
Abstract
Study Design
Systematic review
Objective
Examine the clinical evidence for the use of osteobiologics in hybrid surgery (combined anterior cervical discectomy and fusion (ACDF) and total disc replacement (TDR)) in patients with multilevel cervical degenerative disc disease (DDD).
Methods
PubMed and Embase were searched between January 2000 and August 2020. Clinical studies investigating 18-80 year old patients with multilevel cervical DDD who underwent hybrid surgery with or without the use of osteobiologics were considered eligible. Two reviewers independently screened and assessed the identified articles. The methodological index for non-randomized studies (MINORS) tool and the risk of bias (RoB 2.0) assessment tool were used to assess risk of bias. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) was used to evaluate quality of evidence across studies per outcome.
Results
Eleven studies were included. A decrease in cervical range of motion was observed in most studies for both the hybrid surgery and the control groups consisting of stand-alone ACDF or TDR. Fusion rates of 70-100% were reported in both the hybrid surgery and control groups consisting of stand-alone ACDF. The hybrid surgery group performed better or comparable to the control group in terms of adjacent segment degeneration. Studies reported an improvement in visual analogue scale for pain and neck disability index values after surgery compared to preoperative scores for both treatment groups. The included studies had moderate methodological quality.
Conclusions
There is insufficient evidence for assessing the use of osteobiologics in multilevel hybrid surgery and additional high quality and controlled research is deemed essential.
Keywords
Introduction
Cervical degenerative disc disease (DDD) is commonly seen in clinical practice and is known to progress over time. Cervical DDD can cause pain and/or neurological deficits and thus seriously impact quality of life. 1 Anterior cervical discectomy and fusion (ACDF) is a well-established and effective surgical technique for treating cervical DDD.2-4 However, in case of multilevel cervical DDD, it has been suggested that multilevel fusion could be disadvantageous due to the range of motion constraints and the potential to induce adjacent segment degeneration (ASD) in an accelerated manner. 4
Total disc replacement (TDR), also known as cervical disc arthroplasty (CDA), has commonly been used as an alternative to ACDF. TDR aims to maintain cervical range of motion (ROM) of the affected segments and consequently reduces ASD. 5 In case of multilevel cervical DDD, however, TDR is related to a higher risk of disc prosthesis complications and increased medical costs compared to ACDF. As a result, performing multilevel TDR can be less feasible in clinical practice.4-7
With the purpose to overcome these challenges in multilevel cervical DDD, hybrid surgery (combining ACDF and TDR), has been introduced. Hybrid techniques aim to combine the most effective elements of both surgical interventions. Thereby, the degenerative status of each cervical level can be considered individually with the aim of maintaining sufficient cervical ROM as well as sufficient stability of the cervical spine.4,8 When stabilizing a cervical level, it is essential to attain a decent fusion, as high rates of radiological fusion correlate with improved postoperative outcomes. 9 The rate of fusion can be stimulated by the use of bone grafts or osteobiologics. Although autologous bone grafts are considered the ‘gold standard’, there are inherent disadvantages such as complications that may occur at the donor site (pain, hematoma, fracture), prolonged operation time, and limitations in availability.10,11 Allografts may tackle these disadvantages but are associated with a higher risk of infections or immunogenic rejection as well as lower donor graft quality. Moreover, allografts do not contain osteogenic properties. 10
There is growing evidence for the use of osteobiologic graft substitutes to surmount these limitations. Osteobiologic graft substitutes are a group of synthetic biomaterials that mimic the desired traits of osteoinductivity, osteoconductivity and osteogeneity in varying degrees. Thus, they are often applied to promote spinal fusion as well as to provide structural support.10,12 Common osteobiologic graft substitutes include ceramics, polymers, bioactive peptides, bone morphogenetic proteins (BMPs) and demineralized bone matrix (DBM). The use of osteobiologics, as bone graft extender and as stand-alone bone graft substitute is rapidly expanding.10,11,13 The properties of osteobiologics determine its effectiveness as bone graft substitute. The type of bone graft may be essential for the extent of bone growth at the fused level and consequently may impact the overall effectiveness of hybrid surgery. Therefore, the objective of this systematic review was to determine the evidence for the use of osteobiologics in hybrid surgery in patients with multilevel cervical DDD.
