
Abstract
Purpose:
Cervical sagittal balance plays important roles in transmitting the load of the head and maintaining global spinal balance. This study aimed to identify the association of cervical sagittal alignment with adjacent segment degeneration (ASD) and heterotopic ossification (HO) after Prestige-LP cervical disc replacement (CDR).
Methods:
We enrolled 132 patients who underwent one-level Prestige-LP CDR with 2–10 years of follow-up. Cervical sagittal alignment parameters, including the degree of C2–C7 lordosis (CL), functional spinal unit angle (FSUA), sagittal vertical axis (SVA),, and T1 slope (T1s), were measured. ASD and HO were evaluated at the last follow-up. Unpaired t tests and logistic regression analysis were used to identify the associations of cervical sagittal alignment with ASD and HO.
Results:
We found that patients who developed ASD showed significantly lower FSUA (2.1° vs. −1.4°, p < 0.001) and T1s values (28.4° vs. 25.5°, p = 0.029) after surgery. Similarly, the postoperative CL was significantly better in patients without ASD or HO (18.0° vs. 14.4°, p = 0.043). The decrease in the T1s at the last follow-up was significantly larger in the patients with ASD (−11.0° vs. −3.2°, p = 0.003), HO (−6.7° vs. −2.7°, p = 0.050), and ASD or HO (−7.0° vs. −0.8°, p < 0.001) than in those without ASD or HO. Multivariate logistic regression analysis showed that both the FSUA and T1s are associated with ASD and that the degree of CL is associated with postoperative complications.
Conclusion:
The results imply that maintaining cervical sagittal alignment after Prestige-LP CDR is important.
Keywords
Introduction
Cervical sagittal balance plays important roles in transmitting the load of the head and maintaining global spinal balance. 1 Cervical sagittal malalignment is associated with neck pain and low quality of life. 2 –4 In addition, cervical sagittal malalignment may cause the degeneration of cervical spine segments. 5 For the purpose of quantifying cervical sagittal alignment, several parameters have been proposed, such as C2–C7 lordosis (CL), segmental lordosis (measured as the functional spinal unit angle (FSUA)), sagittal cervical axis (SVA), and T1 slope (T1s). Several studies have shown that the above cervical sagittal alignment parameters are associated with patient outcomes after anterior cervical spine surgeries, such as anterior cervical discectomy and fusion (ACDF). 6 –10 For instance, poor CL and kyphotic FSUAs are risk factors for adjacent segment degeneration (ASD), 8,11,12 and a high T1s is associated with pseudarthrosis and implant subsidence following ACDF. 6,10 However, the relationship between cervical sagittal balance and other kinds of anterior cervical spine surgeries, such as cervical disc replacement (CDR), is poorly understood.
CDR has been considered an effective option for the treatment of cervical degenerative disc disease (CDDD). This nonfusion technique aims at preserving the range of motion (ROM) at the surgical level and delaying degeneration at adjacent levels. 13 –16 To restore the physiological condition of the cervical spine after CDR, it is hypothesized that the cervical sagittal alignment parameters should be corrected to the normal level. However, most previous studies have only focused on describing the CL and FSUA values after CDR, and the other cervical sagittal alignment parameters have been rarely studied. It is not clear whether the cervical sagittal balance is associated with postoperative complications after CDR, including ASD and heterotopic ossification (HO).
Prestige-LP is one of the most commonly used artificial discs currently. Gornet et al. 17,18 have demonstrated that Prestige-LP CDR can effectively relieve patients’ symptoms and preserve the ROM at 10-year follow-up. Compared with ACDF, Prestige-LP CDR showed lower prevalence of ASD and reoperation during long-term follow-up. 17 –20 However, the cervical sagittal alignment and its impacts on clinical outcomes after Prestige-LP CDR has been rarely studied.
We hypothesized that cervical sagittal alignment parameters can affect the outcomes of Prestige-LP CDR. In this study, we evaluated the cervical sagittal alignment parameters (CL, FSUA, SVA, and T1s) of patients who underwent one-level Prestige-LP CDR with a minimum follow-up period of 24 months. We analyzed the association of those parameters with ASD and HO after CDR. We hope our results will guide the prescription of rehabilitation exercises for Prestige-LP CDR patients and reduce postoperative complications.
Materials and methods
Study design and patient selection
This study was a retrospective study and was approved by the Institutional Review Board of West China Hospital. We enrolled patients who underwent one-level CDR using the Prestige-LP cervical disc system and had a minimum follow-up of 24 months. All patients received surgical treatment at our center between January 2008 and December 2017. The surgical indications were as follows: (1) age between 18 years and 65 years, (2) one-level CDDD between C3 and C7 that has led to symptomatic cervical myelopathy or radiculopathy, and (3) a history of conservative treatment for at least 3 months without improvement. The surgical contraindications were as follows: (1) cervical instability at the surgical level, (2) irreducible kyphosis during flexion–extension, (3) severe facet joint degeneration or spondylosis at the surgical level, (4) cervical spine fracture, tumor, or infection, (5) ossification of the posterior longitudinal ligament, (6) ankylosing spondylitis, rheumatoid arthritis, or other metabolic bone disease, and (7) osteoporosis with a T-score of ≤−2.5. Clinical outcomes, such as the Japanese Orthopaedic Association (JOA) score, neck disability index (NDI) score, and visual analog scale (VAS) score, were evaluated before surgery and 1 week after surgery.
