
Abstract
Background:
Stinger syndrome frequently occurs in athletes who compete in collision sports. Sharp pain and impairment of neck motion are major symptoms. Cervical intervertebral disc degeneration (CIDD) is also frequently observed in those who compete in collision sports.
Purpose/Hypothesis:
To investigate whether CIDD and neck functionality are related to a history of stinger syndrome. The hypothesis was that a significant relationship exists between CIDD and neck motion and a history of stinger syndrome in Japanese collegiate football players.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 49 male Japanese collegiate football players (mean age, 20.0 ± 1.1 years; mean athletic experience, 3.8 ± 2.3 years; mean height, 172.3 ± 4.8 cm; mean weight, 83.1 ± 12.2 kg) were subdivided into athletes with stinger syndrome (stinger group) and those without (control group). Stinger syndrome was confirmed based on a questionnaire and interview. CIDD was assessed by using T2-weighted magnetic resonance imaging. Range of motion (ROM) and isometric muscle strength were measured for neck function testing.
Results:
Thirty-nine percent (19/49) of athletes had at least 1 episode of stinger syndrome. The prevalence of CIDD was significantly higher in the stinger group (68%) than in the control group (30%) (P < .01). A statistically significant difference in cervical extension ROM was found between the stinger group (50.9° ± 11.1°) and the control group (60.2° ± 11.4°) (P < .01). Logistic regression analysis showed that CIDD and low cervical extension were independently associated with a history of stinger syndrome.
Conclusion:
Study results suggest that stinger syndrome is associated with CIDD and low cervical extension in collegiate football players.
Football is a collision sport that places players at risk of neck injuries. 20,25 Although the incidence rate is low (1.5 per 100,000 players at the collegiate level), 1,20 spinal cord injuries have occurred in football players. Stinger (or burner) syndrome is also known as a common neck injury in collision sports, including football and rugby. 11,12,14,17,20 Although stinger syndrome is not a catastrophic injury, it occasionally needs a prolonged recovery period and will sometimes lead to athletes withdrawing from practices or games. 17 Levitz et al 14 reported that approximately 87% of players have experienced a recurrence of the symptom. In many cases, players with stinger syndrome have continued to participate in competition or practice. Thus, the prevention of stinger syndrome in athletes is important.
A high incidence of degenerative changes in the cervical spine has been reported in front-row rugby players, which suggests that repetitive collision induces spinal deformation. 8 Football is also a collision sport, so players may experience degenerative changes of the cervical disc. Deformation of the cervical structure, such as foraminal stenosis, has been reported to be a risk factor of stinger syndrome. 14,17 Disc disease, a bulging disc, and herniation have also been associated with a history of stinger syndrome, 14 and intervertebral disc degeneration has been reported to be a risk factor of disc herniation. 10 Taken together, cervical intervertebral disc degeneration (CIDD) possibly induces peripheral nerve deformation and results in radiating pain to the upper extremity. However, the association between a history of stinger syndrome and the occurrence of CIDD has not been examined previously. We hypothesized a significant relationship between stinger syndrome and CIDD in football players.
Athletes with stinger syndrome claim to experience sharp pain and a burning sensation of the ipsilateral muscles such as the supraspinalis, deltoid, biceps, and trapezius muscles, concomitant with strength loss. 15 The proposed causes of stinger syndrome are as follows: (1) nerve root compression (ie, cervical extension-compression), (2) a brachial plexus stretch injury, and (3) a direct blow to the plexus. The extension-compression mechanism may particularly be related to the effect of cumulative trauma from minor compression sprains that lead to chronic inflammation. 17 Therefore, cervical functions such as range of motion (ROM) and neck muscle strength of the athlete may be predictive factors of stinger syndrome.
The purpose of this study was to investigate the relationship between CIDD and a history of stinger syndrome. We also examined whether a significant association exists between stinger syndrome and neck functionality such as ROM and strength. The obtained results may be applied during a preseason medical checkup to prevent stinger syndrome.
Methods
Participants
Forty-nine male Japanese collegiate football players participated in this study (mean age, 20.0 ± 1.1 years; mean athletic experience, 3.8 ± 2.3 years; mean height, 172.3 ± 4.8 cm; mean weight, 83.1 ± 12.2 kg). This cohort belonged to the first division of the Japanese collegiate football league. All players spent a total of 3 hours in football training 6 days a week.
