
Abstract
Background
Hepatitis B virus (HBV) is one of the major threats to global health, affecting millions of people each year and causing morbidity and mortality. The risk of acquiring chronic HVV infection varies with age, with 90% of infections acquired during the perinatal period. Despite many studies, there is little evidence of this virus in the Borena Zone.
Objectives
This study was done to assess seroprevalence HBVinfection and associated factors among pregnant women attending antenatal care at selected Borena Zone public hospitals from June 1 to September 30, 2022.
Methods
A cross-institutional study was conducted on 368 randomly selected pregnant women who received antenatal care at Yabelo General Hospital and Moyale Primary Hospital. Data on sociodemographic and HBV-related factors were collected using a structured questionnaire. A 5 mL blood sample is then taken and tested using a diagnostic method, the enzyme-linked immunosorbent assay. Finally, data were entered using Epidata version 3.1 and exported to SPSS version 25 and Stata version 14 for analysis. Independent predictors were identified using logistic regression analysis and P < .05 was considered statistically significant.
Results
The prevalence of HBV infection was 21 (5.7%) (95% confidence interval [CI], 3.74-8.61). History of hospitalization (adjusted odds ratio [AOR] = 3.44, 95% CI, 1.07-11.09), traditional tonsillectomy (AOR = 4.16, 95% CI, 1.29-13.40), history of sexually transmitted infection (AOR = 5.99, 95% CI, 1.81-19.85), human immunodeficiency virus (HIV) (AOR = 8.28, 95% CI, 1.66-41.41), and alcohol drinking (AOR = 5.08, 95% CI, 1.49-17.31) were independent predictors of HBV infection.
Conclusions
The results of this study indicate a moderate prevalence of HBV in selected public hospitals in the Borena Zone. History of hospitalization, traditional tonsillectomy, sexually transmitted infections, HIV, and alcohol use was significantly associated with HBV infection. Therefore, there is a need to conduct health education and more community-based research on disease transmission routes.
Introduction
Hepatitis B virus (HBV) is a virus that can cause acute or chronic infection. HBV infections in pregnancy are the most common cause of morbidity and mortality for both mother and fetus.1,2 Presence of HBV infection in early life increases the risk of chronic liver disease, the development of cirrhosis, splenomegaly, and hepatocellular carcinoma. 3 Also, it may cause maternal complications and infant death by impaired mental and physical health.2,4The common transmission way of HBV is generally through vertical or perinatal and horizontal transmission. Vertical transmission is the transfer of the virus from mother to infants and horizontal transmission is generally by mucosal exposure to HBV-contaminated blood and other body fluids such as saliva, vagina, and seminal fluids through unprotected sex, medical and surgical procedures, tattooing, scarification, and sharing of sharps. 5
Hepatitis B virus is a major global health problem, with 30.4 million people worldwide infected with HBV and nearly 296 million people with chronic hepatitis. Worldwide, approximately 820,000 people die from HBV-related deaths, and 1.5 million people are newly infected with HBV. 6 Globally, the prevalence of HBV infection in the general population was 3.8%, and the geographical distribution of HBV was highest in the WHO Regions of Africa and the Western Pacific, with prevalences of 7.5% and 5.9%, respectively. 6 About 65 million women between the ages of 15 and 49 years have been infected with HBV, and 9 of 10 mothers with hepatitis B have the disease in their babies at birth.7,8
According to the WHO Global Progress Report on human immunodeficiency virus (HIV), Viral Hepatitis and Sexually Transmitted Diseases, the prevalence of hepatitis B in the general population in 2021 will be highest in the WHO Africa Region, with the estimated prevalence of 7.5% (5.7-10. Estimated prevalence is 5.9% (4.9%-7.3%). 6 In Ethiopia, the prevalence of HBV in children under 5 years of age is 5.7% 9 and the prevalence of HBV infection among pregnant women is 5.7%. 9 The pooled prevalence is 4.75%. 10
In response to the sustainable development goals, WHO developed the first Global Health Sector Strategy on viral hepatitis, due for 2016 to 2021. 8 Also, HBV screening in all pregnant women, universal Hepatitis B (HB) birth dose within the first day after delivery, and hepatitis vaccination are considered effective methods to reduce mother-to-child transmission by 90%. 11 However, most developing countries have not yet adopted HBV vaccine, the birth dose administered to all newborns.12,13 In Africa, only 11 countries include HBV birth dose as part of their routine Expansion of Program Immunizations (EPIs), and none of the East African countries do so. 14 Despite WHO recommendations, health facilities in Ethiopia lack routine prenatal screening for HBV, vaccination with HBV birth doses, and universal hepatitis B vaccination. 15 Moreover, some privately owned private health facilities offer HBV vaccines at price too high for the majority of the population.15,16
