
Abstract
Study Design
Retrospective Cohort Study.
Objective
This study aimed to explore the association between cervical disc degeneration and disease progression in patients with Hirayama disease, with a particular focus on changes in the cervical intervertebral disc space height and potential compensatory mechanisms.
Methods
This retrospective study included 35 patients diagnosed with Hirayama disease (HD), who were compared with 35 healthy control subjects matched for age and sex. This study focused on collecting and analyzing cervical disc grades and intervertebral space heights from C2 to C7, aiming to assess the extent of cervical disc degeneration between HD patients and the control group. The analysis used independent sample t tests and Mann‒Whitney U tests for demographic data and Spearman’s correlation coefficient to explore the relationship between disc degeneration and age.
Results
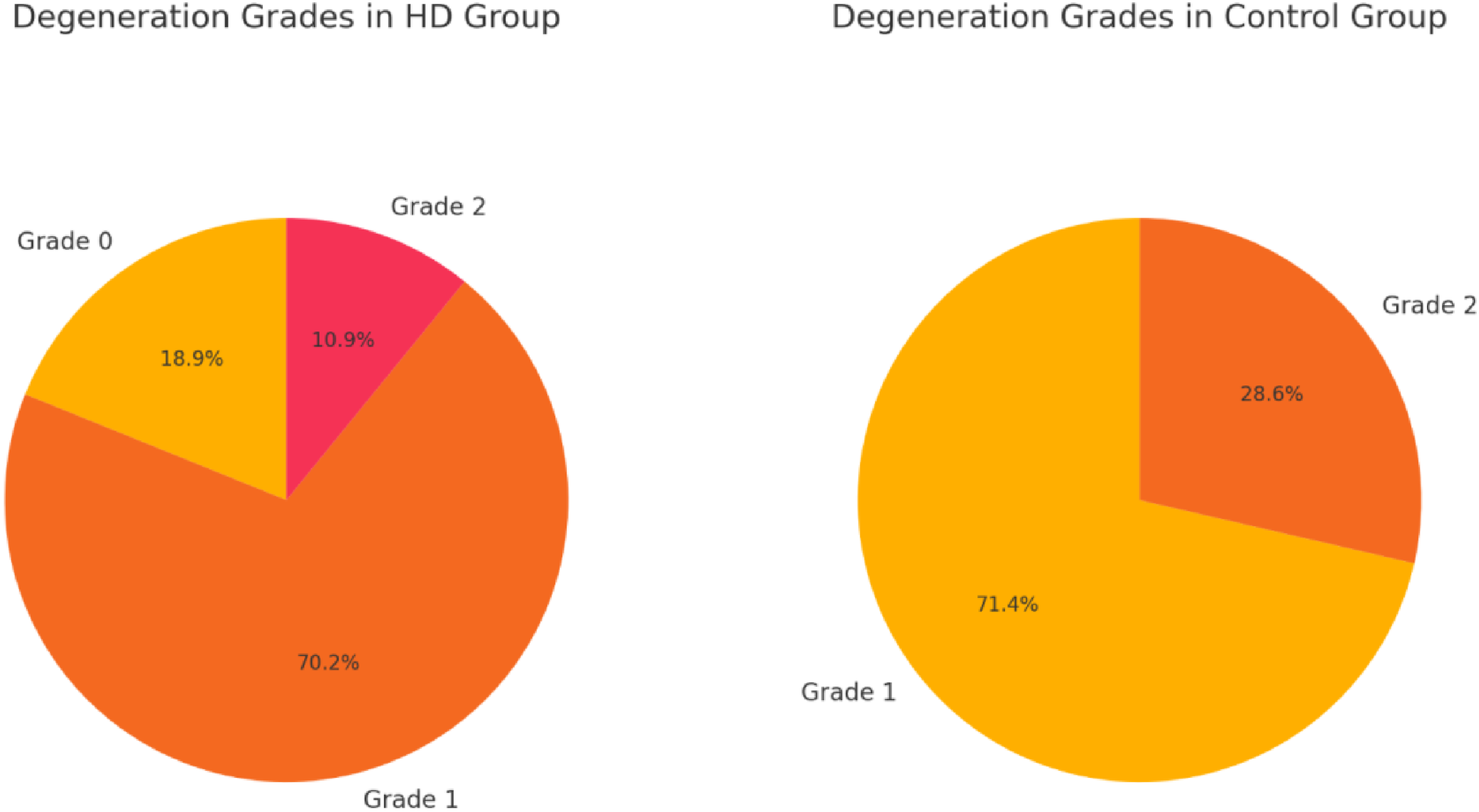
Compared with the control group, patients with Hirayama disease presented significant reductions in intervertebral disc height (P < .01) and increased disc degeneration. Within the HD group, most patients displayed multisegment degeneration (30 out of 35), and more than half presented with full-segment disc degeneration (20 out of 35), which was significantly different from the normal population (P < .01).