Methods
Protocol Registration
This study was registered in the International prospective register of systematic reviews (PROSPERO) under the registration number: CRD42020209665. This manuscript has been written according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 14 A PRISMA checklist is provided in Supplementary Appendix I.
Eligibility Criteria
Studies investigating patients aged between 18 and 80 years, suffering from degenerative cervical discs who had undergone multilevel (2-4 levels) hybrid surgery with or without osteobiologics were considered eligible. Peer-reviewed articles of randomized or non-randomized controlled trials, cohort studies, and prospective case series (n > 20) were included. Articles published before the year 2000 were excluded. The main outcome of interest was radiographical assessment of the cervical ROM. Studies including participants with a history of tumours, infection, spinal cord injury, trauma/fracture, scoliosis, or cervical deformity were excluded. Additionally, studies looking solely at anterior/posterior cervical fusion, anterior cervical corpectomy and fusion (ACCF), or cervical disc replacement were excluded.
Information Sources and Search
The literature search was conducted in PubMed and Embase on August 18, 2020. MeSH terms used in the search were herniation; neck; discectomy; total disc replacement; hybridization; surgery; surgical procedures, operative; general surgery; arthroplasty; intervertebral disc; bone matrix; bone transplantation; autologous graft; ilium; allografts; bone marrow; range of motion, articular. Additional keywords used were anterior cervical discectomy and fusion; ACDF; total disc replacement; TDR; hybrid surgery; osteobiologics and radiographic assessment. Limits applied to the search were human, English or Dutch language, full text, and publication year from 01-01-2000. The detailed search strategy is described in Supplementary Appendix II.
Study Selection
Retrieved articles were screened on title/abstract and subsequently the full text of eligible articles was obtained and screened. This was performed by two reviewers (TH, PW) independently. In case of inconsistency between the two reviewers, a third reviewer (CA) was used to reach consensus. References of full text articles were screened for supplementary studies.
Data Collection Process and Data Items
Data was extracted using a standardized excel format. Two independent reviewers (TH, PW) obtained general characteristics and research specific data of the included studies. The following general characteristics were collected: first author, publication year, country, study design, hybrid construct, surgical control, number of affected levels, number of operated levels, disc/cage, biologic, sample size, diagnosis, gender, mean age, and length of follow-up as well as information on funding and conflict of interest. The following radiological and clinical outcomes were collected: cervical ROM, fusion rate, ASD, postoperative complications, visual analogue scale (VAS) score, neck disability index (NDI) and Odom criteria.
Risk of Bias
Risk of bias was assessed by two independent reviewers (TH, PW) using the methodological index for non-randomized studies (MINORS) tool and the risk of bias (RoB 2.0) assessment tool.15,16 The global ideal score for the MINORS is 24 for comparative studies and 16 for non-comparative studies. The scores obtained with the MINORS tool can further be interpreted in the following manner for comparative studies: 0-6: very low quality; 7-12: low quality; 13-18: moderate quality and 19-24: high quality and for non-comparative studies: 0-4: very low quality; 5-8: low quality; 9-12: moderate quality and 13-16: high quality.17,18 Risk of bias across studies was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach independently by two reviewers. A third reviewer (CA) was consulted to reach consensus in case of inconsistency between the two reviewers.
