
Abstract
Study Design
Systematic review and meta-analysis.
Objective
To compare clinical and radiographic outcomes as well as complications of unplated vs plated anterior cervical discectomy and fusion (ACDF) surgery considering the role of osteobiologics in single- and multi-level procedures.
Methods
A systematic search of PubMed/MEDLINE, Scopus, CINAHL, EMBASE, CENTRAL, Cochrane and ClinicalTrials.gov databases was performed. Briefly, we sought to identify studies comparing unplated vs. plated ACDF for cervical degenerative disc disease reporting the use of osteobiologics in terms of clinical outcomes, radiographic fusion, and complications. Data on study population, follow-up time, type of cage and plate used, type of osteobiologic employed, number of levels treated, patient-reported outcomes (PROs), radiographic outcomes and complications were collected and compared. Relevant information was pooled for meta-analyses.
Results
Thirty-eight studies met the inclusion criteria. No significant difference was found in terms of clinical outcomes between groups. Unplated ACDF was characterized by reduced blood loss, operation time and length of hospital stay. Fusion was achieved by the majority of patients in both groups, with no evidence of any specific contribution depending on the osteobiologics used. Dysphagia was more commonly associated with anterior plating, while cage subsidence prevailed in the unplated group.
Conclusion
Unplated and plated ACDF seem to provide similar outcomes irrespective of the osteobiologic used, with minor differences with doubtful clinical significance. However, the heterogeneity and high risk of bias affecting included studies markedly prevent significant conclusions.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is one of the most popular treatments for cervical degenerative disc disease. 1 Historically, interbody fusion in ACDF procedures has been achieved by using different grafts. Autologous bone graft is considered the gold standard due to its optimal osteoconductive, osteoinductive and osteogenic properties, but is often complicated by donor site morbidity. Furthermore, loss of such properties due to decreasing number of stem cells and growth factors during ageing can also occur. 2 As an alternative, allogeneic bone grafts are associated with decreased operative time and no donor site morbidity, but are accompanied by higher costs and risks of graft rejection, nonunion, host immune response, and disease transmission. 3 Nevertheless, no statistical differences in clinical outcomes were described in different studies comparing autograft vs. allograft both in single and multi-level ACDF.4-6 Synthetic interbody cages have been introduced to overcome aforementioned limitations while assuring an acceptable degree of osteointegration. To date, different cage designs and materials (e.g., polyetheretherketone – PEEK -, titanium, carbon fiber, ceramics, biodegradable materials) are available and can be utilized alone or in combination with diverse osteobiologics (e.g., bone marrow aspirate – (BMA), demineralized bone matrix (DBM), hydroxyapatite, bone morphogenetic protein (BMP), beta tricalcium phosphate (β-TCP)) to promote spine fusion. 7 The tunability and advantages of these constructs have significantly increased their popularity to such an extent that PEEK cages have recently demonstrated to be the most commonly used interbody cage for both simple (84%) and complex ACDF (68%) worldwide. 7 Anterior plating is routinely performed during ACDF to increase fusion rate and construct stability as well as to maintain segmental lordosis, 8 but is associated with increased risk of dysphagia, adjacent segment degeneration (ASD) and hardware failure. 9 Different unplated approaches have been described to decrease abovementioned complications, although incrementing the risk of graft subsidence and pseudarthrosis.10,11 These strategies include the use of non-fixed grafts or cages equipped with locking screws inserted into the contiguous vertebral bodies (ie., zero-profile, stand-alone or anchoring cages). The latter have been showed to decrease intraoperative blood loss, dysphagia and ASD compared to the use of plated systems, with no significant differences in terms of clinical outcomes and fusion rate. 12 However, the most systematic reviews and meta-analysis conducted on the topic conclude that the significant degree of heterogeneity and variability across investigations strongly limits the formulation of general recommendations on the type of graft and osteobiologic to be used in ACDF surgery.10,11,13 The aim of this study was to systematically review patient-reported outcomes (PROs), radiographic fusion and perioperative outcomes in unplated ACDF constructs vs. plated constructs in single- and multi-level procedures considering the role of different osteobiologics.
