The collected data were checked for consistency, completeness, and relevance daily during the entire data collection by the supervisors and principal investigator. The collected data also was checked for missed values and outliers.
Data Processing and Analysis
The collected data were coded, entered, and cleaned by Epidata version 3.1 and exported to Statistical Package for Social Science (SPSS) version 23.0 for analysis. Descriptive statistics were done to describe the data. The household wealth index was computed by using a composite indicator by considering properties, like selected household assets, and analyzed by using Principal Component analysis. Final factors were ranked into three categories (poor, rich and medium). Binary logistic regression analysis was employed to examine the statistical association between utilization of preconception care and every single independent variable. Variables that showed statistical significance during Bivariable analysis at (p-value <0. 25) were entered into multivariable logistic regression to identify statistically significant variables. Multicollinearity was tested by using the variance inflation factor and tolerance test. The Hosmer-Lemeshow test was used to check the model fitness for analysis. Adjusted odds ratios (AOR) with 95% CI were estimated to assess the strength of associations and statistical significance was declared at a p-value < 0.05. Tables, figures, and text were used to present results.
Results
Sociodemographic Characteristics of Mothers
Out of 677 pregnant women initially included in this study, 660 (97.5%) have replied to the interview. The majority of the study participants 347 (52.6%) were in the youth age group of (15 to 24) years. The mean (±SD) ages of the respondents were 25.67
Sociodemographic Characteristics of Pregnant Women in West Guji Zone, Southern Ethiopia, 2021 (n = 660).

Obstetric Characteristics of Mothers
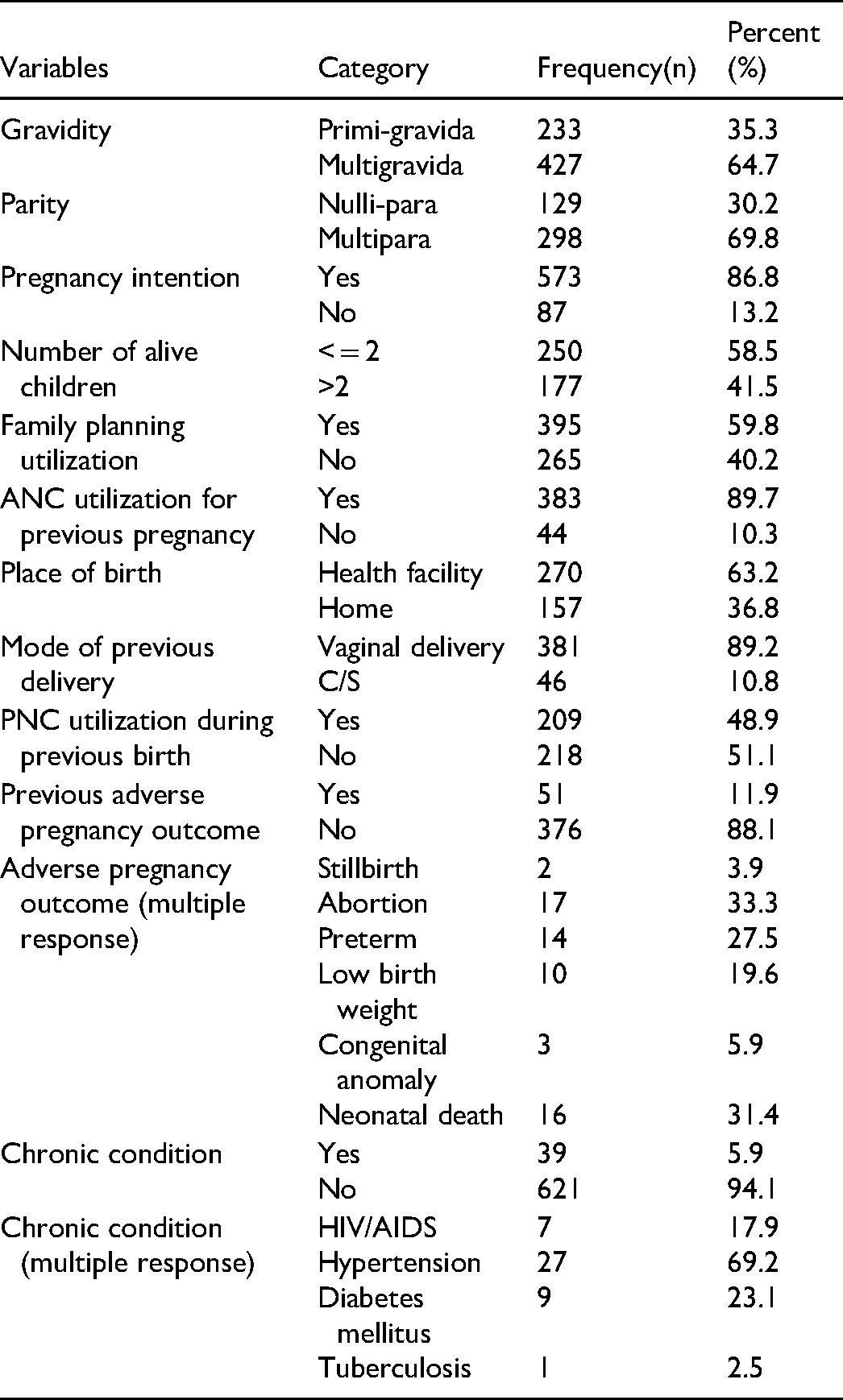