In previous studies conducted in Ethiopia, the seroprevalence of HBV was 5.5% in Tigray, 17 6.5% in Oromia, 18 9.2% in Southern Nation Nationalities and People’s Region (SNNPR), 19 and 3.7% to 9.2% in Addis Ababa. 20 The HBV seroprevalence in pregnant women was associated with a history of blood transfusions, surgical history, tooth extraction, hospitalization, abortion, genital mutilation, family history of HBV infection, tattoos, noise, and ear piercings. It has also been reported that multiple sexual partner was associated with HIV positive.17–20 Another study conducted in Oromia showed no factors significantly associated with HBV seropositivity. 21
In addition, information from various studies showed that the degree of HBV infection and predictors of HBV infection varied by region. The extent and burden of the pregnant women's HBV infection are unknown, and there is no locally generated information on risk factors associated with pregnant women in the study area. Therefore, this study aims to assess the seroprevalence of HBV infection and associated factors among pregnant women attending antenatal care (ANC) at selected public hospitals in the Borena zone, southern Ethiopia.
Methods
Study Area, Design, and Period
The study was conducted on pregnant women who received ANC at a selected hospital in the Borena zone, Oromia region, southern Ethiopia. Borena zone has 13 districts and 1 municipality, bordered by the region of Somali to the east, West Guji to the north, Guji to the northeast, Kenya to the south, and the SNNPR to the west. It is one of the hotspot areas in the Oromia region. According to the Central Bureau of Statistics in 2019, the population of the zone is estimated to about 503,877. About 89% of the population lives in the zone's 134 rural pastoralist kebeles. The zone altitude is <1500 m above sea level. The average annual temperature is 27°C to 29°C.22,23 In terms of medical facilities, Borena zone has 4 primary hospitals, 1 general public hospital, and 44 health centers. 24 A facility-based cross-sectional study design was conducted at Yabelo General Hospital and Moyale Primary Hospital from June 1 to September 30, 2022.
Study Population and Selection Criteria
All randomly selected pregnant women who visited the ANC during the data collection period and who had their first ANC follow up at selected public hospitals during the study period were included in the study, while the pregnant women who are critically sick and unable to answer were excluded from the study.
Sample Size Determination
The sample size for this study was determined using the single-population ratio formula. When the HBV proportion (9.2%) is taken from a previous study conducted in the Gedeo zone, 19 there is an error rate of 3%, a confidence interval (CI) of 95%, and a nonresponse rate of 5% was assumed.

where n denotes the sample size, Z the value corresponding to 95% level of significance = 1.96, p the proportion of prevalence of HBV in pregnant women = 9.2%, d the marginal error assumed to be 3%, q = (1−p) = (1−0.092) = 0.908, and n = (1.96) 2 (0.092) (0.908)/ (0.03) 2 = 356.57 = 357.
Adding a 5% nonresponse rate, which is 18, the final sample size was
Sampling Techniques
From 5 public hospitals, 2 hospitals in Borena zone were selected using the lottery method. According to the previous data obtained from the past 3 months ANC follow up from registration, an estimated 543 and 836 pregnant women visit Yaballo and Moyale hospitals respectively. The total number of ANC attendants in 2 hospitals counted from ANC registration was 1379. The total sample size of pregnant mothers at each facility is then proportional to the population size based on previously enrolled ANC followers. Eligible pregnant women participating in ANC at the time of data collection were carefully selected using a systematic randomization procedure. To set the interval (k), divide the estimated total number of ANC attendants to the assigned study sample size. H·K = N/n, where N = sum of ANC attendants, n = desired sample size, K = sampling interval, K = 1379/ 375 = 3.7 ≈ 4, so every fourth suitable pregnant woman is included and interviewed until the required sample size is reached (Figure 1).