Results
Study Selection
85 articles were retrieved during the initial search. After removal of duplicates, 84 articles were screened on title and abstract. Consequently, 66 articles were excluded from further analysis. After assessing the full text articles on eligibility and screening the references for additional studies, 11 articles were included in the study. (Figure 1) PRISMA flowchart study inclusion. Abbreviations: ACCF, anterior cervical corpectomy and fusion; ACDF, anterior cervical discectomy and fusion.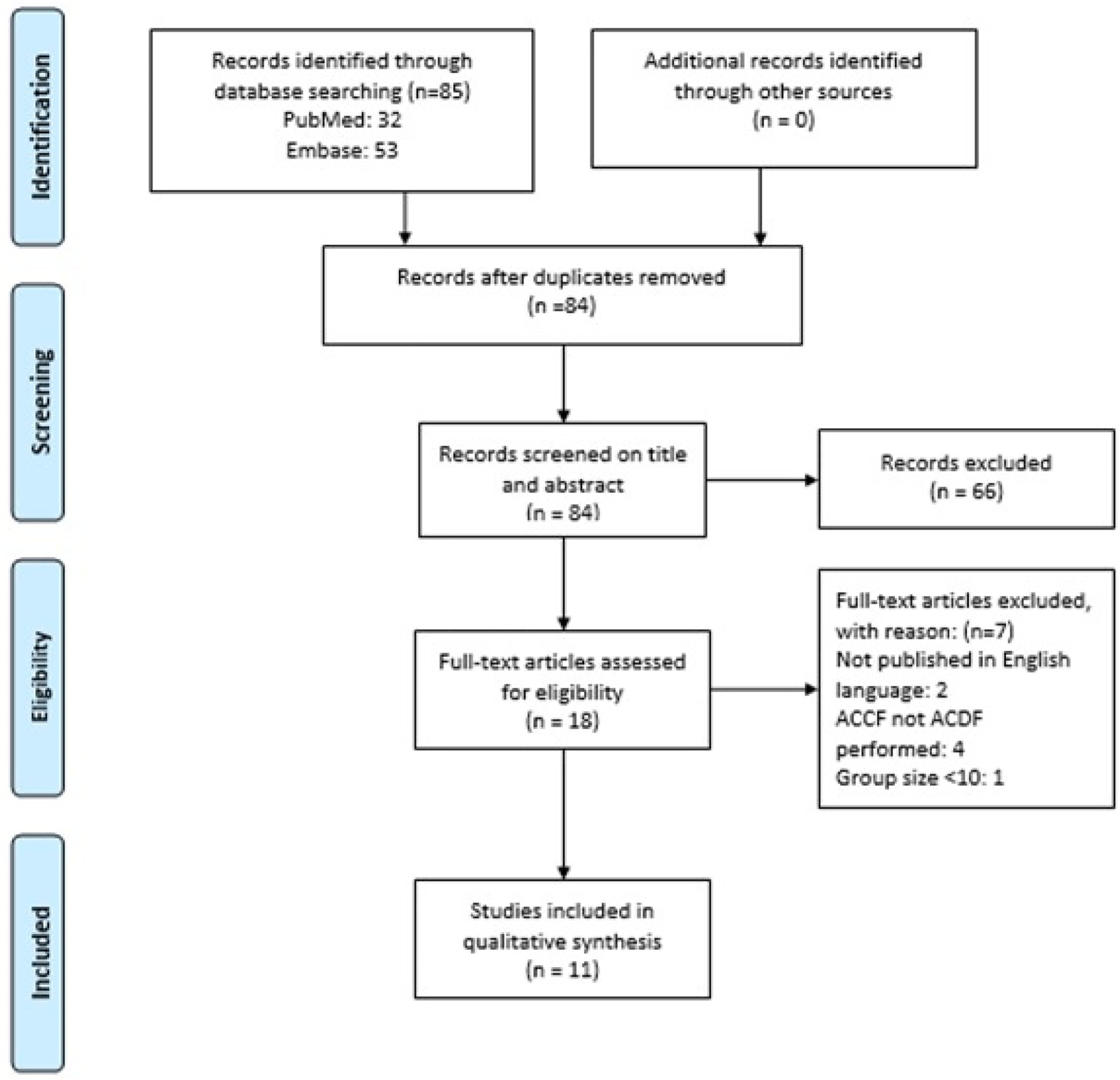
Study Characteristics
Characteristics of Included Studies.