Nearly two-third, 64.7% and seven-in-ten, 69.8% of mothers were multigravida and multiparous, respectively. Majority of the respondents, 573(86.8%) and 250(58.5%) had intended pregnancy and two or less alive children, respectively. The majority, 395 (59.8%) and 383(89.7%) of the respondents had ever utilized family planning and ANC services for current pregnancy, respectively. Nearly two-third, 63.2% of respondents places of previous delivery were health facilities. Almost half, 48.9% of the respondents had ever utilized postnatal care. Majority, 376(88.1%) of respondents had no previous adverse pregnancy outcome (Table 2).
Obstetric Characteristics of Pregnant Women of West Guji Zone, Southern Ethiopia, 2021 (n = 660).
Knowledge About Preconception Care
Three fourth, 73.5% of mothers agreed that they should avoid bad practices when planning for pregnancy. Nearly half, 47.3% 0f mothers agreed that testing for HIV/AIDS when planned for pregnancy is important. One third, 31.7% of respondents agreed that they should receive folic acid and multivitamins to prevent neural tube defects. Half, 51.4% of mothers had knowledge that they should preserve body weight when planned for pregnancy. Two hundred seventy-three, 41.4% of respondents had knowledge that they should receive zinc when intended for pregnancy. Two hundred ninety-eight, 45.2% of mothers had good knowledge about preconception care, while remaining 362(54.8%) of the mothers had poor knowledge about preconception care (Table 3).
Mothers Response for Knowledge Questions Regarding Preconception Care among Pregnant Women of West Guji Zone, Southern Ethiopia, 2021 (n = 660).

Attitude Towards Preconception Care
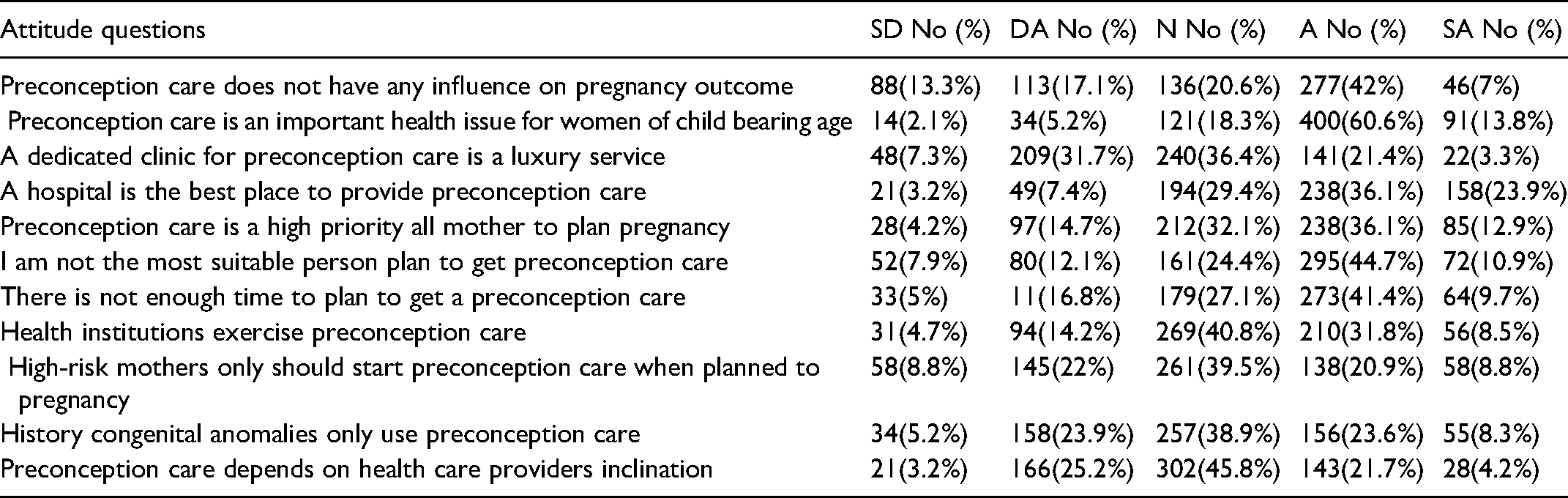
Among the total of 660 respondents, 400(60.6%) of respondents also agreed that preconception care is an important health issue for women of child bearing age and 238(36.1%) of the mothers agreed that a hospital setting is the best place to provide preconception care. Two hundred thirty-eight, 36.2% of the respondents agreed that preconception care is a high priority mother to plan pregnancy. Besides, 273(41.4%) of participants agreed that there is no enough time to plan to get preconception care. Three hundred forty-two, 51.8% of respondents had a positive attitude toward preconception care, while the remaining, 318(48.2%) of participants had a negative attitude toward preconception care (Table 4).