Conclusion
Patients with Hirayama disease exhibit disc degeneration and reduced intervertebral space height, which may represent a compensatory response.
Keywords
Introduction
Hirayama disease is considered a rare, benign, self-limiting disorder that often manifests as unilateral upper limb weakness and muscle atrophy and is predominantly observed in young Asian males. 1 The diagnosis of Hirayama disease relies primarily on imaging evidence. Characteristic manifestations of Hirayama disease on MRI include anterior displacement of the posterior dural sac at the lower cervical spine level when the neck is flexed.2,3 Considering the characteristic MRI findings in patients with Hirayama disease, ischemia of the anterior horn and/or nerve roots caused by excessive anterior displacement of the posterior dural sac during cervical flexion is currently considered the main hypothesis for the pathogenesis of HD. 4 During development, disproportionate growth between the dural sac and the spine causes the dural sac to be taut. When the cervical spine is flexed, the taut dural sac moves forward and compresses the posterior part of the spinal cord, leading to spinal cord compression ischemia. 5 Our study revealed that patients with Hirayama disease not only present with characteristic manifestations during neck flexion but also exhibit significant cervical disc degeneration. Why do these cervical disc changes occur?
The traditional view is that disc degeneration is closely related to genetics, degeneration, and aging. 6 In recent years, research has increasingly revealed a close interrelationship between the spinal cord and surrounding structures, including the vertebrae, intervertebral discs, and ligaments. Under pathological conditions of the spinal cord, the spine often undergoes compensatory changes,7-9 and disc degeneration may be an important compensatory mechanism.10,11 When Hirayama disease patients experience compression due to imbalanced growth between the dura mater and the spine, a compensatory mechanism may exist in the body. Through disc degeneration, this “compensatory regulation” reduces the compression caused by the relative shortening of the dural sac in relation to the cervical spine, improving spinal cord compression. This study aimed to explore the relationship between cervical disc degeneration and Hirayama disease through quantitative assessment of cervical disc degeneration and intervertebral disc space height. In the future, we will further explore how spinal structures, such as intervertebral discs, ligaments, and vertebral morphology, undergo compensatory changes in response to the condition of the spinal cord.
Materials and methods
Patient Population
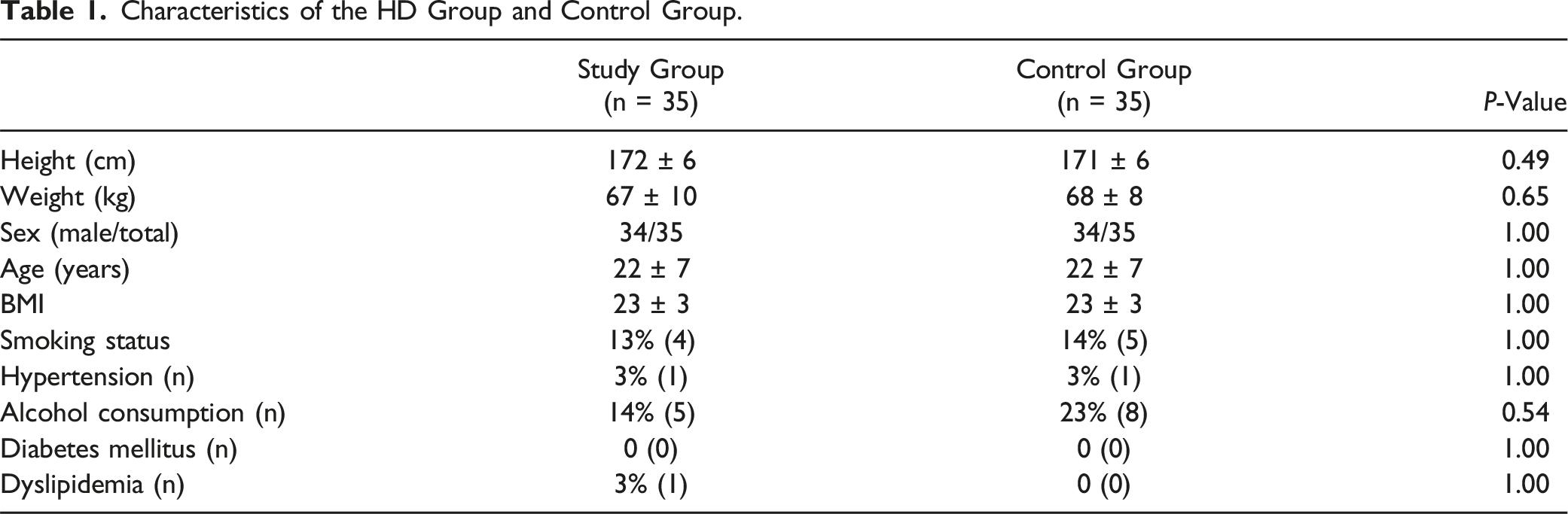
Ethical approval and consent to participate in this study were obtained from the ethics committee of the Third Hospital of Hebei Medical University (K2022-067-1). All patients were fully informed about the clinical trial and signed informed consent forms to participate. This study followed a retrospective case‒control design. The study population comprised patients diagnosed with Hirayama disease at our institution between June 2016 and April 2024. All patients met the definitive HD diagnosis criteria established by the international guidelines for the diagnosis and treatment of Hirayama disease formulated by clinical doctors in 2020. 12 The inclusion criteria for the study included the following: (A) unilateral intrinsic hand muscle atrophy, cold paresis, and extensor tremor symptoms; (B) spinal cord atrophy (SCA) and loss of attachment (LOA) observed on the sagittal plane of MR T2-weighted imaging (T2WI) when the neck was bent; and (C) electromyography (EMG) showing segmental localized nerve damage in the anterior horn or anterior roots of the spinal cord. Patients with traumatic brain injury, epilepsy, Parkinson's disease, or other neurological disorders were excluded, as were those with claustrophobia, metallic implants in the body, or