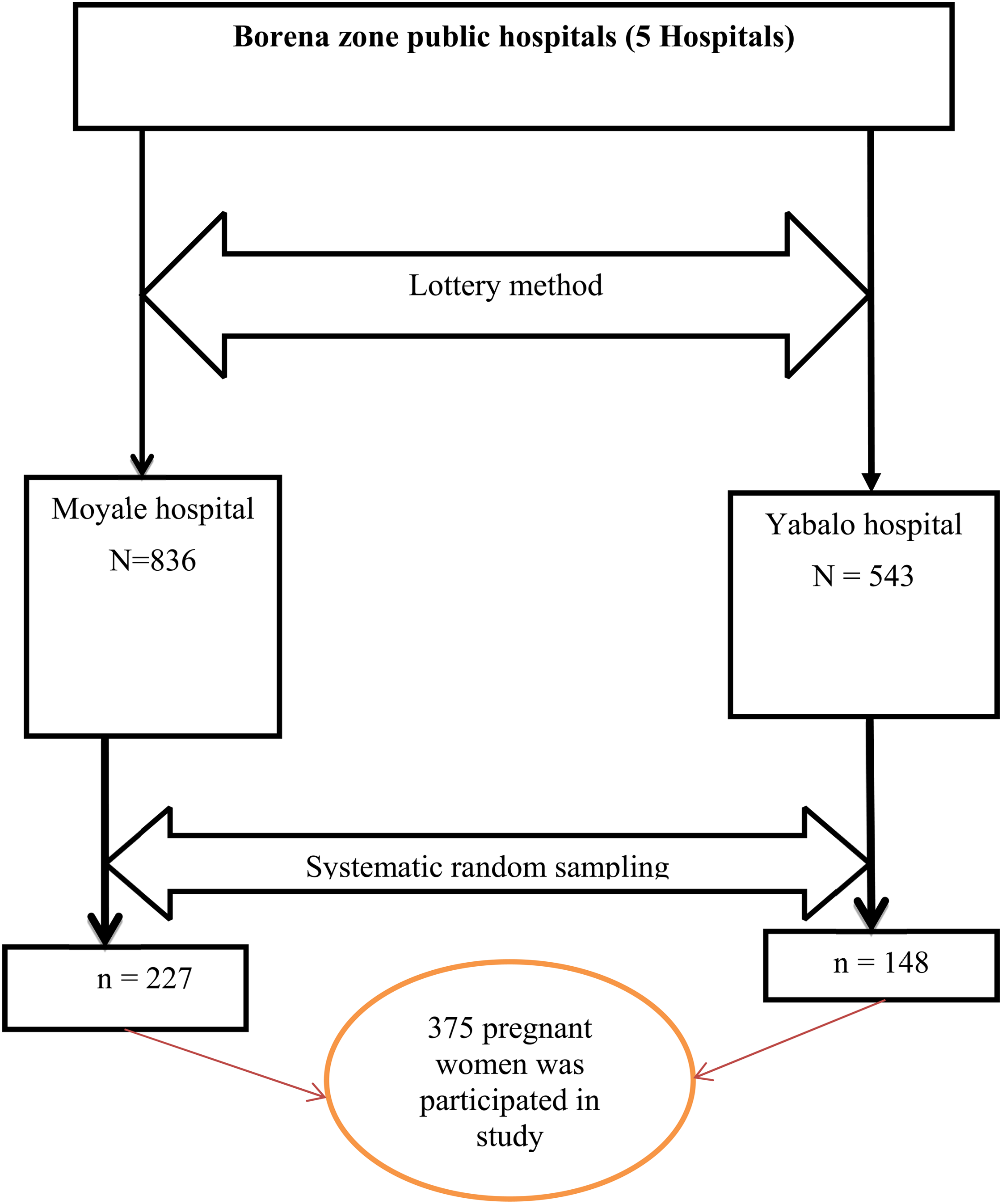
Schematic representation of the sampling procedure for prevalence and associated risk factors among pregnant women attending ANC of public hospitals in the Borena zone. Abbreviation: ANC, antenatal care.
Data Collection Method
Three midwives and 3 senior laboratory staff were recruited from the ANC office and laboratory. Data were collected using a structured questionnaire. The questionnaire was originally written in English and then translated into Afaan Oromo. The language version of Afaan Oromoo was reformulated into English to check for any contradictions or distortions in the meaning of words and concepts. The data collector introduced herself, explained the purpose of the study, and emphasized the benefits of having tested for HBV during pregnancy. The questionnaire was used to collect sociodemographic characteristics, previous healthcare-related risk behaviors, and practice-related information at ANC wards and 5 mL of venous blood samples were collected in laboratory for HBV screening.