Mothers Response for Attitude Questions among Pregnant Women of West Guji Zone, Southern Ethiopia, 2021 (n = 660).
Utilization of Preconception Care
One hundred forty-seven, 22.3% [95% CI (19.2, 25.4)] of mothers utilized preconception care. The most frequently used component of PCC in this study was screening and treatment of HIV/STI, 128(87.1%) while the least utilized was optimizing psychological health, 39(26.5%) (Figure 1).

Types of care utilized by mothers among pregnant women of west guji zone, southern Ethiopia, 2021 (n = 660).
Health Facility and Parental Support
Majority, 403 (61.1%) and 363 (55%) of the participants confirmed that there were availability of adequate laboratory and medication service, respectively. Three hundred seventy-eight (57.3%) of the participants mentioned that the time to reach the nearby health facility with foot took more than 30minutes. Three hundred seventy-nine, 57.4% of the respondents haven’t attended a community meeting about reproductive health services. Among the study participants who are married half, 49.1% of respondents had support from their husbands for preconception screening. Two hundred seventy 40.9% of mothers make a decision about maternal health services with their husbands (Table 5).
Health Facility and Parental Support among Pregnant Women of West Guji Zone, Southern Ethiopia, 2021 (n = 660).

Factors Associated with Utilization of Preconception Care
To identify factors affecting the utilization of PCC bivariable and multivariable logistic regression analysis was done. After controlling the confounding factors, the multivariable analysis revealed that the following factors have an association with the utilization of preconception care: Educational status of the mother, wealth status of family, knowledge about preconception care, attitude towards preconception care, and decision makers for maternal health. Those mothers who attained secondary education were 4.46 times more likely (AOR = 4.46, 95% CI 1.38, 14.39) to utilize preconception care compared to mothers who had no formal education. Those mothers who were college and above in educational status were 5.51 times more likelihood (AOR = 5.51, 95% CI, 1.43, 21.19) of utilizing preconception care compared to mothers who had no formal education. Mothers who were rich had 4.23 times more likelihood (AOR = 4.23 95% CI, 1.32, 13.55) utilizing preconception care compared to mothers who were poor. Mothers who had good knowledge about PCC were 2.34 times more likely (AOR = 2.34 95% CI, 1.05, 5.28) to utilize PCC when compared to their counterparts. Mothers who had positive attitudes toward PCC were 9.99 times more likely (AOR = 9.95 95% CI, 4.25, 23.48) to utilize PCC when compared to their counterparts who had a negative attitude towards PCC. Those mothers who made a decision with her husband were 4.71 times more likely (AOR = 4.71, 95% CI 1.91, 11.56) to utilize PCC as compared to those mothers who made a decision regarding maternal health services by herself (Table 6).
Bivariable and Multivariable Logistic Regression Analysis of Factors Associated with Utilization of Preconception Care among Pregnant Women in West Guji Zone, Southern Ethiopia, 2021 (n = 660).

Key: * = statistically significant at p < 0.05 in multivariable logistic regression;
1 = indicated the reference category.