other conditions making MRI examination intolerable. Ultimately, 35 patients met the inclusion criteria and participated in this study. The control group consisted of healthy individuals enrolled over the same study period from the medical examination center where the researchers were based. To minimize the influence of key confounding factors, the control group was rigorously matched with the experimental group in terms of age, sex, and height. Participants without symptoms in the neck or arms and who exhibited normal sensation, muscle tone, and deep tendon reflexes were considered eligible for inclusion. Individuals with any prior diagnoses or treatments affecting the entire spine were excluded from the control group. This included those with a history of spinal trauma, spinal deformity, spinal tumors, systemic arthritis, central nervous system disorders, peripheral neuropathies, or malnutrition impacting muscle function. Additionally, individuals who engaged in moderate to heavy physical labor were excluded. Other confounding factors included smoking, alcohol consumption, dyslipidemia, hyperglycemia and hypertension. Hypertension was defined as a systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg. Body mass index (BMI) was calculated by dividing the participant's weight by the square of their height (kg/m2).
Imaging Technique
All MRI data for the subjects in this study were acquired using the same MRI equipment (1.5T, Magnetom Verio, Siemens Medical Solutions, Germany). All images needed for measurement in this study were obtained from the electronic imaging system workstation at our institution. Axial T2-weighted MR images of all subjects were collected and analyzed using Radiant Viewer.
Radiographic Evaluation
This paper describes cervical disc degeneration via the grading system proposed by Lloydine J. Jacobs in 2016 for cervical disc degeneration 13 : Grade 0: normal, light gray center, and mid cleft still visible; Grade 1: Dark disc, not collapsed; Grade 2: Dark disc, collapsed with minimal osteophytes; Grade 3: Dark disc, collapsed with many osteophytes. Because there were no statistically significant differences in age, height, weight, or BMI between the experimental and control groups and endplate collapse generally occurs in the later stages of disc degeneration, this study used direct measurements of the anterior and posterior disc space heights and their averages to describe the height of the disc space. All MRI analysis measurements for the study participants were conducted based on supine-position MRI. Two physicians independently measured all the parameters, and the final result was an average of the two measurements. Grading was performed by two spinal surgeons, and excellent interobserver reliability (kappa score = 0.85) was observed. Any variations in grading between the observers were reviewed by the senior author and graded appropriately.
Statistical Analysis
All the statistical analyses were performed via IBM SPSS 23.0 (IBM Corp, Armonk, NY, USA), and the Kolmogorov–Smirnov test was used to confirm a normal distribution. Independent sample t tests and Mann‒Whitney U tests were used to assess the demographic data, including age, height, weight, BMI, disc space height, and disc grade, of Hirayama disease patients and healthy controls. The chi-square test was used to evaluate general information about the subjects. The Spearman correlation coefficient was used to determine the correlation between disc grade and age. To better understand the manifestation of disc degeneration in patients with Hirayama disease, a disc grade higher than 2 was defined as severe cervical disc degeneration (SCDD), and degeneration segments extending beyond three segments were defined as multisegment cervical degeneration (MCDD). In all instances, a P value of <0.05 was considered to indicate statistical significance.
Results
Characteristics of the HD Group and Control Group.
Intervertebral Space Height of the HD Group and Control Group.