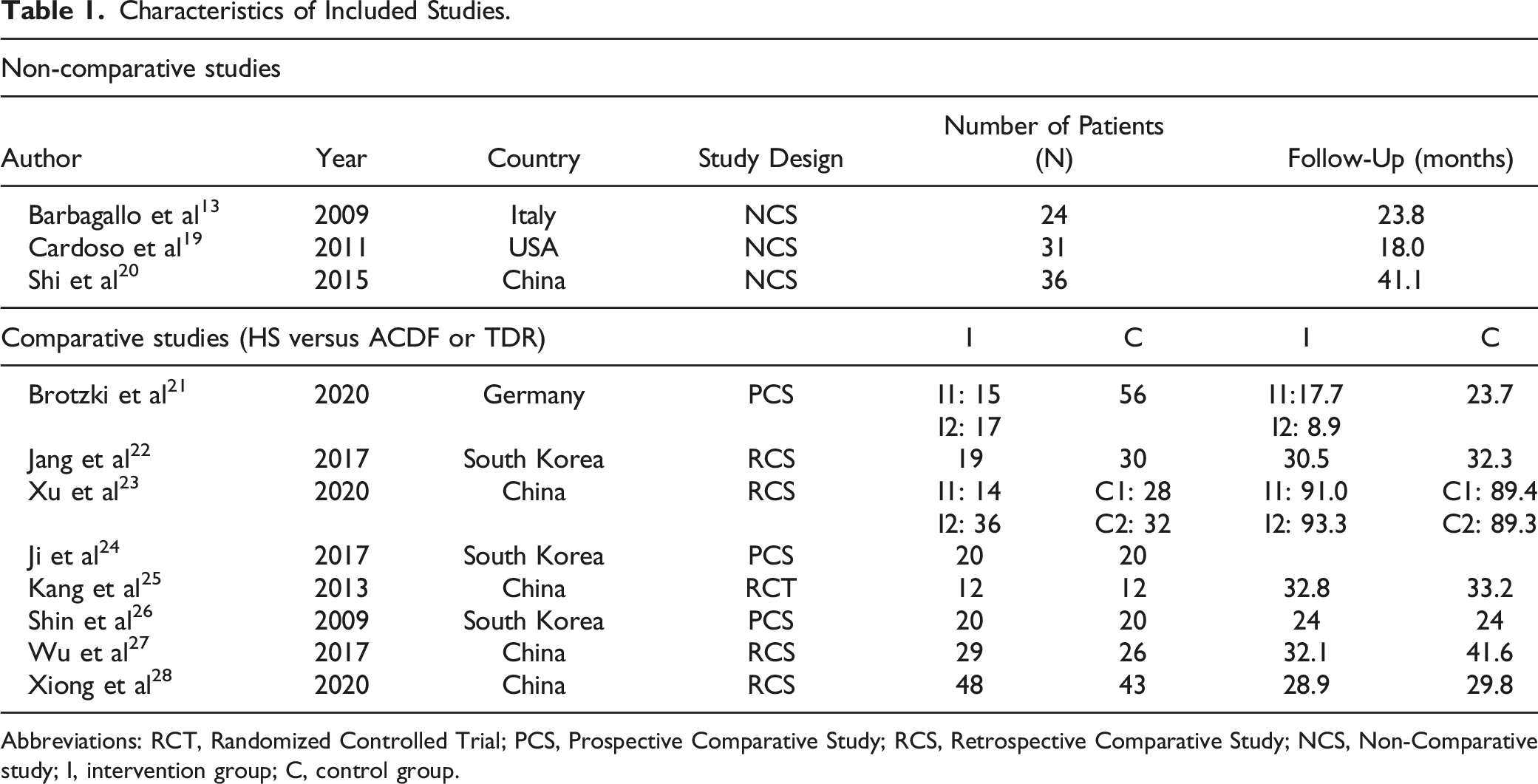
Abbreviations: RCT, Randomized Controlled Trial; PCS, Prospective Comparative Study; RCS, Retrospective Comparative Study; NCS, Non-Comparative study; I, intervention group; C, control group.
The selected studies included a total of 588 patients. All comparative studies included sample sizes of more than 10 participants per group and the included prospective case series had sample sizes of above 20 participants. The follow-up period ranged from 8.9 to 93.3 months in the included studies. On average, studies had a minimal follow-up time of 24 months which was deemed as adequate to determine the outcomes of interest.
Osteobiologics
In four studies the use of osteobiologics as part of the surgical intervention was not reported.20-23 Authors were contacted for more information, but no additional information was obtained. The type of osteobiologic that was used varied among the studies, but the most common type among the control groups was an autologous iliac crest graft. DBM and beta-tricalcium phosphate as well as allogeneic bone were additionally found within the control groups. The type of osteobiologic within the intervention groups varied widely eg, DBM, BMP-2, bovine bone, beta-tricalcium phosphate, allogeneic bone and autologous graft. The surgical construct used by the included studies is described in Supplementary Appendix III.