Materials and Methods
The methods for this systematic review followed accepted standards for systematic review/comparative effectiveness reviews for rigor, quality, and transparency including those described by the Agency for Healthcare Research and Quality (AHRQ), 14 IOM Standards for Systematic Reviews, 15 and the PCORI Methods Guide. 16
Electronic Literature Search
A systematic search of PubMed/MEDLINE, Scopus, CINAHL, EMBASE, CENTRAL, Cochrane and ClinicalTrials.gov databases was performed on November 1st, 2020 for literature published through January 2000 and November 1, 2020. The primary outcome of the study was the evaluation of bone fusion rate in patients undergoing unplated vs. plated ACDF based on the use of different osteobiologics. Secondary outcomes included the assessment of additional relevant radiological parameters, perioperative outcomes (blood loss, length of hospital stay and complications), and PROs (pain, satisfaction, disability). The search strategy with the Medline string, PICO approach, study inclusion and exclusion criteria, list of complications and osteobiologics included are reported in Appendix A within Supplementary Materials. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were used to improve the reporting of the review as described by Moher et al. 17 The definition of radiographic fusion was reported according to the study by Rhee et al. 18 The review protocol has been approved by the International Prospective Register of Systematic Reviews (PROSPERO) under the ID CRD42021256607.
Study Selection
The initial search of the article was conducted by two reviewers (S.D.S. and L.A.). In case of disagreements, the third reviewer (G.V.) was included. The following research order was used: titles were screened first, then abstracts and full papers. The full text of all papers not excluded based on abstract or title was evaluated. The number of articles excluded or included were registered and reported in a PRISMA flow diagram (Figure 1).