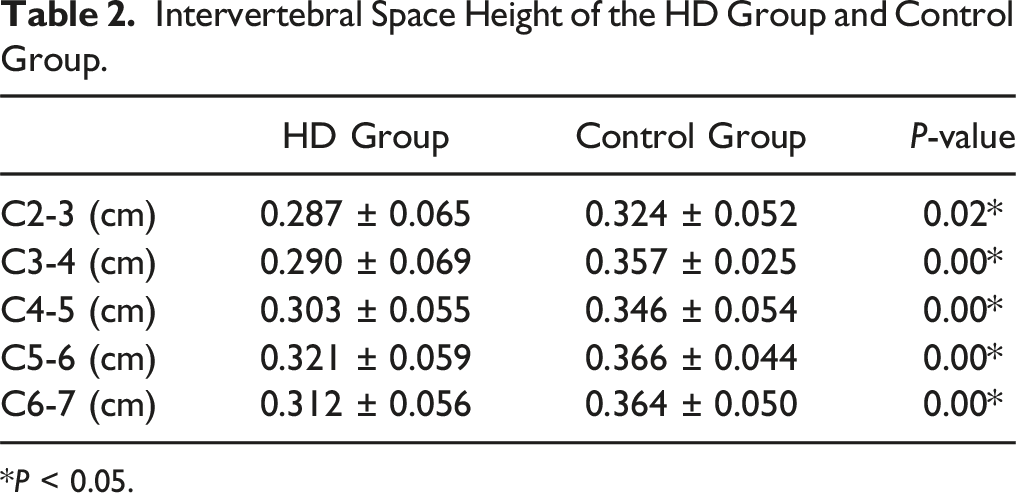
*P < 0.05.
The Segmental Distribution of disc Degeneration in the study Population.
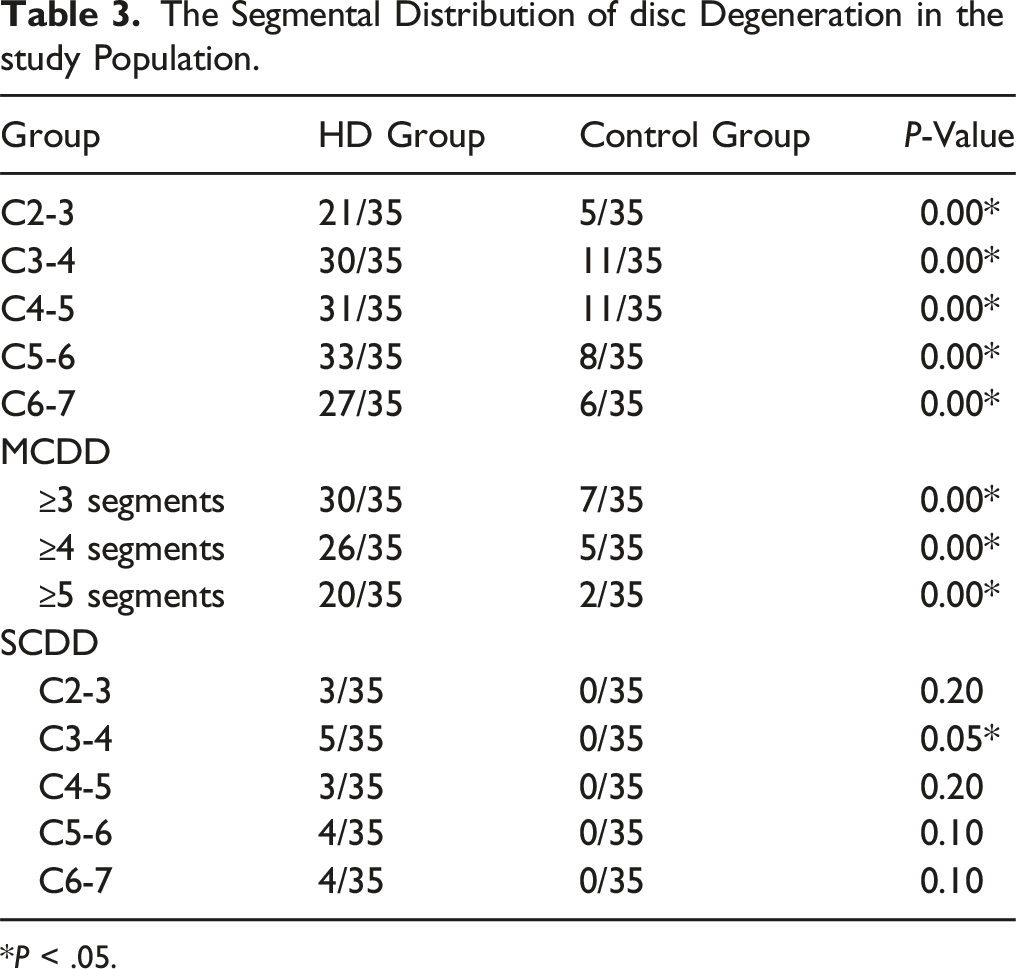
*P < .05.
Relationship Between Intervertebral disc Grade and Age.