Blood Collection
Five milliliters of venous blood were drawn from each study participant by an experienced laboratory technician. Regular standard operating procedures for sample collection were strictly followed. Serum was separated by centrifugation at 3000 rpm for 15 min.25,26 Each serum was subjected to a rapid hepatitis B surface antigen (HBsAg) test. The remaining serum samples were stored frozen until shipment from each medical facility. Positive results were confirmed by enzyme-linked immunosorbent assay (ELISA) testing by transportation to the Awassa Regional Blood Bank using refrigerated boxes. Data were collected by structured questionnaire through participants’ personal questions after verbal and written consent.
Data Quality Control
Data collectors and laboratory technicians responsible for sample processing were trained. The questionnaire was pre-tested on 5% of pregnant women sampled at Arero Hospital before the actual study and necessary changes were made to the study tool. Data collectors were supervised by the principal investigator, and data validity and completeness were checked by the principal investigator. Specimen collection, labeling, processing, storage, and testing were performed according to the laboratory standard operating procedures (SOPs) and manufacturer's recommendations. HBsAg Rapid Test performance has its own internal quality control and is evaluated using known positive and negative controls derived from ELISA test samples. Additionally, all positive and 10% negative samples were retested by ELISA.
Data Processing and Analysis
All completed checklists were checked for completeness and consistency and data were entered using Epidata version 3.1 software. Data were then exported to SPSS version 25 and Stata version 14 for further analysis. For univariate analysis, descriptive statistics were performed to examine the frequency distribution, central tendency, variability, and overall distribution of the independent variables. A bivariate logistic regression analysis was performed to select candidate variables for multivariate analysis. Variables with P values <.25 in the bivariate analysis were included in the multivariate logistic regression model. Multivariate logistic regression was performed to control possible confounding and identify the true effects of the selected predictors. Multicollinearity between independent variables was checked using variance expansion coefficients. Model fit was performed using Hosmer and Lemeshow statistics, Pearson's chi-square (χ2 = 9.31, P = .90), and was found to be nonsignificant, demonstrating model fit. The strength of the association between outcomes and determinants was assessed using adjusted odds ratios (AOR) with 95% CIs, and the significance of the association was reported at P values <.05.
Ethical Approval and Consent Participate
The ethical approval of this study was reviewed and approved by the Bule Hora University Ethical Review Board with reference number 09/2014. Official letters were written to Moyale and Yaballo hospitals, and the Borena zone Health Department wrote the letters of support to selected hospitals. Informed, voluntary, written, and signed consent was obtained from study participants and selected medical facilities. Participation in the study was voluntary and participants were informed that they had the right to withdraw/refuse to participate at any time during the study if they did not wish to participate. To ensure the confidentiality of participant information, a code was used and no participant identifiers were written on questionnaires and test tubes. Participants were interviewed alone to protect their privacy. Testing is free. Blood samples were used for study purposes only. Test results were sent to healthcare providers working in the ANC wards at the hospital for further diagnosis and treatment.
Results
Sociodemographic Characteristics of Study Participants
A total of 368 pregnant women were enrolled, with a response rate of 98.1%. The mean age of the participant was 24.74 with a standard deviation of ±4.71 years. About 129 (35.1%) of pregnant women were in the age range of 21 to 25 years. About 326 (88.6%) of women were housewives and only 5.2% were divorced and widowed. Concerning the place of residence, around 210 (57.1%) were urban residents. In terms of educational status, 159 (43.2%) of women were unable to read and write and only 20 (5.4%) attained above grade 12 and 275 (74.7%) of them were multigravida (Table 1).
Sociodemographic Characteristics of Pregnant Women Who Attended ANC at Selected Hospitals of Borena Zone, Southern Ethiopia, 2022.

Abbreviation: ANC, antenatal care.
Health-Related and Risky Behavior of Study Participants
Among the 368 women in the study, only 7 (1.9%) had a history of working in a health institution. Around 210 (57.1%) had an ear-piercing history, while only 48 (13%) women had a history of nose piercing. The majority, 212 (57.6%) of mothers, had a history of female genital mutilation. Of the total participants, 70 (19%) had a history of multiple sexual partners and 49 (13.3%) had a history of alcohol drinking (Table 2).