The ethical committee of our university approved the protocol of the present study, and all the players provided written informed consent before participation. Information regarding the study’s purpose and any risks, as well as the participants’ rights, was provided to all the players.
Assessment of Stinger Syndrome
A history of stinger syndrome was confirmed based on questionnaire responses and a health record investigation. Stinger syndrome was defined as an episode of numbness or sharp or burning pain from the neck to the hand resulting from a collision in the past year. 12 We excluded players who had sharp and burning pain closer to the neck than the shoulder. In the questionnaire, we used images of parts of the human body to describe sharp or burning pain at the time of injury. Recurrence and injury status were also evaluated. Results of the questionnaire led to the categorization of the players into 2 groups: a stinger group (n = 19) and a control group (n = 30). We classified a participant into the stinger group if he had ≥1 stinger episodes in the past year.
Assessment of CIDD
Magnetic resonance imaging (MRI) (AIRIS II; Hitachi) was performed using a 0.3-T unit with surface coils with the patient in the supine position. The following T2-weighted sequence was used: spin echo with a repetition time of 2000 milliseconds, echo time of 120 milliseconds, thickness of 50 mm, matrix of 256 × 256, and field of view of 250 mm. Five cervical discs from C2/C3 to C6/C7 were scanned (Figure 1). The severity of lumbar disc degeneration was graded as 1 to 5 in accordance with the classification of Pfirrmann et al. 19 We defined CIDD to be Pfirrmann grades of ≥3 based on a previous study. 19 Two orthopaedic surgeons specializing in spine disorders assessed the scans; they were blinded to the injury.

Magnetic resonance imaging of the intervertebral disc of a football player with grade III cervical intervertebral disc degeneration of C5/C6 (arrow).
Cervical Function
For the cervical function assessment, cervical ROM and isometric muscle strength testing was performed. Measurements were taken after the season, and participants were asymptomatic during the measurements. To minimize interexaminer variation, a single examiner (T.H.) made all measurements. The examiner was blinded to the participants’ medical history and MRI findings. Measurements were performed 2 times, and averaged values were used.
ROM included flexion, extension, lateral flexion, and rotation in the sitting position before stretching with the use of a standard goniometer. 5 Cervical ROM was measured in a standardized sitting position to remove errors and compensate for movement. The participant’s ankles, knees, and hips were positioned at the desired angle, and arms were folded across the chest to minimize thoracic movement.
For muscle strength testing, the flexion, extension, and lateral flexion in the supine, prone, and lateral positions were measured with a handheld dynamometer (MicroFET 2; Hoggan Health). 26 At the start of the measurement, the chin was fully pulled downward, and the line between the earlobe and acromion was horizontal to the ground (Figure 2). The handheld dynamometer was vertically pushed for 5 seconds and used to measure isometric muscle strength. The measurement was calculated 3 times for each direction. The average strength was divided by the body weight to obtain relative isometric muscle strength. Participants were not informed of the MRI results.

For the start position of the measurement in the cervical muscle strength test, the chin is pulled downward.
Statistical Analysis
The Student unpaired t test was used for statistical analysis of cervical function between the stinger and control groups. The prevalence rates of stinger syndrome and CIDD were compared between the 2 groups by using the chi-square test. In addition, logistic regression analyses were performed to investigate whether CIDD and cervical function were independently associated with stinger syndrome. A P value of <.05 was considered statistically significant. All statistical analyses were performed by using SPSS 22.0 for Macintosh (IBM). We also calculated the effect size (ES) for each group and parameter. According to Cohen, 4 ESs of 0.2, 0.5, and 0.8 are considered small, medium, and large, respectively. In addition, the phi and Cramer V correlations were used to assess the significance of predictors. According to Cohen, 4 ESs of 0.1, 0.3, and 0.5 are considered small, medium, and large, respectively.
Results
Thirty-nine percent of the participants had a history of stinger syndrome (≥1 stinger episodes; 19/49). No significant differences in the demographic profile (height, weight, age, athletic experience, and body mass index) were found between the stinger and control groups (Table 1). Of the 26 offense and 23 defense players in this study, we found that 5 offense and 14 defense players suffered from stinger syndrome. The recurrence rate within the past year was 84% in the stinger group.
Demographic Profile of Football Players a

a Data are shown as mean ± SD. There were no statistically significant differences between groups (P ≥ .05, unpaired t test).