Qualitative Review
A qualitative description of the radiological and clinical outcomes are presented in Supplementary Appendix IV and V. The included studies prohibited quantitative assessment of the effect of osteobiologics in hybrid surgery since the methodological design and the heterogeneity of the studies did not allow for direct assessment of the research question.
Radiological Outcomes
Differences were seen in the direction and significance of change when looking at the cervical ROM (C2-C7). Studies mostly reported decreased cervical ROM postoperatively relative to preoperative measurements for both the hybrid surgery and ACDF groups.19,20,22,23 Jang et al observed a significant difference between the ROM between the hybrid surgery and ACDF group 6 months postoperatively. The hybrid surgery group showed a faster recovery and reached a ROM closer to the preoperative value. Shi et al reported a significant cervical ROM limitation up to 6 months surgery after surgery. However, this was reversed at last follow-up since the cervical ROM showed a slight but insignificant increase compared to preoperative measurements.
Five studies reported fusion rate in a quantitative manner and two studies qualitatively.19-22,24,27,28 Studies reporting quantitative fusion rates found rates ranging between 70 and 100%, whereas Shi et al and Brotzki et al reported satisfactory fusion and the presence of fusion in ACDF in a qualitative manner, respectively. Jang et al was the only study to report a statistically significant difference in fusion rate between patients who underwent hybrid surgery compared to ACDF but the use of osteobiologics was not specified.
Six comparative studies assessed ASD.21-23,25,27,28 Brotzki et al reported that the hybrid surgery group produced the best results; the increase of ASD on the Kellgren-Lawrence score was smallest and not significant at final follow-up in the hybrid group compared to preoperative scores. This is supported by Jang et al who found that radiographic ASD presented more frequently in the ACDF group compared to the patients undergoing hybrid surgery, and by Kang et al who reported one case of ASD requiring revision surgery in the ACDF group but no cases in the hybrid surgery group. However, Xiong et al and Xu et al reported that there were no statistically significant differences in ASD between the hybrid surgery and control group.
The rate of subsidence was assessed in two studies.25,28 Kang et al detected asymptomatic implant subsidence in one control participant who underwent arthrodesis with a cervical plate system and an autogenous iliac-crest graft, but this required no further intervention. Xiong et al found a subsidence rate of 27% in the participants receiving hybrid surgery compared to 37% in participants who underwent multilevel ACDF. However, the subsidence difference between the two groups was not statistically significant.
Postoperative complications included dysphagia, heterotopic ossification and complications related to prosthesis or cages.13,19-25,27,28 Jang et al noted that the group receiving hybrid surgery experienced lower incidences of complications compared to the control group and Ji et al indicated that lower heterotopic ossification rates were found in the hybrid surgery group. However, Xiong et al found more complications in the hybrid surgery group compared to the ACDF group.
Clinical Outcomes
Brotzki et al showed that the hybrid surgery group had the greatest reduction in arm pain VAS score compared to the patients receiving a dynamic cervical implant or ACDF. Jang et al found that there was a significant decrease in arm pain on VAS in both the hybrid and ACDF group but no statistically significant difference between the two groups was noted 24 months after surgery. Similarly, three studies concluded that there were no statistically significant differences in VAS scores between the hybrid surgery and control group.25,27,28 On the contrary, Ji et al and Shin et al found that the hybrid surgery group had less postoperative neck pain compared to the control group (P < .05).
All ten studies assessing NDI presented improvement compared to preoperative values.13,20-28 Brotzki et al showed that improvement was significantly greater in the hybrid group. This was supported by findings from Xu et al, Ji et al and Shin et al. However, Wu et al, Xiong et al and Kang et al found that there were no statistically significant differences in NDI values between the respective intervention and control groups.
Jang et al was the only study to assess the Odom criteria, which is used to determine general clinical outcome after surgery. The authors concluded that there was significant improvement in both groups, but no statistically significant differences between groups (P > .05).