Discussion
Understanding of Preconception care is crucial for many Sub-Saharan African countries, such as Ethiopia, where maternal and perinatal mortality remains alarmingly high. 15 This community-based cross-sectional study was carried out to assess the utilization of preconception care and its associated factors among pregnant women of West Guji Zone. This study found that 22.3% of the study participants had utilized preconception care. Educational status of the mother, wealth status of the family, knowledge about preconception care, attitude towards preconception care, and decision makers for maternal health were found to be independent factors affecting the utilization of PCC among pregnant women in West Guji Zone, Southern Ethiopia.
The prevalence of preconception care 22.3% obtained by this study is similar with the different studies done in Aga Khan University Hospital of Kenya, 24 Mekele city 15 and, Addis Ababa. 25 This similarity might be due to socioeconomic similarity among participants.
This finding is higher than the report from the study done in Sao Polo, Brazil, 26 Abakalik, Southern Nigeria, 27 Debre Berhan town 23 and, Adet Town. 28 This finding is lower than the study done in Malaysia, 29 Saud Arabia, 30 Kaznazan, Iraq 31 and, Obafem Awolwo University Hospital, Nigeria. 32 The possible explanation for the discrepancy might be due to differences in the study setting, health service access and sociodemographic characteristics of the countries.
This study found that those mothers who were college and above and, attained secondary school were 5.51 and 4.46 times more likely to utilize preconception care when compared to mothers who had no formal education respectively. This finding was in line with the study done in Malaysia, 29 Saud Arabia, 30 and Adet town. 28 This might be due to that mothers who were educated might have the opportunity to get information about the importance of preconception care for the wellbeing of the mother and children through formal education or indirectly through different social Medias.
Mothers of rich wealth status were 4.23 times more likely to utilize preconception care when compared to those mothers with poor wealth status. This is comparable with the study done in West Shewa Zone, Ethiopia. 17 This might be due to that mothers with low socio-economic status cannot afford their health expenses. Rich mothers might also have access to information about maternal health services through different Medias.
Mothers who had good knowledge about PCC were 2.34 times more likely to utilize PCC when compared to their counterparts who had poor knowledge about preconception care. This finding is in lines with the study done in Malaysia, 29 Mekelle city, 15 and west Shewa zone. 17 This might relate to information leading to knowing details about the importance of service. In addition to that, knowledge about PCC might improve attitudes towards PCC that might in turn improve the utilization of preconception care.
Mothers who had positive attitudes toward PCC were 9.99 times more likely to utilize PCC when compared to their counterparts who had a negative attitude towards PCC. This might be due to that mothers who had a good attitude towards PCC will try their best to reduce the barriers affecting utilization of preconception care.
Those mothers who made a decision with her husband were 4.71 times more likely to utilize PCC when compared to those mothers who made a decision regarding maternal health services by women alone. This significance is in line with the study done in Mekelle city. 14 This might be due to that mothers who made a decision with her husband might have confidence for the importance of PCC and her husband might also help her financially that increases the affordability of services.
The nature of problem under the study requires the potential ability of respondents to remember information retrospectively, recall bias is also the other limitation of this study.
Conclusions
This study found that the utilization of preconception care in the study area is low. Being college and above and secondary in educational status, rich wealth status, good knowledge about preconception care, positive attitude towards preconception care, and deciding with her husband regarding maternal health services were independent factors positively affecting the utilization of preconception care. Information, education, and communication activities should be strengthened in communities that increase the awareness of mothers about preconception care.
Footnotes
Acknowledgments
First, we would like to express our deepest thanks to Bule Hora University Research and Publication Directorate for providing this wonderful opportunity to prepare this research paper. Then we would like to acknowledge West Guji Zone Health Department for giving important information needed for this research paper. Lastly, our acknowledgments also go to data collectors, supervisors, and those who were cooperatively participated in our study.
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Bule Hora University. Based on the approval, an official letter was written by Bule Hora University Research and Publication directorate to West Guji Zone Health Department. Explanation on the objective of the research was provided to the concerned personnel at each level. The West Guji Zone Health Department wrote a letter to the selected districts and cities for cooperation. At last, data was collected after assuring the confidentiality nature of the responses and obtaining verbal consent from the study participants. All study participants were encouraged to participate in the study and at the same time they were also told that they have the right not to participate.
Participant consent
Obtained
Consent for publication
Not applicable.
Availability of data and materials
For those who are interested; the datasets of this study could be accessed from the corresponding author on reasonable request.
Authors’ contributions
EA, AF, and TU conceptualized the paper, conducted the data collection process, and analyzed the data. EA, AF, and TU wrote the draft of the manuscript. EA, AF, and TU revised and edited the manuscript draft. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.