Assessment of cervical sagittal alignment parameters
We measured cervical sagittal alignment parameters on the lateral radiographs according to the methods presented in previous studies (Figure 1). 21,22 The following parameters were evaluated: (1) CL, measured as the angle between the inferior end plate of C2 and the inferior end plate of C7; (2) FSUA, measured as the angle between the superior end plate of the superior vertebra and the inferior end plate of the inferior vertebra at the surgical segment; (3) sagittal cervical axis (SVA), measured as the distance between the plumb line from the center of C2 and the superior posterior corner of C7; and (4) T1s, measured as the angle between the superior end plate of T1 and a horizontal line. When obtaining radiographs, the anterior–posterior view of the cervical spine was taken at first, and patients were required to (1) stand and look straight ahead, with their hips and knees extended; (2) lean their back against the fluorescent screen. After taking the anterior–posterior radiograph, patients were required to turn right 90° and lateral radiographs were taken. These procedures could reduce bias when taking radiographs. If T1s cannot be obtained from lateral radiographs, then C7 slope would be measured, and T1s would be calculated using the following formula: T1s = (C7 slope + 0.54)/0.88. 21

Radiological evaluation of the cervical sagittal alignment after cervical disc replacement.
The postoperative values (values at 1 week after surgery) of the cervical sagittal alignment parameters were measured. Because cervical sagittal alignment may change over time, the differences between the values at the last follow-up and postoperative values (last minus postoperative, Δ) were calculated. However, the values at the last follow-up may be a result of the compensatory response of ASD or HO and may not reflect the impact of cervical sagittal alignment; therefore, they were not included in the analysis of this study. All measurements were performed by two surgeons independently, and the mean values were calculated and recorded.
Assessment of ASD and HO
ASD was evaluated on the lateral radiographs at the last follow-up, as they were in previous studies, and ASD was defined by the presence of at least one of the following conditions 23,24 : (1) ossification of the anterior longitudinal ligament, (2) narrowing of intervertebral disc space at the superior or inferior adjacent level, with or without osteophytes, and (3) new or enlarged anterior osteophytes at adjacent levels. HO was evaluated on the lateral radiographs and sagittal plane reconstruction CT scans taken at the last follow-up. According to the McAfee classification criteria, HO was defined as the exposed bony end plates of the vertebral bodies at the surgical-level growth toward the artificial disc. HO was classified into low-grade HO (grade 1–2) and high-grade HO (grade 3–4, ROM-limiting HO). 24,25 The assessments of ASD and HO were performed by two surgeons independently, and the discrepancies were settled by consulting another senior surgeon to reach a consensus.
Statistical analysis
Patients with missing data were excluded from this study. Continuous variables are presented as the mean ± standard deviation (SD). Categorial variables are presented as the number of cases. The paired t test was used to compare the clinical outcomes before and after the surgery. Student’s t test (for normally distributed data) or the Mann–Whitney U test (for nonnormally distributed data) was used to compare the data between two groups. Logistic regression analysis was used to identify the association of postoperative and Δ cervical sagittal alignment with ASD and HO. Variables with p ≤ 0.20 in the univariate analysis were included in the multivariate logistic regression analysis. All statistical analyses were performed using SPSS 22.0 software (IBM Corp., Armonk, New York, USA). A two-tailed p-value of <0.05 was defined as statistically significant.
Results
General information on the patients
In the current retrospective study, 132 patients were included. All patients underwent one-level CDR using the Prestige-LP cervical disc system. All surgeries were performed by the same senior surgeon. The baseline characteristics of the patients are presented in Table 1. The average age of the patients in this study was 43.6 ± 7.6 years, with a range from 28 years to 63 years. The mean follow-up time was 43.2 ± 22.6 months, with a range from 24 months to 120 months. The most frequent surgical level was C5/6. The clinical outcome scores including the JOA, NDI, and VAS all improved significantly after surgery compared with before surgery (p < 0.05 for each score). We did not find significant correlations between cervical sagittal alignment parameters and clinical outcome scores at the last follow-up time (JOA, NDI, and VAS). Twenty-four patients (constituent ratio: 18.18%) with high-grade HO and 62 patients (constituent ratio: 46.97%) with low-grade HO were identified. The presence of HO significantly decreased the segmental ROM at the last follow-up (8.7 ± 4.9° vs. 11.0 ± 6.0°, p = 0.017). However, the presence of ASD did not affect the segmental ROM (Supplementary Table 1).