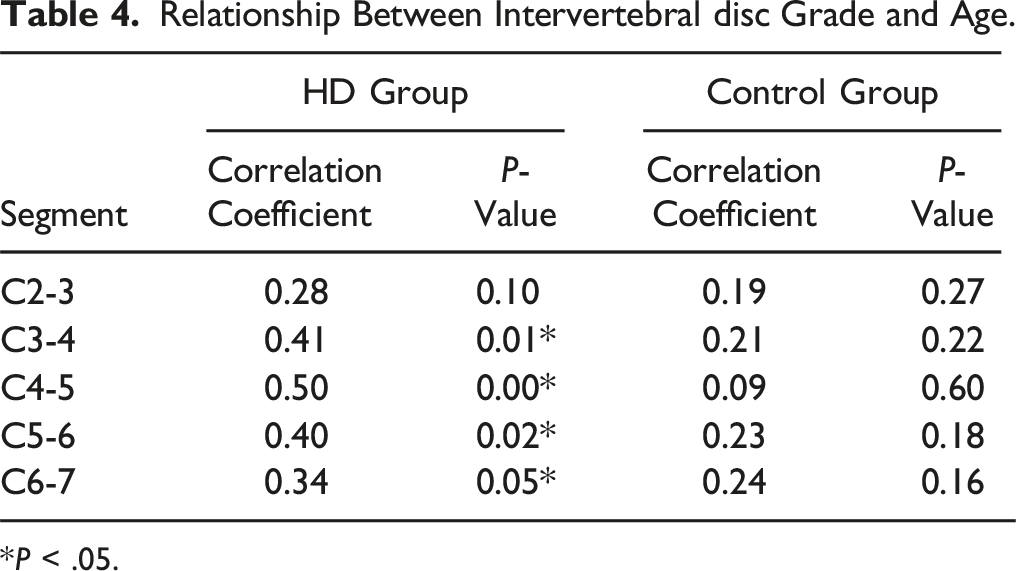
*P < .05.
Discussion
Hirayama disease (HD) is considered a rare, benign, self-limiting disease that commonly manifests as unilateral upper limb weakness and muscle atrophy and is predominantly observed in young Asian males. 1 Current research posits that excessive anterior displacement of the posterior dura mater during cervical flexion causing ischemia of the anterior horn and/or nerve roots is a principal hypothesis for the pathogenesis of HD.5,14 Studies by Chen 15 revealed that many patients also experience loss of attachment (LOA) in a neutral position, suggesting that the dural sac in HD patients is abnormally taut even without neck flexion. It is generally believed that the posterior wall length increases significantly compared with the anterior wall during spinal flexion, and Chen 16 suggested that the loss of cervical curvature could increase the cervical height, exacerbating the symptoms of HD. Xu's research indicated that HD patients, compared with healthy individuals, have greater cervical mobility, which produces more tension on the dura during repetitive flexion and extension of the neck, further exacerbating spinal cord compression. 17 Tian suggested that a lack of posterior neck muscles causing cervical instability could also be a causative factor for HD. 18 Although there is no consensus on the etiology of HD, current research supports the dynamic neck flexion hypothesis, which suggests that various factors lead to a disproportionate relationship between cervical height and dural length. For patients in relatively stable condition, wearing a cervical brace to restrict neck flexion is a common approach. 19 However, some patients exhibit poor compliance with long-term brace use. In cases where the disease progresses rapidly, surgical interventions may be applied. Anterior cervical discectomy and fusion surgery are mainstream surgical methods for HD patients; these methods effectively restore the cervical curvature, stabilize compressive segments, and reduce the cervical height to achieve favorable outcomes. 20 Previous studies have demonstrated that correcting disproportionate cervical height to the dura and reducing excessive cervical activity are key principles in the treatment of HD.19-21
Our findings revealed significant differences in cervical disc degeneration and cervical intervertebral disc height between HD patients and healthy individuals (Tables 3 and 4). Compared with normal patients, HD patients exhibit multisegment cervical disc degeneration and even full-segment degeneration, with reduced intervertebral disc heights. Lu’s research indicated that abnormal increases in the range of motion (ROM) in HD patients could increase the cervical load, 22 potentially increasing susceptibility to cervical disc degeneration in these patients. However, this increased ROM and load are primarily noted in the lower cervical spine, and our findings indicate that degeneration in patients with Hirayama disease is observed in the C2-3 segment, and this degeneration does not correlate with age (Tables 2 and 3). Hirayama disease typically manifests in younger patients, who are rarely afflicted by chronic metabolic conditions such as hypertension, hyperlipidemia, or diabetes. Therefore, the cervical degeneration observed in patients with Hirayama disease is challenging to attribute to metabolic abnormalities or excessive activity levels.