In addition, we evaluated 245 cervical intervertebral discs (C2-C7) and found that 15.5% (38/245) were degenerated. All degenerated discs were grade 3 according to the Pfirrmann classification (Table 2). With regard to the spine level of the lesion, 61% (23/38) of the CIDD cases were observed in the lower discs (C5/C6 and C6/C7) (Table 3). Some participants had multiple areas of CIDD at different levels of the cervical disc, which we defined as a single incidence. Of the 49 participants, 22 (45%) had CIDD in at least 1 area of their spine.
Severity of Cervical Intervertebral Disc Degeneration a
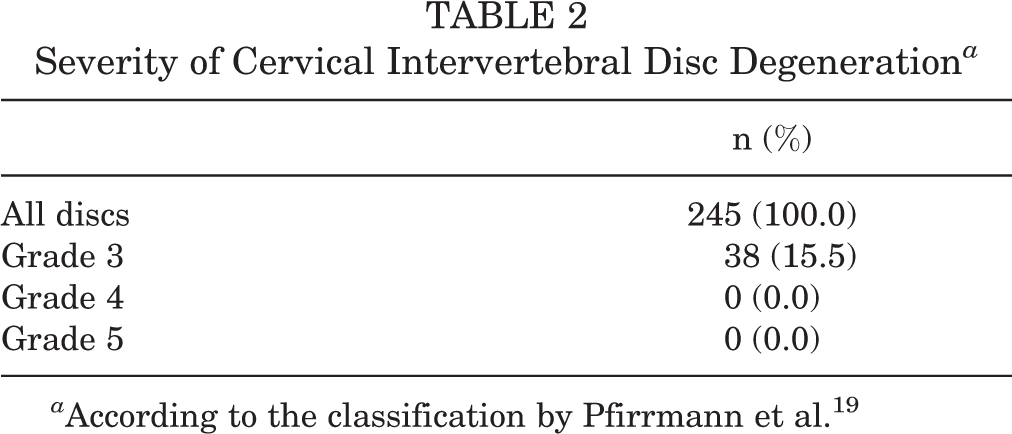
a According to the classification by Pfirrmann et al. 19
Location of Cervical Intervertebral Disc Degeneration

Table 4 shows the prevalence of stinger syndrome in the players with CIDD and those without CIDD. Among the 22 athletes with CIDD, 13 (59%) had stinger syndrome. Of the 27 athletes without CIDD, only 6 (22%) had stinger syndrome. The incidence of CIDD was significantly higher in the stinger group, as determined by chi-square test (P < .01, Cramer V = 0.38).
Prevalence of CIDD Associated With Stinger Syndrome a

a CIDD, cervical intervertebral disc degeneration.
Table 5 shows the cervical ROM and isometric muscle strength results of the 2 groups. A statistically significant difference (P < .01, ES [d] = 0.83) in cervical extension ROM was found between the stinger (50.9° ± 11.1°) and control groups (60.2° ± 11.4°). The extension decrement of the stinger group was 10°. Conversely, no significant statistical difference in isometric muscle strength was found between the groups. The test-retest reliability is shown in Table 6. The intraclass correlation coefficient values ranged from 0.99 to 0.84, suggesting that the measurement methods used in this study are highly reproducible.
Range of Motion and Isometric Muscle Strength Data a

a Data are shown as mean ± SD unless otherwise specified. NS, not significant.