Risk of Bias Assessment
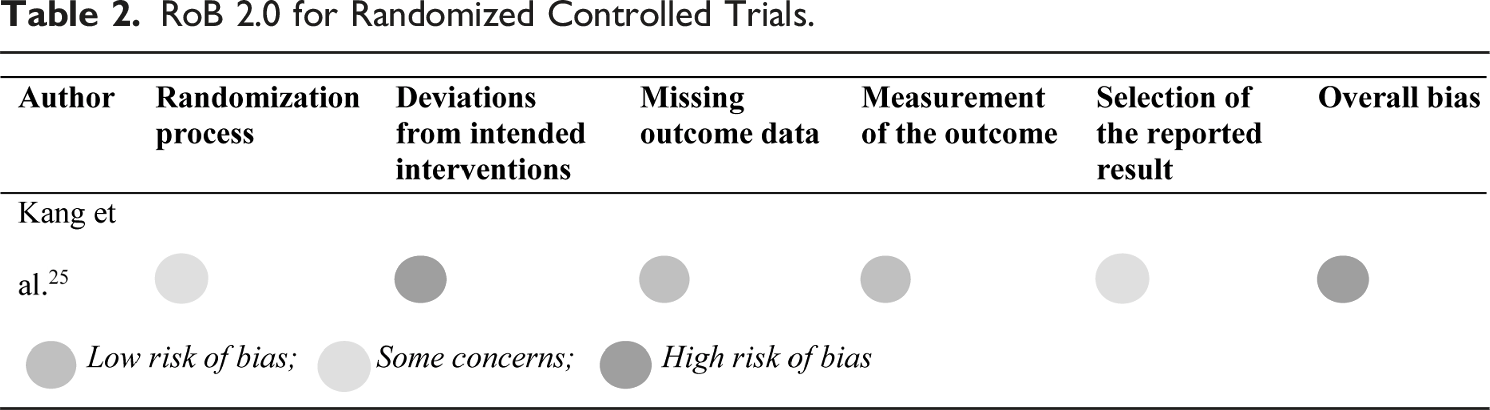
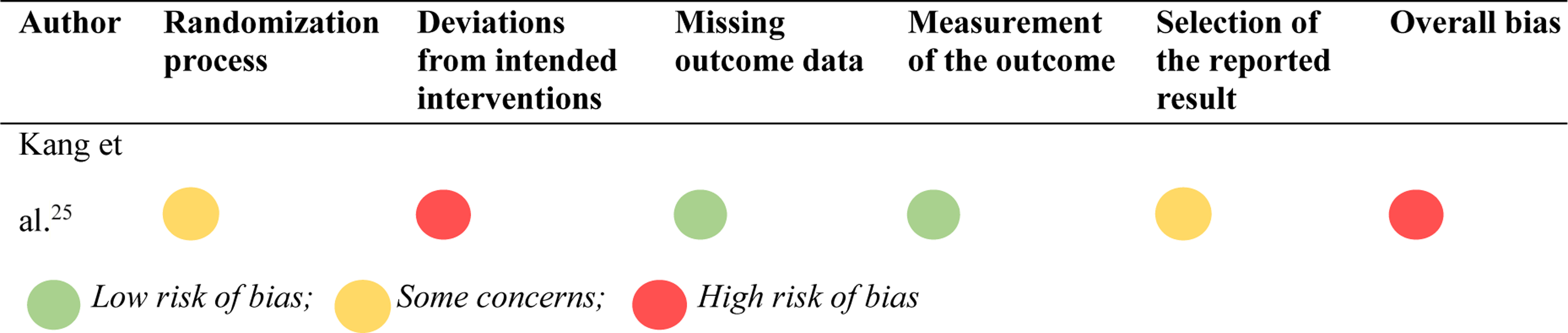
RoB 2.0 for Randomized Controlled Trials.
MINORS Tool for Non-Randomized Studies.