Thus, the pathomechanics of disc degeneration in HD require further exploration. A key question remains: is cervical disc degeneration and a reduction in intervertebral space height a cause or a consequence of HD? Our group considers disc degeneration as a possible compensatory response to some spinal cord disorders. Jian-gang introduced the concept of “bowstring disease”, suggesting that when nerves are under tension, the body may employ various strategies, such as nerve growth, postural adjustments, autogenous degeneration of intervertebral discs, idiopathic scoliosis, and degenerative scoliosis, to reduce nerve tension. 7 We believe that the spine, intervertebral discs, and spinal cord should be viewed as a functional whole; abnormalities in one part can induce changes in the entire system. Just as facet joint hypertrophy in spondylolysis patients might serve to counteract unstable lumbar vertebrae, 23 disc degeneration could be a “compromised regulation” by the body to protect the more vital spinal cord. Research has shown that disc degeneration leads to a reduction in intervertebral space height and may be associated with spinal stiffness. 22 Although the specific etiology of Hirayama disease (HD) remains unclear, its radiographic hallmark is a mismatch between the cervical height and dural length. The posterior dural sac, which is too short, is pulled forward when the cervical spine is flexed, causing persistent compression of the spinal cord. Current research suggests that HD often ceases to progress within a few years, which might indicate that the reduction in intervertebral space height is a compensatory response to the shortening of the posterior dural sac. The findings of this study suggest that the cervical disc degeneration observed in HD patients could be a compensatory change whereby the body reduces the height of the spine through shortening of the intervertebral space to match the shortened dural sac and stabilizing a highly ROM cervical spine. These findings suggest a complex interrelationship between the spinal cord and the cervical spine, likely involving compensatory mechanisms.