General information on the patients.a
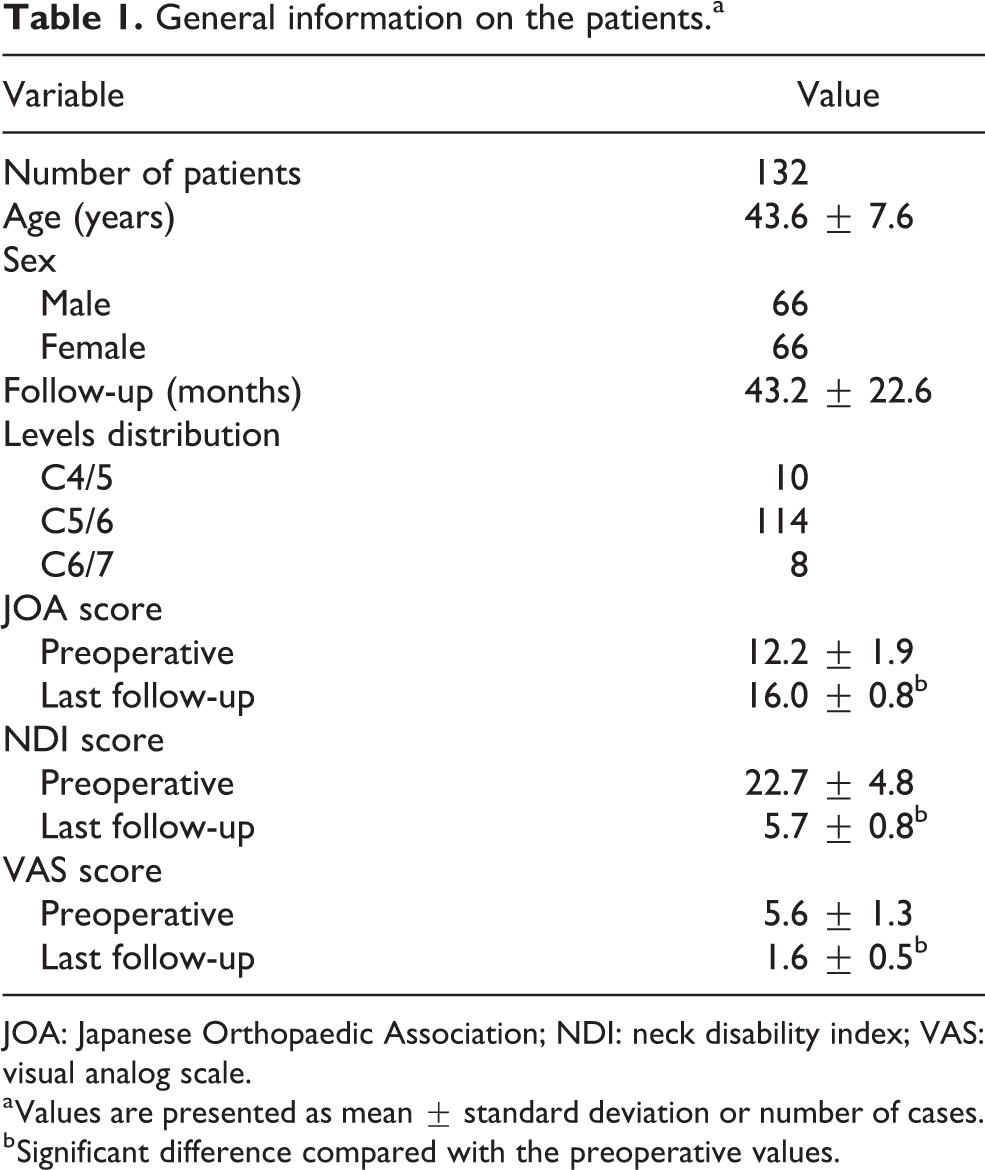
JOA: Japanese Orthopaedic Association; NDI: neck disability index; VAS: visual analog scale.
a Values are presented as mean ± standard deviation or number of cases.
b Significant difference compared with the preoperative values.
Relationship between the cervical sagittal alignment parameters and ASD
Table 2 shows the characteristics of the cervical sagittal alignment parameters in the presence of ASD. The patients were divided into the ASD group or non-ASD group according to the features found on their radiographs at the last follow-up. The degree of CL in the ASD group was smaller than that in the non-ASD group, but the difference did not reach statistical significance (13.6° vs. 16.1°, p = 0.239). The SVA was comparable between the two groups (p = 0.909). Significant kyphotic FSUAs were noticed in the ASD group, while the mean FSUA in the non-ASD group was lordotic (−1.4° vs. 2.1°, p < 0.001). In addition, the T1s was significantly smaller in the ASD group than in the non-ASD group (25.5° vs. 28.4°, p = 0.029).