19
Search strategy flow diagram in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol.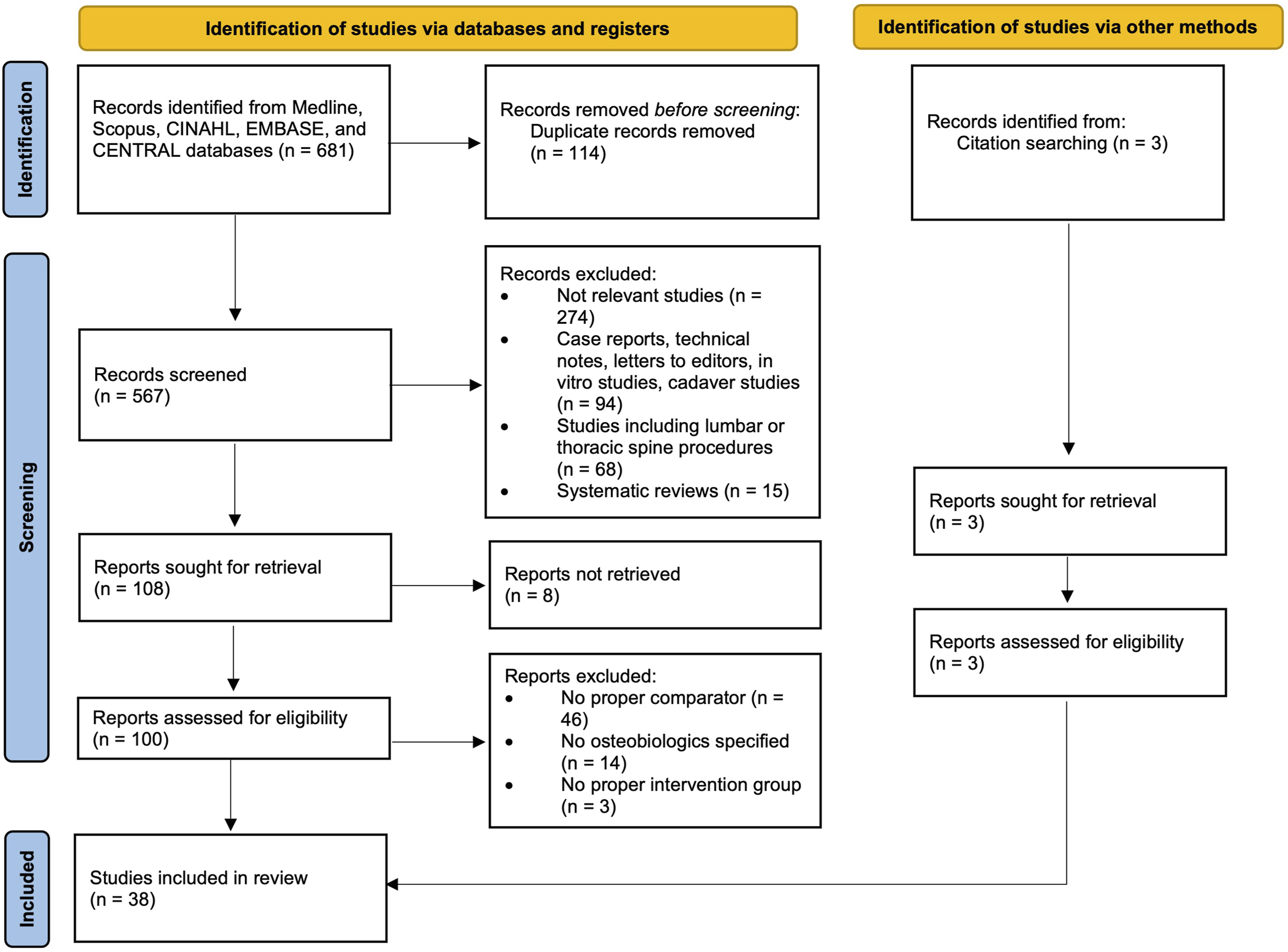
Data Extraction
General study characteristics extracted were: authors, country, sample size, mean age, mean follow-up, study design, level of evidence (LOE), year of publication, intervention (zero-profile or cage alone), comparator (cage or graft + plating), type of osteobiologic used, number of levels treated, and PROs including visual analogue scale (VAS), Japanese Orthopaedic Association score (JOA) or modified JOA (mJOA) score, Neck Disability Index (NDI), Oswestry Disability Index (ODI), Odom’s criteria, Short Form-36 (SF-36), Patient Satisfaction Index (PSI), Robinson’s criteria and Prolo Scale. In addition, mean operation time, mean intraoperative blood loss, fusion rate, additional radiological outcomes, mean length of hospital stay (LOS), complications and conclusions of the studies were reported.
Risk of Bias
The RoB-2 20 for randomized controlled trials (RCTs) and the Methodological Index for NOn-Randomized Studies (MINORS) 21 tool for non-randomized RCTs (NRCTs) were utilized to assess the quality of studies. To avoid imprecisions, selected papers were rated independently by two reviewers (S.D.S. and L.A.) and verified by the a third reviewer (G.V.). The “Robvis” tool was utilized to generate the traffic light plot in accordance with Cochrane recommendations. Publication bias was evaluated using funnel plots for each analyzed outcome (Supplementary Figure 2).
Quality of Evidence
For the primary outcomes of pain, disability, satisfaction, fusion rate, and dysphagia the overall strength of evidence across included studies was assessed using the precepts outlined by the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group (Figure 2).
22