Conversely, an abnormal state of the spine can also impact spinal cord function. Previous studies have demonstrated that osteotomy can be used to treat tethered spinal cord syndrome 24 and that releasing the tethered cord can also slow the progression of scoliosis. 25 When symptoms arise from a mismatch between the spine and the spinal cord, correcting one anomaly can alleviate the progression of another pathological change. Spine surgeons should be aware of this association, as in most cases, during surgery, spine surgeons often focus on avoiding direct damage to the spinal canal and nerve roots. When expanding or correcting the spine, it is important to consider whether the procedure may cause excessive axial traction on the spinal cord to avoid inducing iatrogenic spinal cord symptoms. This awareness is vital to prevent complications and optimize surgical outcomes by respecting the intricate balance between spinal structure and neurological function. The results of this study should be interpreted with caution. This study focused solely on the correlation between Hirayama disease (HD) patients and cervical disc degeneration and demonstrated that HD patients exhibit widespread cervical disc degeneration. However, owing to the lack of long-term follow-up of HD patients who undergo conservative treatment and the absence of monitoring electrophysiological changes before and after treatment, the discussion on disc degeneration in this article is based solely on inferences made from disease progression in HD patients. Future studies could yield more significant results by longitudinally monitoring patients undergoing conservative treatment, observing changes in intervertebral space height, and regularly monitoring neurophysiology.
Conclusion
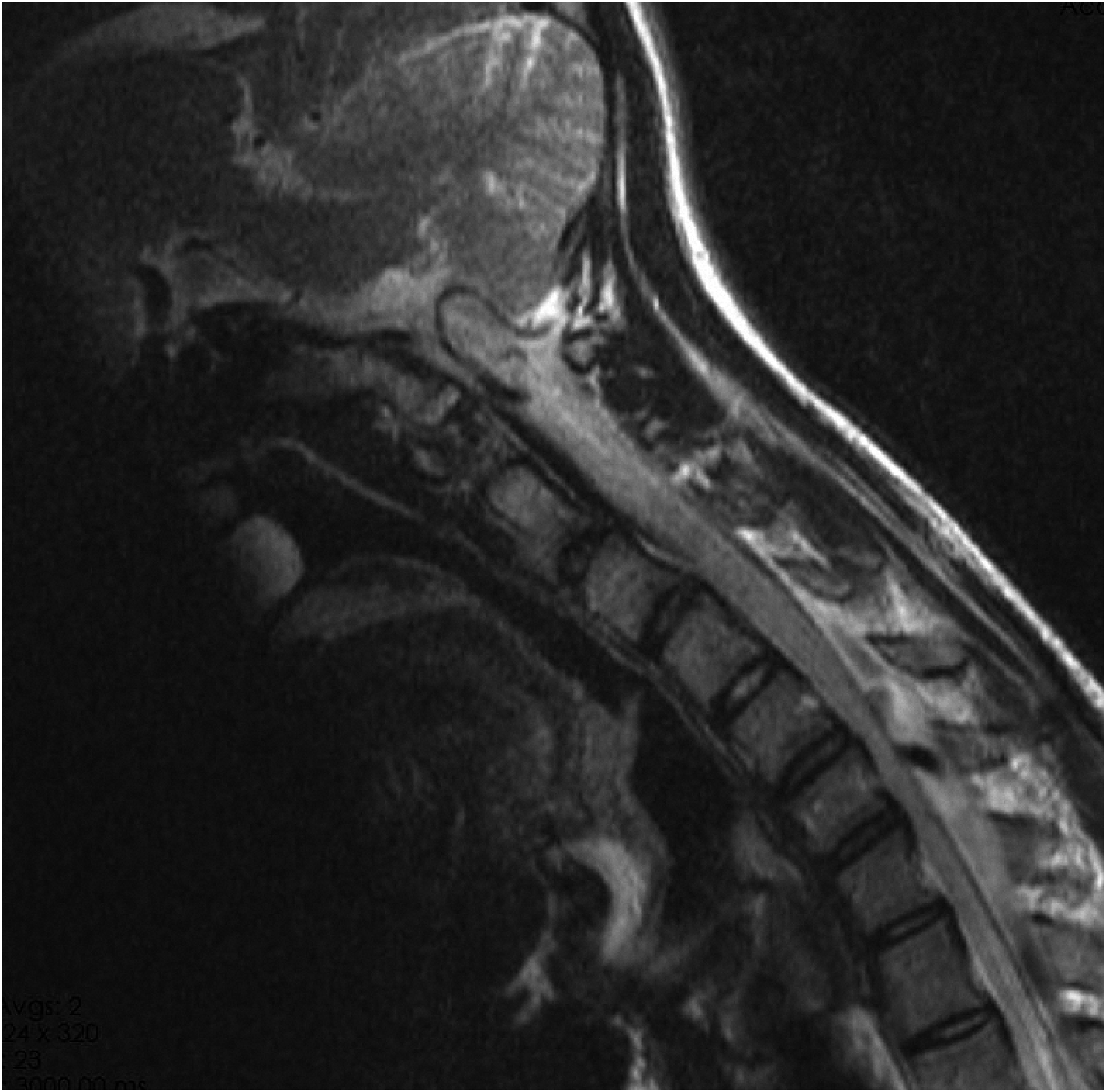
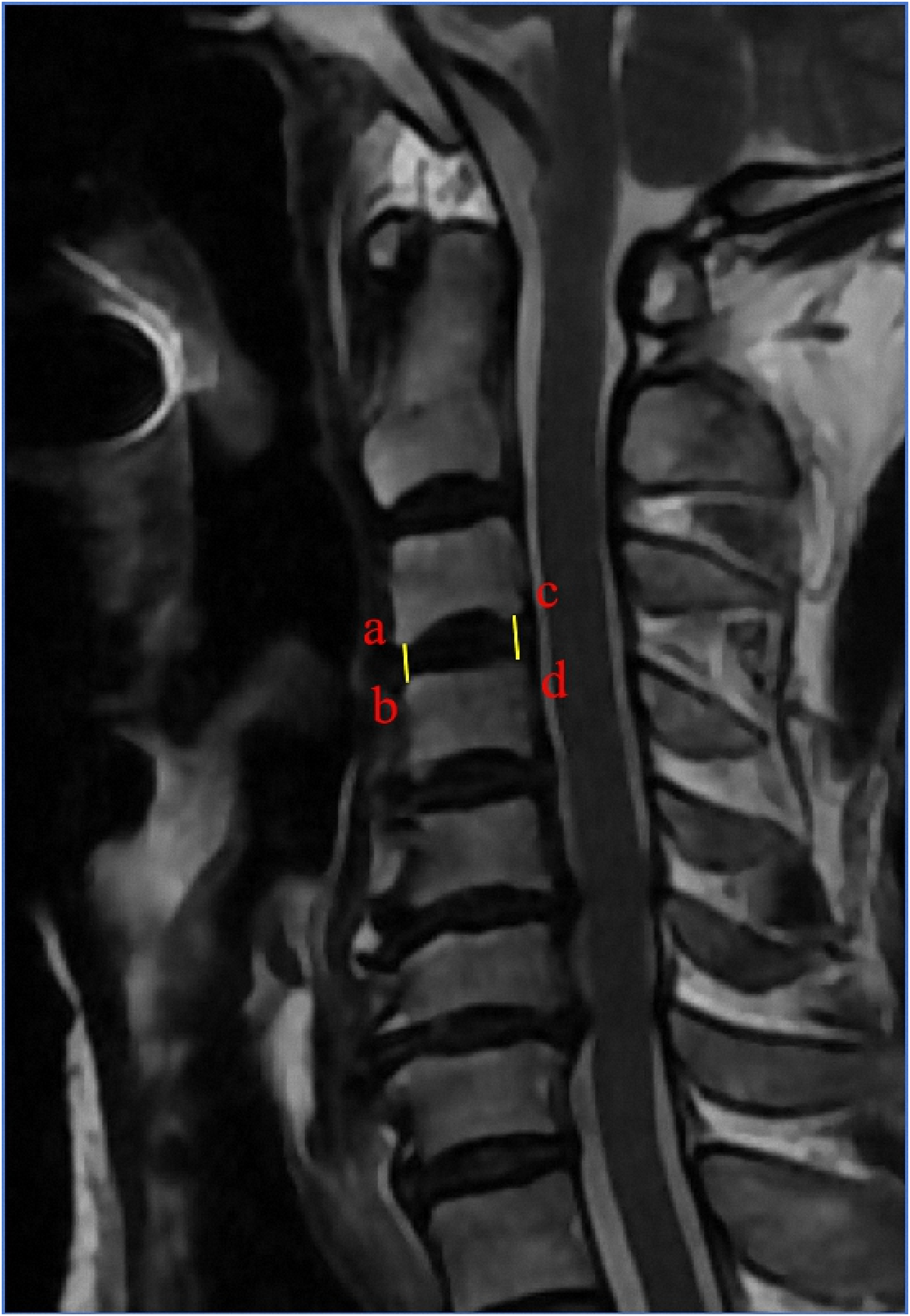