Cervical sagittal alignment parameters with the presence of adjacent segment degeneration.a
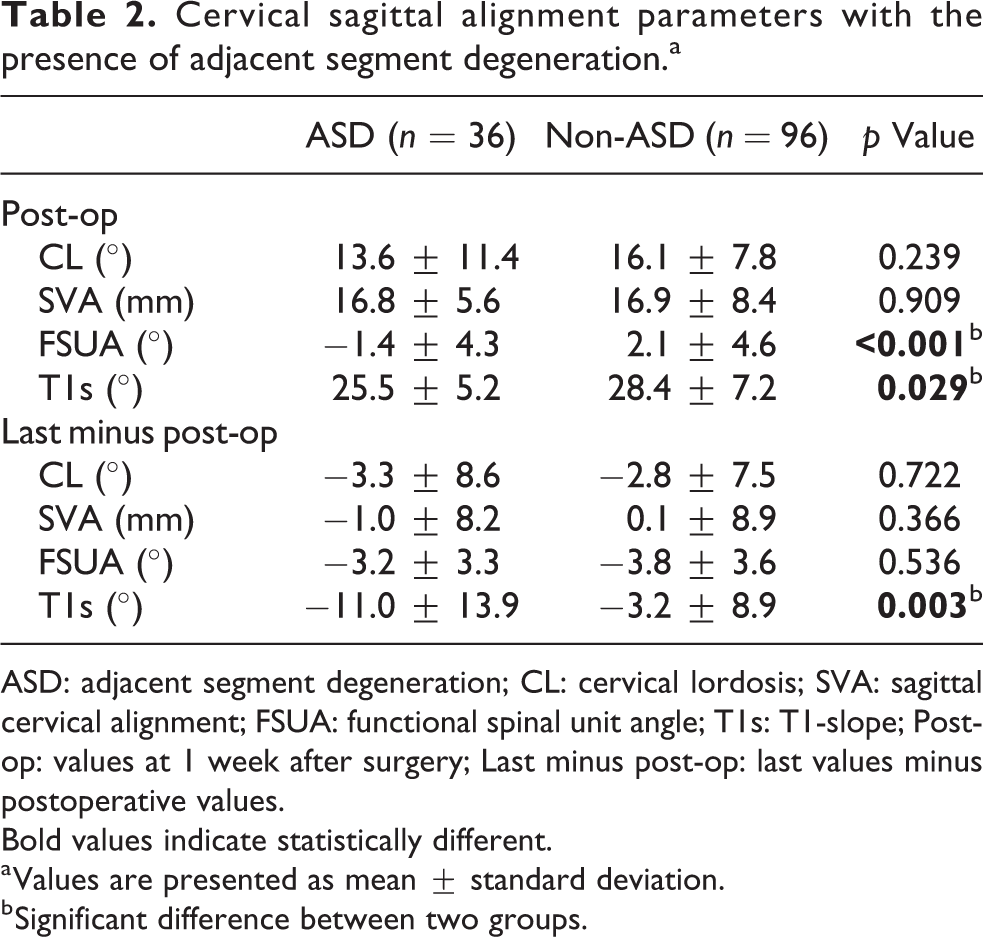
ASD: adjacent segment degeneration; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Values are presented as mean ± standard deviation.
b Significant difference between two groups.
The difference between the cervical sagittal alignment values at the last follow-up and postoperative values was calculated (represented symbolically by Δ, and a Δ value closes to zero means the sagittal alignment was maintained well at the last follow-up). This difference can help clarify the importance of maintaining cervical sagittal alignment to reduce the risk of complications. In the current study, ΔT1s was the only variable that was found to be significantly different between the two groups (−11.0° in the ASD group vs. −3.2° in the non-ASD group, p = 0.003).
Relationship between the cervical sagittal alignment parameters and HO
Table 3 shows the characteristics of the cervical sagittal alignment parameters in the presence of HO. The patients were divided into the HO group or non-HO group according to the McAfee criteria at the last follow-up. The degree of CL in the HO group was slightly smaller than that in the non-HO group (14.7° vs. 16.8°, p = 0.201), but the difference did not reach statistical significance. There was no significant difference in the FSUA or T1s between the two groups (p > 0.05 for each variable). However, the ΔT1s was significantly smaller in the HO group than in the non-HO group (−6.7° vs. −2.7°, p = 0.050).
Cervical sagittal alignment parameters with the presence of heterotopic ossification.a

HO: heterotopic ossification; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Values are presented as mean ± standard deviation.
b Significant difference between two groups.
Relationship between the cervical sagittal alignment parameters and ASD or HO
Table 4 shows the characteristics of the cervical sagittal alignment parameters in the presence of ASD or HO (collectively called AOH). Patients were included in the AOH group if they had ASD or HO at the last follow-up. Conversely, patients were included in the non-AOH group if they had neither ASD nor HO. Patients with AOH showed significantly smaller degrees of CL than those without AOH (14.4° vs. 18.0°, p = 0.043) after surgery. In addition, patients with AOH showed a larger SVA than those without AOH, although this difference did not reach statistical significance (17.6 mm vs. 15.0 mm, p = 0.081). There was no significant difference between the two groups in the ΔCL or ΔSVA.
Cervical sagittal alignment parameters with the presence of either adjacent segment degeneration or heterotopic ossification.a

AOH: the presence of either ASD or HO; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Values are presented as mean ± standard deviation.
b Significant difference between two groups.
Both the FSUA and T1s were comparable between the two groups at 1 week after surgery (p > 0.05 for each variable). However, the ΔT1s was significantly larger in the AOH group than in the non-AOH group (−7.0° vs. −0.8°, p < 0.001). Unexpectedly, the decrease in the FSUA in the AOH group was smaller than that in the non-AOH group (−3.1° vs. −4.9°, p = 0.021). Although the difference between the two groups was small, it was statistically different.