Health-Related and Risky Behavior Among Pregnant Women Who Attended ANC at Selected Hospitals of Borena Zone, Southern Ethiopia, 2022.

Abbreviations: AIDS, acquired immunodeficiency syndrome; ANC, antenatal care; HIV, human immunodeficiency virus.
Prevalence of HBV Among Pregnant Women Who Attended ANC Services
The overall prevalence of HBsAg was 21 (5.7%) with (95% CI, 3.74-8.61) in the prevalence among study participants at Yaballo and Moyale hospitals was 8 (5.4%) and 13 (5.9%), respectively (Figure 2). All 21 (5.7%) serum samples positive for HBsAg were confirmed positive by ELISA. The highest seroprevalence of HBsAg 7 of 104 (6.7%) was observed in the age group of 26 to 30 years and the lowest 4 of 92 (4.3%) in <21 years categories. The prevalence of HBsAg was highest in rural residents, 12 of 158 (7.6%), whereas 9 of 210 (4.3%) in urban residents. Concerning educational status, the prevalence of HBV was highest at 2 to 20 (10%) among those who attended above grade 12 and lowest at 2 of 95 (2.1%) among those able to read and write. About 1 to 93 (1.1%) and 20 to 275 (7.3%) were positive for primigravida and multigravida, respectively. The details are presented in Table 3.
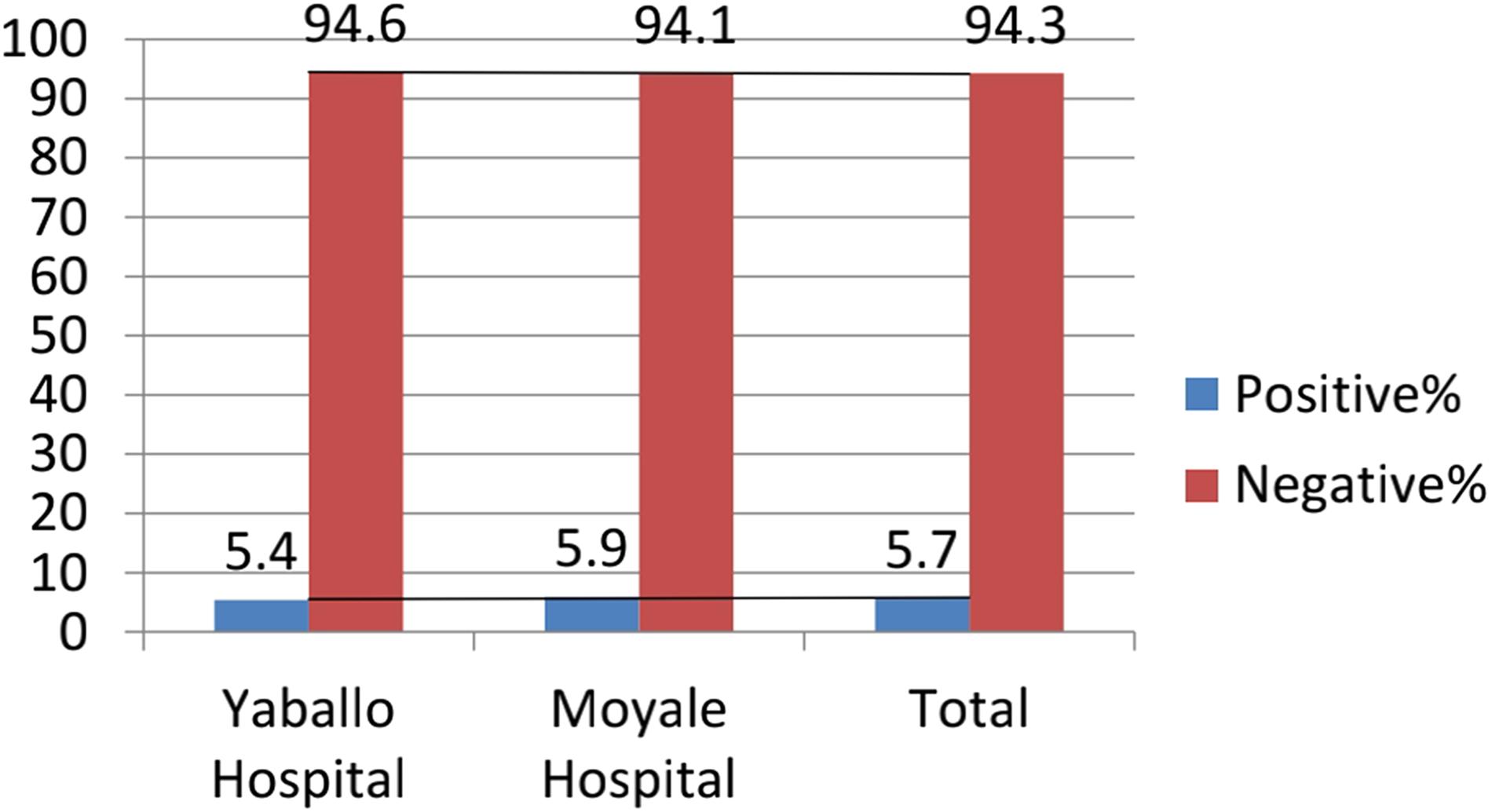
Prevalence of HBV among pregnant women attending ANC at selected hospitals in Borena zone, southern Ethiopia, 2022. Abbreviations: ANC, antenatal care; HBV, hepatitis B virus.
Prevalence of HBV With Sociodemographic Characteristics Among Pregnant Women Who Attended ANC at Selected Hospitals of Borena Zone, Southern Ethiopia, 2022.

Abbreviations: ANC, antenatal care; HBV, hepatitis B virus.
Factors Associated With the Prevalence of HBV
A logistic regression analysis showed that pregnant mothers who had been hospitalized were approximately 3 times more likely to have HBV infection than women who had not been hospitalized (AOR = 3.44, 95% CI, 1.07-11.09). Traditional tonsillectomy was 4 times more likely to be HBsAg seropositive compared to its counterpart (AOR = 4.16, 95% CI, 1.29−13.40). Pregnant women with a history of sexually transmitted infections were 6 times more likely to be infected with HBV than those without a history of sexually transmitted infections (AOR = 5.99, 95% CI, 1.81-19.85).