Intrarater Reliability of the Cervical Function Test a
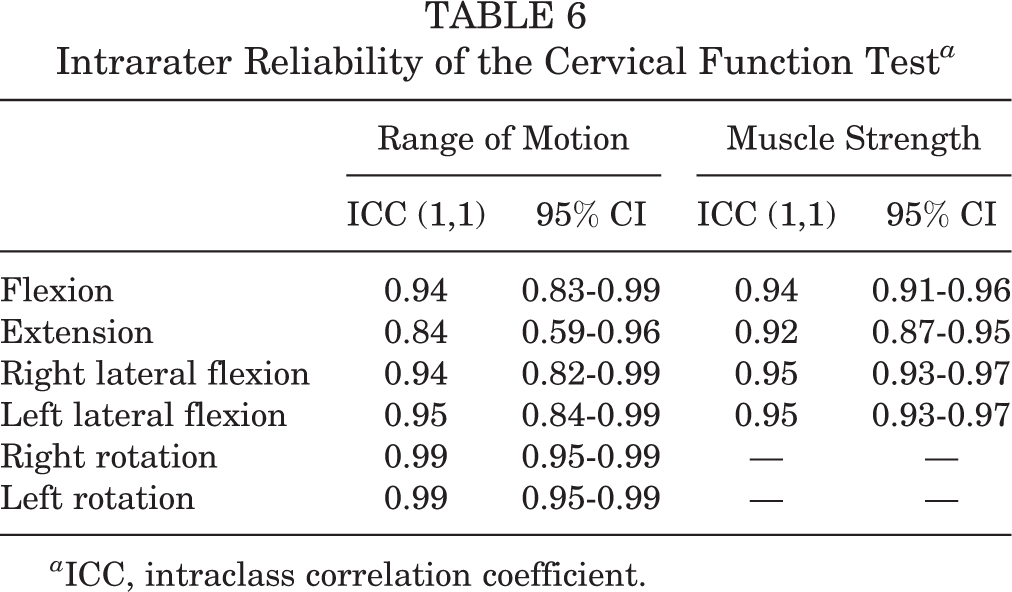
a ICC, intraclass correlation coefficient.
By using logistic regression analysis, we further examined significant predictive factors. We confirmed that CIDD (adjusted odds ratio [OR], 5.58; 95% CI, 1.43-21.76) and decreased cervical extension ROM (adjusted OR, 0.93; 95% CI, 0.87-0.99) were independently associated with stinger syndrome (Table 7).
Logistic Regression Analysis of Football Players With Stinger Syndrome a
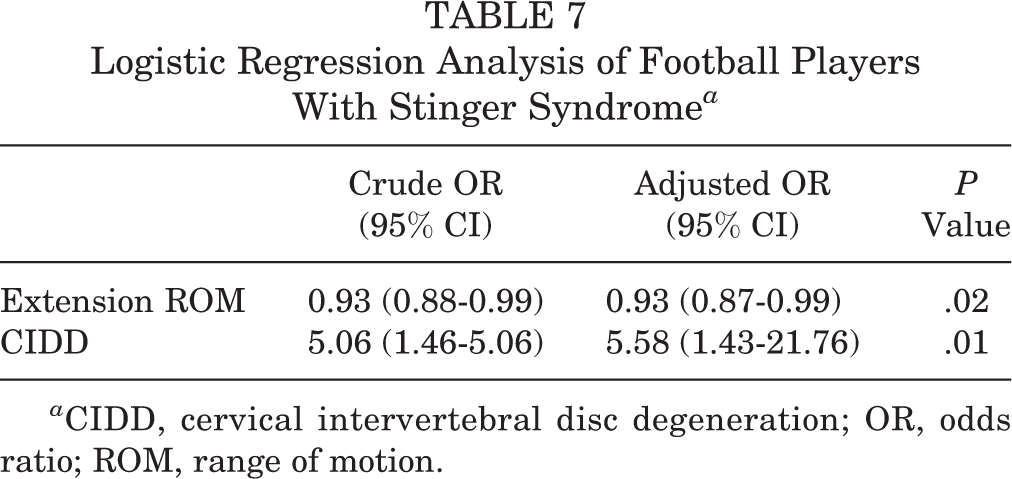
a CIDD, cervical intervertebral disc degeneration; OR, odds ratio; ROM, range of motion.
Discussion
Stinger syndrome is a type of neurapraxia of the cervical roots or a brachial plexus nerve injury 11,20 and is common in contact sports such as football. In this study, we found a significant association of CIDD and lower cervical extension with stinger syndrome in Japanese collegiate football players. Furthermore, logistic regression analyses revealed that CIDD and decreased cervical extension ROM were independently associated with stinger syndrome.
We found that 39% of the players had stinger syndrome. Previous studies have reported that 50% to 65% of collegiate football players had stinger syndrome, 3,21 thus incidence rate in this study was lower than those in previous studies. The athletic experience of the participants (>4 years) in previous studies was longer than that in this study (3.9 years). 20,21 Moreover, our study participants are considered to be much smaller in height and body weight than collegiate football players in America. In addition, in previous studies, participants with stinger syndrome were selected based on medical records. 12,14,17 Conversely, in the present study, stinger syndrome was evaluated by using a questionnaire and interview. Therefore, the lower incidence of stinger syndrome in this study was mainly because of the relative lack of athletic experience of the target participants.