Relationship between the cervical sagittal alignment and postoperative complications
Table 5 shows the result of univariate logistic regression analysis between cervical sagittal alignment and postoperative complications. At 1 week after surgery, a lower FSUA was significantly related to the presence of ASD (odds ratio (OR) 0.84, 95% confidence interval (CI) 0.77–0.93, p < 0.001). The results were similar for the T1s (OR 0.94, 95% CI 0.88–0.99, p = 0.032) and ΔT1s (OR 0.94, 95% CI 0.90–0.97, p = 0.001). In addition, the degree of CL was considered to be a potential protective factor for ASD (OR 0.97, 95% CI 0.93–1.01, p = 0.162).
Factors associated with the presence of ASD or HO according to the univariate logistic regression analysis.

ASD: adjacent segment degeneration; HO: heterotopic ossification; AOH: the presence of either ASD or HO; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate these values would be included in multivariable logistic regression analysis.
a Factors involved in multivariate logistic regression analysis.
b Statistical difference.
Cervical sagittal alignment failed to correlate with HO in univariate logistic regression analysis. Both the degree of CL (OR 0.97, 95% CI 0.93–1.01, p = 0.200) and ΔT1s (OR 0.96, 95% CI 0.93–1.01, p = 0.055) were considered to be potential protective factors, while the SVA (OR 1.04, 95% CI 0.99–1.09, p = 0.125) was considered to be a potential risk factor for HO.
When considering ASD and HO as a whole, both the degree of CL (OR 0.95, 95% CI 0.91–0.99, p = 0.046) and ΔT1s (OR 0.93, 95% CI 0.89–0.98, p = 0.006) were protective factors for the presence of AOH. In contrast, larger SVAs (OR 1.05, 95% CI 0.99–1.10, p = 0.083) and smaller ΔSVAs (OR 0.97, 95% CI 0.93–1.01, p = 0.177) were considered to be associated with AOH.
Theoretically, segmental misalignment negatively impacts patient outcomes after cervical spine surgery. This concept has been proved to be true by previous studies in terms of ACDF. However, in the current study, segmental misalignment was found to be a potential protective factor of HO and AOH, and these results are not consistent with this theory or those observed in clinical practice. Therefore, ΔFSUA was not included in the multivariate logistic regression analysis, although it was found to be correlated with the presence of HO and AOH.
Risk factors for postoperative complications
Tables 6 to 8 show the results of multivariate logistic regression analysis between cervical sagittal alignment and postoperative complications. Each 1° increase in the FSUA after surgery corresponded to a lower risk of ASD by 16% (OR 0.84, 95% CI 0.75–0.95, p = 0.005). Similarly, each 1° increase in the T1s after surgery corresponded to a decrease in the risk of ASD by 10% (OR 0.90, 95% CI 0.82–0.99, p = 0.032). When ASD and HO were considered together, a 1° increase in the degree of CL corresponded to a decrease in the risk of AOH by 8% (OR 0.92, 95% CI 0.86–0.98, p = 0.007). In addition, a higher value of ΔT1s, which indicated that the T1s was retained well at the last follow-up, was a protective factor for ASD (OR 0.90, 95% CI 0.85–0.94, p < 0.001), HO (OR 0.95, 95% CI 0.92–0.99, p = 0.021), and AOH (OR 0.90, 95% CI 0.85–0.96, p = 0.001).
Factors associated with the presence of ASD according to the multivariate logistic regression analysis.
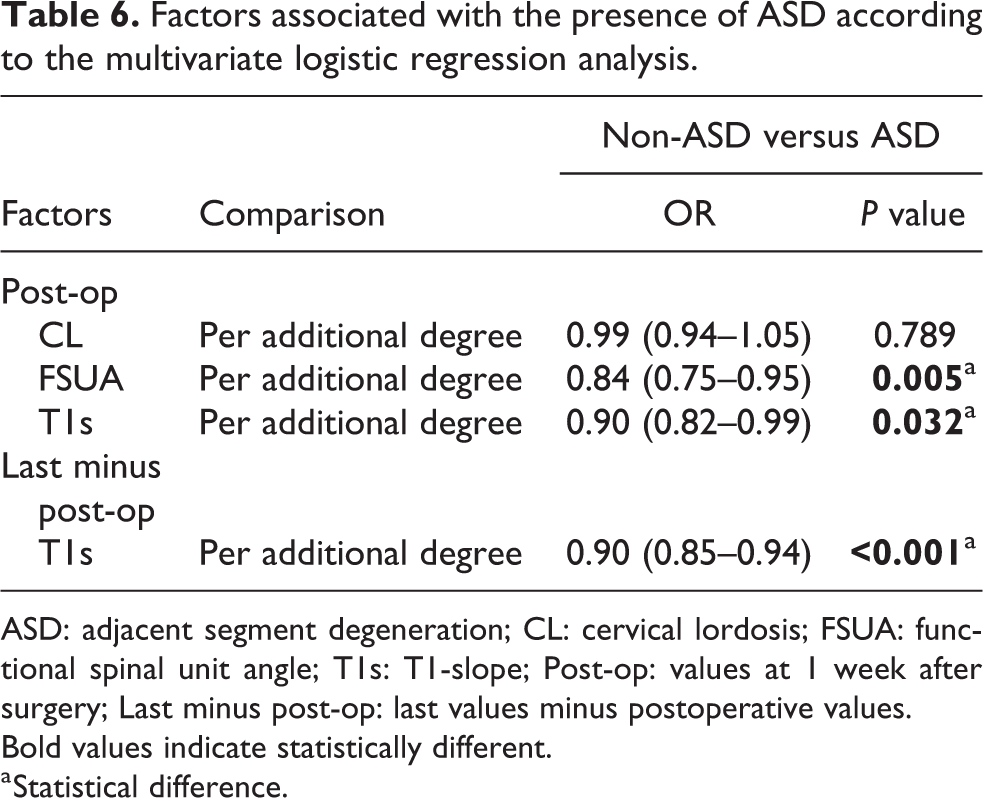
ASD: adjacent segment degeneration; CL: cervical lordosis; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Statistical difference.