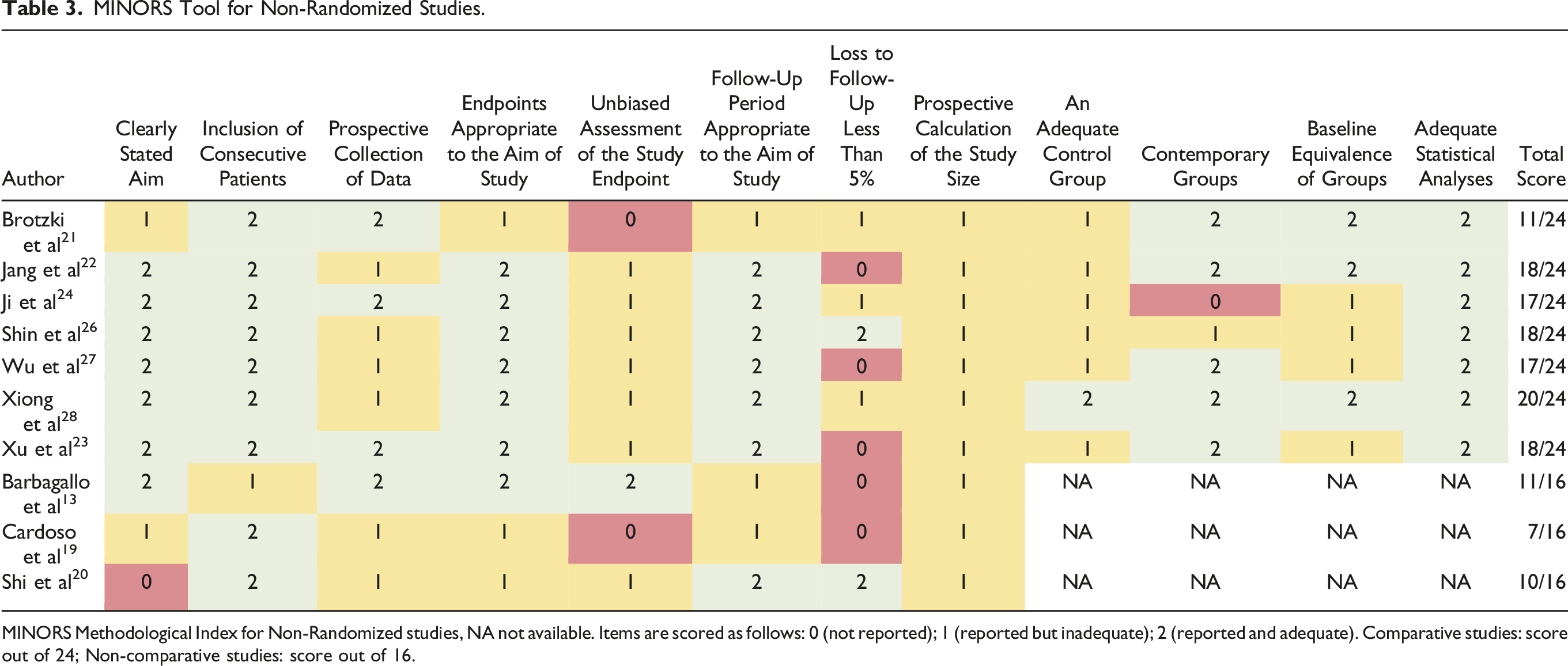
MINORS Methodological Index for Non-Randomized studies, NA not available. Items are scored as follows: 0 (not reported); 1 (reported but inadequate); 2 (reported and adequate). Comparative studies: score out of 24; Non-comparative studies: score out of 16.
Methodological Quality of Evidence
The GRADE procedure used to assess the quality of evidence across studies per outcome could not be performed due to the heterogeneity in studies and consequently the lack of pooled outcomes.
Discussion
This study investigated the evidence for the use of osteobiologics in multilevel hybrid surgery for cervical DDD. Although studies reported the use of osteobiologics, no studies were identified that directly investigate the role of osteobiologics in hybrid surgery. Rather, studies reporting the use of osteobiologics looked at the effectiveness of hybrid surgery compared to stand-alone ACDF or TDR. Consequently, the heterogeneity in study design, methodological quality and outcome measures prohibited pooling of study results. Therefore, a qualitative review of the radiological and clinical outcomes was presented.