In this study, the Pfirrmann classification 19 was used for assessing CIDD. In general, the Pfirrmann classification is used for assessing the severity of disc degeneration in the lumber spine. Low signal intensity and disc height on T2-weighted MRI are the criteria for the Pfirrmann classification; thus, it is applicable for CIDD. In a recent study, Oh et al 18 used the Pfirrmann classification for cervical MRI findings and successfully assessed CIDD. Similarly, we also assessed CIDD in accordance with the Pfirrmann classification and found that 45% of athletes had CIDD. Although using a different classification system, Matsumoto et al 16 investigated CIDD in patients without neck pain and cervical injuries. They used T2-weighted MRI and found that in 20- to 29-year-old patients, 17% of discs in men and 12% of discs in women were degenerated. 16 The frequency of CIDD increases depending on age, 9,16 so the CIDD occurrence rate should be 15% to 18% in patients in their 20s.
We also found that C5/C6 was the most damaged disc. When the cervical spine axially directs energy input by “spearing tackles,” a compression power by axial loading is thought to increase, and C3/C4 is easily injured. 24 We conclude that external stress (hyperextension, hyperflexion), other than axial pressure, might induce C5/C6 CIDD.
The main finding of this study was that CIDD was significantly associated with stinger syndrome in football players. The prevalence of CIDD in players who experienced stinger syndrome was 68% in this study. Although this is only an association, there are several possible mechanisms by which CIDD induces stinger syndrome. Risk factors of CIDD are repeated crash forces when the athletes are subjected to contact and external stressors. 8 In this study, external stress was caused by contact-induced cervical degeneration. As a result, a higher occurrence of CIDD was observed in the athletes with stinger syndrome than in those without stinger syndrome. CIDD is accompanied by intervertebral foraminal stenosis 12,14,22 ; thus, we believe that the surrounding tissues such as the cervical nerve root were deformed. Stinger syndrome is accompanied by nerve symptoms such as numbness and pain, so nerves deformed by CIDD might be easily damaged by external stress.
We performed muscle strength and ROM measurements to assess cervical function. Weaker neck muscle strength and smaller cervical ROM are considered to be characteristic clinical signs in patients with neck pain versus those without neck pain. 13,23 In addition, a history of stinger syndrome has been associated with neck pain. 6 In the present study, we found that cervical extension ROM in the stinger group was significantly lower than that in the control group. The “head-up” technique is highly recommended for football players to prevent a catastrophic injury of the cervical vertebral disc at the time of contact. 2,7 Although this technique can protect the hyperextension load of the neck by contraction of the deep cervical flexor muscles, our findings suggest that repeated contact might decrease low cervical extension ROM. Moreover, logistic regression analyses revealed that CIDD and low cervical extension ROM were independently associated with stinger syndrome. From the results of this study of stinger syndrome, CIDD and cervical extension ROM were independent factors, but all of these conditions (tackling position, repeated contact) should be considered as risk factors.
This study suggests that MRI and physical examinations are important for the prevention of cervical diseases such as stinger syndrome. If either CIDD or a decrease of cervical extension ROM can be confirmed, we may be able to prevent stinger syndrome by improving the tackling technique. Although increasing the muscle strength of the neck is generally recommended for the prevention of stinger syndrome, in this study, we found no difference in neck muscle strength between the stinger and control groups. Because there are several limitations, as discussed below, further studies with a large cohort and longitudinal design might provide contributions of neck muscle strength for the prevention of stinger syndrome.
This study had several limitations. First, its cross-sectional design could not support any claims of causality. Second, the sample size was relatively small. Third, stinger syndrome was defined based on a questionnaire and a health record investigation. We should also consider that there are 3 possible mechanisms for stinger syndrome—disc degeneration, spinal cord or root encroachment, and a soft disc or foraminal stenosis—although disc degeneration and spinal stenosis might be related to spinal cord or root encroachment. 22 Although these limitations exist, we still suppose that the pre-existence of CIDD and cervical extension ROM may be predictive factors of stinger syndrome.
Conclusion
The results of this study suggest that CIDD and low cervical extension are associated with stinger syndrome in collegiate-level football players. We believe that additional studies with a longitudinal design and other factors are needed to establish possible risk factors for stinger syndrome.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the ethics committee of Nippon Sport Science University.