Factors associated with the presence of HO according to the multivariate logistic regression analysis.
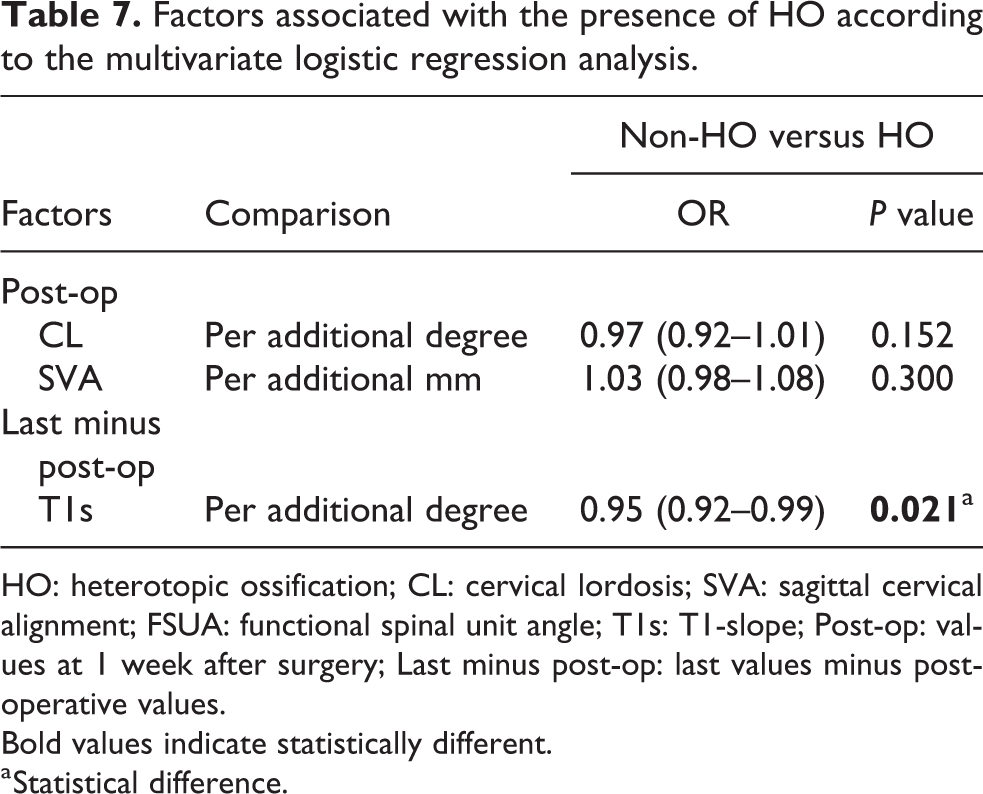
HO: heterotopic ossification; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Statistical difference.
Factors associated with the presence of ASD or HO according to the multivariate logistic regression analysis.

AOH: the presence of either ASD or HO; CL: cervical lordosis; SVA: sagittal cervical alignment; FSUA: functional spinal unit angle; T1s: T1-slope; Post-op: values at 1 week after surgery; Last minus post-op: last values minus postoperative values. Bold values indicate statistically different.
a Statistical difference.
Discussion
Multiple studies have shown that there is a relationship between cervical sagittal balance and neck pain, cervical disc degeneration, and the outcomes of ACDF. 3,4,7,9 –12,21,26 However, the importance of cervical sagittal parameters in CDR is rarely noted. In addition, the cervical sagittal alignment and its impacts on clinical outcomes after Prestige-LP CDR has been rarely studied. By performing a retrospective analysis with an average follow-up of 43 months, we found that cervical sagittal alignment parameters, including the degrees of cervical lordosis (CL), segmental lordosis, and T1s, were associated with ASD or HO after Prestige-LP CDR. The results of our study filled the gaps in previous studies.
In the current study, preoperative values of the cervical sagittal alignment were not included in the analysis. This is because in patients who underwent one-level Prestige-LP CDR, the presence of neck pain or neurological deficit resulted in significantly worse cervical sagittal alignments before surgery. 27 Therefore, it is not necessary to include preoperative values to access their associations with postoperative complications. In addition, although ASD was associated with cervical sagittal alignment in this study, it was radiological and did not affect the clinical results during the follow-up period. However, the fact that changes of cervical sagittal alignments were found on radiographs means that clinical outcomes may also be worse in the future.