This retrospective study revealed that most patients with Hirayama disease exhibit multisegment disc degeneration, which reduces the cervical intervertebral space height. This degeneration may represent a compensatory change associated with the development of Hirayama disease. Future investigations should aim to deepen the understanding of the underlying mechanisms and potential therapeutic interventions for managing and possibly reversing the complications associated with this condition (Figures 1–4). Cervical disc degeneration graded according to Jacob’s classification (Jacob et al., 2016). Grade 0: Normal, light grey center, mid cleft still visible. Grade 1: Dark disc, not collapsed. Grade 2: Dark disc, collapsed with minimal osteophytes. Grade 3: Dark disc, collapsed with many osteophytes. Depicts a typical cervical spine MRI image of a patient with Hirayama disease. Describes the method for measuring the height of the cervical intervertebral space. Given that there was no statistically significant difference in height between the control group and the experimental group, the researchers chose to use the average value of the anterior and posterior edges of the intervertebral space to describe the intervertebral space height. The a-b line represents the anterior disc height, measured as the vertical distance between the anterior endplates of adjacent vertebrae, while the c-d line represents the posterior disc height, measured in the same manner at the posterior endplates. Describes the comparison of the grades of intervertebral disc degeneration between the experimental group and the control group.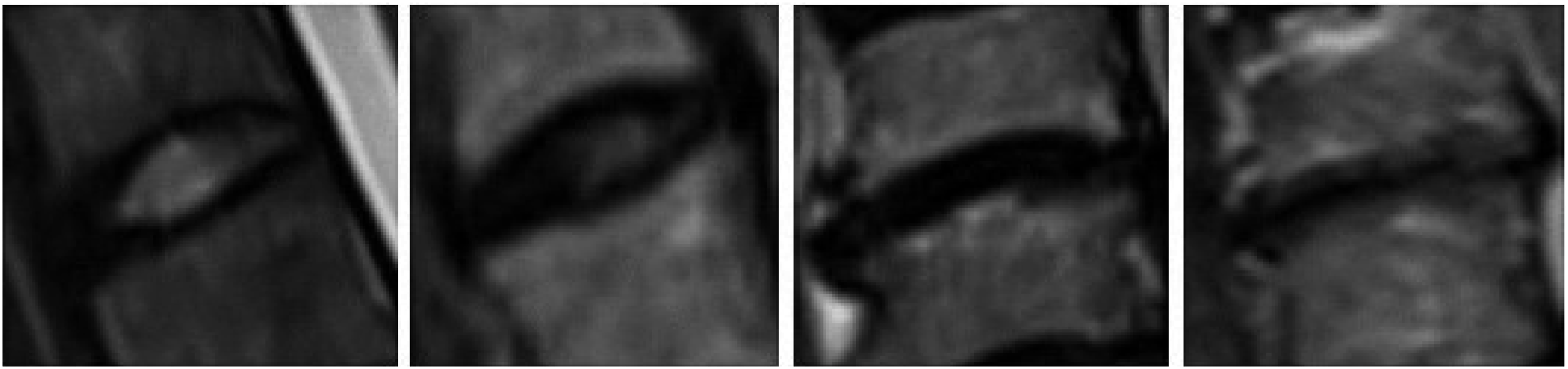
Footnotes
Author Contributions
Xianzhong Meng: Conceptualization, Supervision. Zhaoxuan Wang: Data curation, Writing-Original draft preparation. Hengrui Chang: Writing–review & editing. Jianhua Ren: Methodology, Software. Guzhen Liang: Software. Junkai Kou: Investigation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Government-Funded Clinical Medicine Outstanding Talent Training Program (ZF2024088).