HIV infection was highly significantly associated with HBV infection, where HIV-infected pregnant women were around 8 times more likely infected by HBV than HIV-non-infected pregnant women (AOR = 8.28, 95% CI, 1.66-41.41). Pregnant women who had a history of alcohol drinking were about 5 times at higher risk when compared with those who had no history of alcohol drinking (AOR = 5.08, 95% CI, 1.49-17.31) (Table 4).
Bivariable and Multivariable Analysis of Associated Factors With HBV Infection Among Pregnant Women Who Attended ANC at Selected Public Hospitals of Borena Zone, Southern Ethiopia, 2022.

Note: Statistically significant at ***P < .01, **P < .05, Reference = 1.
Abbreviations: AIDS, acquired immunodeficiency syndrome; ANC, antenatal care; AOR, adjusted odds ratio; CI, confidence interval; COR, Crude odd ratio; HBV, hepatitis B virus; HIV, human immunodeficiency virus.
Discussion
In this study, the overall prevalence of HBV infection among pregnant women attending ANC services in the study area was 5.7% with (95% CI, 3.74-8.61). The prevalence of HBV infection was nearly similar to results reported in Shone, Nekemte, Bishoftu, and Felegehiwot referral hospitals 4.9%, 27 5.8%, 28 6.5%, 18 and 4.7% 29 , respectively.
The result of this study was relatively high when compared to the result reported from Addis Ababa at 3.7%, 20 7.8% Southern Ethiopia, 30 Gandhi memorial hospital at 2.3%, 31 Agena health center in the Gurage zone at 4.1%, 32 Uganda at 2.1% 33 , and Rwanda 3.1%. 34 The variation might be due to the differences in cultural practices and strategies used for infection prevention and risky behavior practices. In comparison with other studies done outside African region, the result of the study was higher than the result reported by Pakistan at 2.78%, 35 Turkey at 2.1%, 36 and India at 1.6%. 37 This variation might be due to regular screening and vaccination provided in those countries.