Patients with ASD showed a significantly lower FSUA than those without ASD, and the average FSUA in the ASD patients was kyphotic. In addition, multivariate logistic regression analysis showed that poor segmental lordosis was a risk factor for ASD. This result demonstrates the importance of maintaining segmental lordosis in preventing ASD after Prestige-LP CDR. Similar results have been proved in cervical fusion surgery. Katsuura et al. 8 reviewed the radiological data of 42 patients who underwent anterior cervical fusion surgery and found that ASD was more likely to develop in patients with kyphotic segmental alignment after surgery. Xiong et al. 12 enrolled 130 patients who underwent ACDF and were followed up after at least 2 years and found that patients with postoperative segmental kyphosis were 2.8 times more likely to develop ASD than those with lordotic segmental alignment. The reason for this result might be that the stress distribution of the cervical spine can be altered by segmental kyphosis. Physiologically, the cervical spine transmits 64% of the axial loads through the posterior columns and 36% of the loads in the anterior columns. 28 However, the kyphotic segment might induce more forward-directed pressure on the adjacent intervertebral levels, which can affect the blood supply and nutrient diffusion in intervertebral discs and subsequently lead to ASD. 1
Cervical curvature is one of the key parameters in preserving the physiological function of the cervical spine. Harrison et al. found that hypolordosis of the cervical spine is significantly related to neck pain. 29 Similar findings were also reported by Iyer et al. 3 Kumagai et al. 5 found that C2–C7 alignment is significantly correlated with the degree of degeneration in cervical intervertebral discs. In the current study, although no significant difference was found in the postoperative degree of CL between patients with or without ASD and between patients with or without HO, the degree of CL was relatively worse in patients with AOH. In addition, for every 1° increase in the postoperative CL, there was an 8% reduction in the risk of complications when ASD and HO were considered together. Our results were consistent with those in the previous meta-analysis by Zhang et al., 11 who reviewed five studies and found that the postoperative degree of CL was significantly lower in patients who underwent anterior cervical spine surgery and developed ASD compared with those who did not develop ASD by the last follow-up. Based on our findings and those of previous studies, we believe that it is important to maintain normal cervical alignment after Prestige-LP CDR.
In this study, the other important parameter that was found to be associated with the outcomes of Prestige-LP CDR was the T1s. The T1 vertebra has been considered the foundation of the cervical spine, and the orientation of T1 (measured as T1s) is one of the determinants of global sagittal balance. 26 A small T1s has been shown to be a risk factor for nonspecific neck pain. 4 The relationship between T1s and outcomes of ACDF has been discussed in the literature. Iyer et al. 3 found that a larger T1s was correlated with lower preoperative NDI values for patients with CDDD. Lee et al. 10 found that patients with T1s <28° were more likely to develop implant subsidence after ACDF. Choi et al. 6 noticed that a larger T1s was a risk factor for pseudarthrosis after ACDF. However, there is only one study, which was conducted by Yang et al., 30 that reported the relationship between T1s and outcomes after CDR, and the results showed that a larger T1s was a risk factor for ASD and HO after CDR.
In contrast to the findings of Yang et al. 30 , we noticed that the postoperative T1s was significantly smaller in patients with ASD than in those without ASD, and a larger T1s was a protective factor for ASD. In addition, the T1s was found to not be related to HO. A possible explanation for our results might be that a larger T1s represents a more favorable cervical curvature when the SVA is in the normal range. 26,31 As shown in previous studies, there is a significantly negative correlation between the T1s and CL. 1,26,31 A larger T1s and more favorable CL may be helpful in maintaining the physiological load transmission pattern of the cervical spine. Otherwise, the load of the head may shift forward and lead to an increase in the intervertebral disc pressure, which can increase the risk of ASD, as we described earlier.
The association of ΔT1s with ASD and HO implied the importance of maintaining a good posture of the cervical spine after CDR. In the current study, the patients who had a consistent T1s from postoperation to the last follow-up were less likely to develop ASD or HO. However, every 1° decrease in the T1s at the last follow-up may increase the risk of ASD or HO by 5–10%. In our opinion, cervical spine misalignment after CDR may be related to a lack of muscle strength and unhealthy lifestyles. 32,33 According to Panjabi et al., 34 the neck muscles in the cervical spine account for approximately 75–80% of the mechanical stability, while the load of the osteoligamentous compartment is approximately 15–20% of the weight of the head. The neck muscles also help maintain the sagittal balance of the cervical spine. 35 Therefore, an unhealthy lifestyle (such as working for long periods of time at a desk and using a cell phone) and weak muscles can cause cervical sagittal parameters to worsen and affect the transmission of loads by the cervical spine, thus inducing the degeneration of the cervical spine after CDR.
Our study cannot directly conclude the importance of maintaining normal cervical alignment after Prestige-LP CDR by exercising neck muscles. However, this idea was supported by previous studies. First, the relationship between the paraspinal muscle volume and spinal alignment was reported by several studies. For instance, Tamai et al. 33 found that the cross-section area of paraspinal muscle showed significant positive correlations with C7 slope, neck tilt, and thoracic inlet angle. They also found the ratio of muscle area to vertebra area had a significant positive correlation with CL. Passias et al. 33 found that the number of cervical muscle composition was negatively correlated with SVA. Second, in open-door laminoplasty, the preservation or reconstruction of paraspinal muscles could help to maintain cervical sagittal balance after surgery. 36,37 Third, Tamai et al. 33 found that the paraspinal muscle volume was negatively correlated with intervertebral disc degeneration, which also explains the importance of exercising neck muscle. All these findings suggest the necessity of neck muscle exercising in maintaining cervical sagittal alignment. Together with the studies we described above, our work highlights the importance of maintaining normal cervical alignment after Prestige-LP CDR by exercising the neck muscles. However, further studies should be focused on the association of neck muscle exercising and postoperative complications after CDR.