Radiological/Clinical Outcomes
A decreased cervical ROM was seen in most studies for both the hybrid surgery and the control group.19,20,22,23 In general, the fusion rates reported were adequate and only one study reported a statistically significant difference in fusion rates in favour of the hybrid surgery group compared to the ACDF group. 22 Of the six studies investigating ASD, three studies reported that the hybrid surgery group performed better than the control group.21,22,25 The rate of subsidence was lower in the hybrid surgery group, but this was only assessed by two studies.25,28 Postoperative complications were noted in varying degrees in both the hybrid surgery and control group.13,19-28 Overall, studies reported an improvement in VAS pain scores and NDI values after surgery compared to preoperative scores.13,20-28 However, studies varied greatly on whether the reported changes were statistically significant between the hybrid surgery and control group.
Limitations
This systematic review has several limitations. Firstly, this review is limited by the quality of evidence currently available in the literature. Secondly, no studies could be identified that directly assessed the use of osteobiologics in hybrid surgery. Thus, indirect inferences had to be made, weakening the strength of the evidence found, and prohibiting the pooling of data. Thirdly, language restrictions were applied which potentially could have led to a loss of information considering the majority of included studies were conducted in Asia. Lastly, length of follow-up, study design and outcome measures varied greatly among the included studies, which could explain the heterogeneity in the reported outcomes.
Reduced overall cervical alignment but greater cervical ROM after TDR compared to ACDF has been reported. 29 Furthermore, literature indicates the importance of mechanical stability and stimulation for osseointegration.21,30,31 Considering the differences in physiological movement of the spine when comparing ACDF to TDR, it is assumed that hybrid constructs may lead to altered biomechanical dynamics of the spine as compared to ACDF alone. 21 This altered biomechanical state may in turn influence bone regeneration and osteobiologic ingrowth. 30 Thus, to definitively determine the effectiveness of osteobiologics in cervical hybrid surgery, there is a need for high-quality prospective controlled, preferably multicentre randomized trials, with a long-term follow-up (minimum of 24 months) in patients treated by hybrid surgery, comparing different osteobiologics or comparing osteobiologics to autologous bone graft. Additionally, analysis of adjacent level disease, subsidence of the construct and patient-related outcome measures should be included. Furthermore, future studies should focus on the positioning of TDR in the hybrid surgery construct (lower, middle or upper position of the treated levels) and the necessary parameters to indicate the TDR. At present, there is only one randomized controlled trial available of low methodological quality. Additionally, studies should aim to assess endpoints in a blinded manner. Although blinding may be difficult in surgery, outcome assessment on intervention and control patient groups that received surgery can be done by independent assessors that have no prior knowledge of the prescribed treatment and type of osteobiologic used. Furthermore, conformity regarding validated, preferably quantifiable outcome measures is also essential to pool studies in future reviews. Financial aspects related to the use of osteobiologics were beyond the scope of this review. However, there are increased costs related to using biomaterials other than autologous grafts considering material costs as well as personnel costs associated in addition to longer operation times. Thus, research considering the cost-effectiveness of the use of osteobiologics is warranted.
Conclusions
As of now, there is insufficient clinical evidence to assess the use of osteobiologics in multilevel hybrid surgery. Currently, no studies were identified that directly investigated the role of osteobiologics in hybrid surgery and the available evidence is of low methodological quality. Additionally, there is no consistency in the published results regarding the outcome measures. Hence, there is a need for focused high quality, randomized controlled studies with adequate follow-up time to determine whether the use of osteobiologics is advantageous and cost-effective in hybrid surgery for the treatment of multilevel cervical DDD.
Supplemental Material
Supplemental Material - The Evidence for the Use of Osteobiologics in Hybrid Constructs (Anterior Cervical Discectomy and Fusion and Total Disc Replacement) in Multilevel Cervical Degenerative Disc Disease: A Systematic Review
Supplementary Material for The Evidence for the Use of Osteobiologics in Hybrid Constructs (Anterior Cervical Discectomy and Fusion and Total Disc Replacement) in Multilevel Cervical Degenerative Disc Disease: A Systematic Review by Thomay-Claire A. Hoelen, Paul C. Willems, Arjan Loenen, Hans-Jorg Meisel, Jeffrey Wang, Amit Jain, Zorica Buser, Jacobus J. Arts, and AO Spine Knowledge Forum Degenerative in Global Spine Journal.
Footnotes
Authors’ Note
This review is part of a series of reviews initiated by AO spine knowledge forum. Systematic review registration number: Registered at PROSPERO (CRD42020209665).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.