However, the result of this study was lower than the result reported from Gedeo zone at 9.2%, 19 Jigjiga town at 8.5%, 38 Gambella at 7.9%, 39 Yirgalem hospital at 7.2%, 40 Ghana at 7.7%, 41 South Darfur state, Sudan at 8.5% 42 , and Gambia at 9.2%. 43 The variation might be due to the differences in geographical regions, sociodemographic variations, differences in cultural practices, and risky behavior toward the risk of HBV infection.
The odds of HBV infection were about 3 times higher among pregnant mothers who had a history of hospital admission when compared to those who had no history of hospital admission. This result is in line with the study reported from Ambo town, 44 Desie, 45 Gedeo zone, 19 Agena health center, Gurage zone, 32 West Hararghe public hospitals, 46 and Egyptian. 47 This might be due to that the hospitalized women might easily acquire the infection during a different procedure than the pregnant women who had no history of hospital admission.
In this study, pregnant women with traditional tonsillectomy have 4 fold chance to have HBsAg seropositivity compared with their counterparts. The finding of this report is similar to the study conducted in Felegehiwot referral hospital 29 and West Hararghe Public Hospital. 46 This study revealed the traditional surgery of tonsillectomy was done in an area where appropriate sterilization was not followed. Therefore, the virus easily transferred from a career to a healthy woman.
Regarding the history of sexually transmitted infection, women who had a history of sexually transmitted infection were 6 times more likely to have an infection with HBV than those who had no history of sexually transmitted infection. This finding was similar to the study conducted in Jinka Hospital 48 and Harar city. 49 A possible explanation for this occurrence is that HBV and other Sexual Transmit Infection (STI) co-infections can occur since STI and HBV share the same modes of transmission.
The finding of this study revealed that HIV co-infection was highly significantly associated with HBV infection, with HIV-infected women being around 8 times more likely infected by HBV than HIV-non-infected women. The result of this report agreed with the study done in the Gedeo zone, 19 Amhara national regional state hospitals, 50 Dire Dawa, 51 Yirgalem Hospital, 40 and Harar city. 49 The major justification might be explained by their nature of sharing similar modes of transmission.
Pregnant women who had a history of alcohol drinking were about 5 times at higher risk when compared with those who had no history of alcohol drinking. The finding of this report was consistent with the result of a study conducted in Ambo town, 44 Nigeria, 25 and Kenya. 52 The possible explanation for this occurrence might be alcohol intake is associated with risky sexual behavior and chronic alcohol intake has adverse effects on the liver.
Strength and Limitations
The strength of the study was data were collected from clients and it was primary data which increase the completeness and consistency of data. The limitation of this study was due to time and budget constraints, limited to assessing the only prevalence and associated factors. In addition, markers of HBV like hepatitis B envelope antigen (HBeAg), hepatitis B core antigen (HBcAg), anti-Hepatitis B surface (HBs), anti-Hepatitis B envelope (HBe), anti-Hepatitis B core (HBc) nor viral load were detected, due to resource constraints and a wide CI in associated factors due course of a small sample of HBV positive cases.
Conclusion
The prevalence of HBV infection among pregnant women in the study area was intermediate endemic according to WHO classification criteria. Factors such as hospitalization history, previous traditional tonsillectomy, history of sexually transmitted infections, HIV infection status, and alcohol consumption were associated with HBV infection among pregnant women. Healthcare providers have to make effort to implement the infection prevention strategy during admission at the health facility to prevent HBV infection trasmission. The health extension workers should creat awareness on the risk of contact with sexually transmitted infection person, traditional tonsillectomy, and alcohol consumption. The government should provide routine HBV screening for people living with HIV.
Footnotes
Abbreviations and Acronyms
Acknowledgements
First, we would like to acknowledge Bule Hora University for giving us this chance to prepare a research report. Further, we extend our sincere gratitude to the Medical Laboratory Science staff for their timely support and positive approach. We also like to express our thanks to our study participants, Yaballo and Moyale hospital, and Borena Zone Health Office for their cooperation.
Availability of Data and Materials
Data essential to the conclusion are included in this manuscript. Additional data are available upon reasonable request from the corresponding author.
Authors’ Contributions
AK performed conceptualization, developed proposals, resources, project management, research and monitoring, data analysis, and interpretation. MKA, DT, and DD were involved in supervision, performed document preparation and interpretation, and writing. AA, WD, and AE was involved in manuscript preparation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.