Considering that ASD might be partially due to the natural history of preexisting degeneration that was not symptomatic at the time of surgery, we reviewed the preoperative radiographs of the included patients and identified 12 patients with preexisting ASD. Interestingly, we found the preexisting ASD was associated with HO (p = 0.008, OR 1.62, 95% CI 1.41–1.87). However, the preexisting ASD was not associated with postoperative ASD (p = 0.735). This result may be because of the small sample size and the retrospective, single-center design. Further studies could focus on this topic.
It should be noted that the malposition of cervical artificial discs could also lead to complications. Kim et al. 38 reported that the coronal tilting of the artificial disc was associated with HO and ASD. Suchomel et al. 39 found that implant with a more posterior located center of rotation was at higher risk for developing ROM-limiting HO. Park et al. 40 reported seven patients who received revision surgery after CDR due to malposition of artificial discs and HO. They hypothesized that malposition of artificial discs may cause damages to the normal kinematics of implants, which may lead to abnormal biomechanical stress at the surgical level. In addition, Park et al. 40 reported that the progression of facets degeneration after lumbar disc replacement was positively related with malposition of the implant on the coronal plane. All these findings indicate the importance of properly positioning artificial disc during CDR. In our experience, we take the following measures to ensure the proper position of artificial discs. First, we use a level to make sure the surgical bed is absolutely horizontal. Then the patient is placed in the neutral position, and intraoperative radiographic confirmation should be done to make sure the patient is well positioned on the surgical bed. To achieve perfect intraoperative radiographs, the c-arm should be adjusted to ensure the uncovertebral joints at the operated level are symmetrical on the anterior–posterior view, and the facet joints at the operated level are overlapping on the lateral view. Next, the Caspar pins are centrally inserted with the help of a self-made tool. The perfectly inserted Caspar pins can be used as markers for midline for where the implant would be inserted. 41 In addition, intraoperative radiographic confirmation is performed during each step of the implantation process. 42 All these procedures guarantee a proper position of the implanted artificial discs.
To the best of our knowledge, this is the first study to evaluate the association of cervical sagittal alignment with ASD and HO after Prestige-LP CDR. We found that postoperative segmental kyphosis may be a risk factor for ASD, and poor CL is related to AOH after CDR. We also found that both T1s and ΔT1s are key factors in preventing ASD and HO after CDR. In addition, these findings were confirmed by multivariate logistic regression analysis. Our study suggests that maintaining cervical sagittal alignment is necessary to guarantee good outcomes after Prestige-LP CDR.
There are several limitations in the current study. First, the average follow-up time was short, which may lead to the underestimation of the occurrence of ASD and HO. During the study period, no patient had symptoms and “adjacent segment disease,” while the latter is more meaningful in clinical practice. The ranges of the postoperative follow-up period were relatively big, which may have led to bias in our results. The single-center and retrospective design of this study also limited the generalizability of the results. However, the relationship between postoperative cervical sagittal alignment and complications has been identified. Therefore, our study may be clinically significant. Another limitation is that we only discussed these relationships in terms of regression analysis, and we did not calculate cutoff values to predict the occurrence of ASD or HO. In addition, cervical sagittal parameters can compensate for each other so that the individual can maintain a horizontal gaze. However, we did not measure the parameters that represent the stress on the cervical spine required to maintain a horizontal gaze, such as the occipito-cervical inclination, chin-brow to vertical angle, and C2 slope. 1,21,43 Other limitations included the lack of a control group and small sample size. Future studies with long-term follow-ups and assessments of multiple parameters are needed to overcome the above limitations.
Conclusion
Cervical sagittal alignment is important in preventing ASD and HO after Prestige-LP CDR. Reduced segmental lordosis and small T1s are risk factors for ASD, and poor CL is a risk factor for AOH. A decrease in the T1s at the last follow-up is related to the development of ASD and HO. The results imply the importance of maintaining cervical sagittal alignment after Prestige-LP CDR.
Supplemental material
Supplementary_table_1 - Association of cervical sagittal alignment with adjacent segment degeneration and heterotopic ossification following cervical disc replacement with Prestige-LP disc
Supplementary_table_1 for Association of cervical sagittal alignment with adjacent segment degeneration and heterotopic ossification following cervical disc replacement with Prestige-LP disc by Xiaofei Wang, Yang Meng, Hao Liu, Hua Chen, Beiyu Wang and Ying Hong in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
The authors appreciate the warm work of editors and reviewers earnestly.
Author contributions
XW and YM should be considered co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Post-Doctor Research Project, West China Hospital, Sichuan University (2018HXBH002); West China Nursing Discipline Development Special Fund Project, Sichuan University (HXHL19016); and 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC18029).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.