The overall quality of evidence was based on studies at the lowest risk of bias. In determining the quality (strength) of a body of evidence regarding a given outcome, the overall quality may be downgraded 1 or 2 levels based on the following domains: (1) risk of bias due to study limitations, (2) consistency (heterogeneity) of results, (3) directness of evidence, (4) precision of effect size estimates, and (5) publication or reporting bias. The initial quality of the overall body of evidence begins as “High” for RCTs and “Low” for observational studies. As the majority of included studies was observational and the few RCTs were characterized by a considerable risk of bias, the initial quality of the overall body of evidence was set as “Low”. GRADE evidence and summary of findings.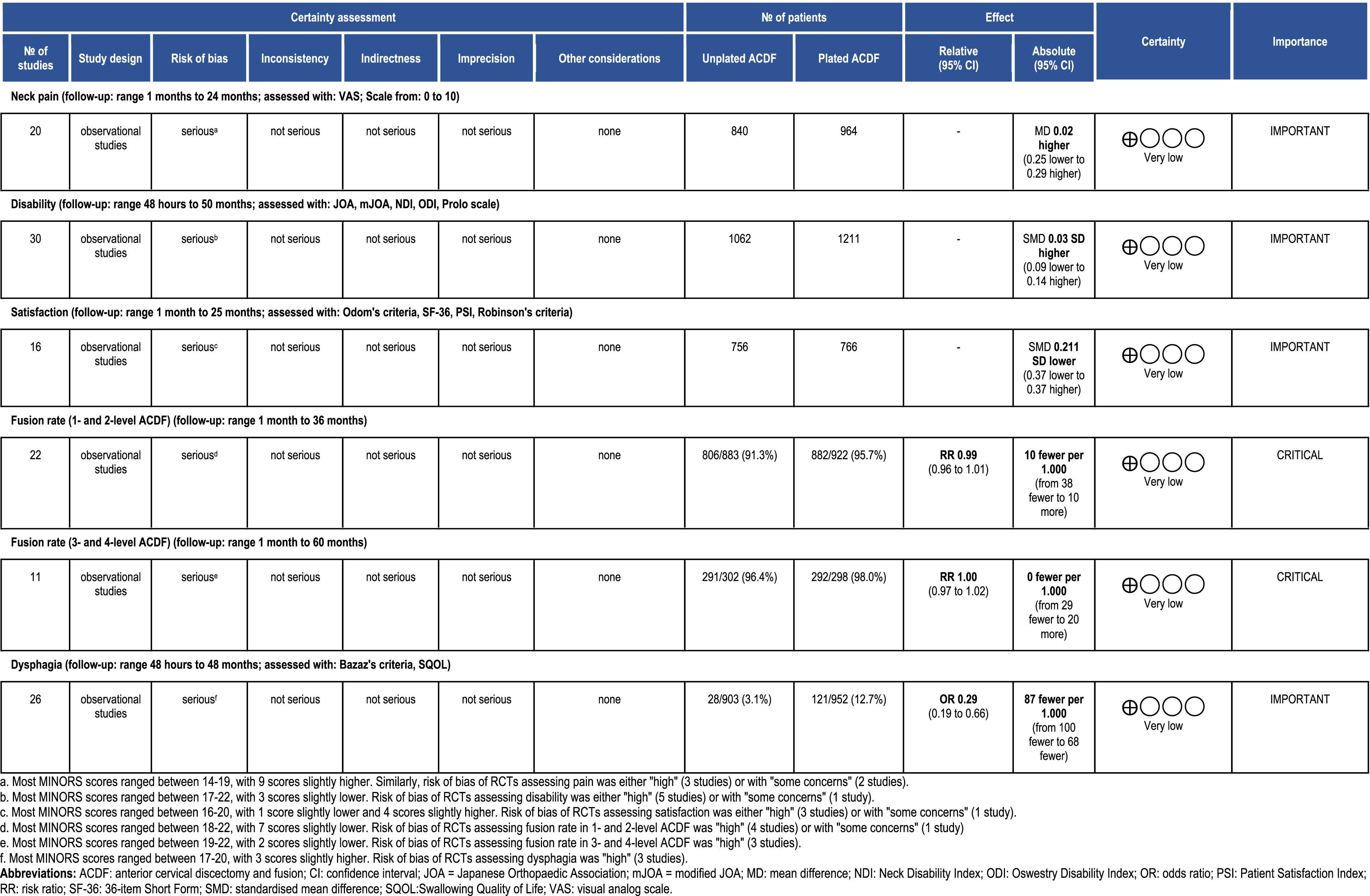
Statistical Analysis
Meta-analysis was performed using mean differences (MD) with 95% confidence intervals (Cl) to describe continuous variables and odds ratios (OR) to describe dichotomous variables. If a study describing a continuous outcome did not report corresponding standard deviations, it was excluded from meta-analysis. 23 In case of missing events in either group, risk ratios (RR) were utilized to describe dichotomous variables. When outcomes were described by both continuous and dichotomous variables, standardized mean differences (SMD) were employed for the analysis. 23 Pooled estimates were calculated by random effects models and the inverse variance method for pain, disability, satisfaction, and dysphagia outcomes, while the Mantel-Haenszel method was used for the fusion rate outcome. The level of significance was set at .05. Heterogeneity among comparisons was calculated by the I2 statistics, classified as “low” (I2 ≤ 25%), “moderate” (I2 = 26-74%), or “high” (I2 ≥ 75%). The analysis was performed using Review Manager version 5.4 (Cochrane Collaboration, UK).
Results
Study Selection
A total of 681 studies were found. 567 studies were obtained after duplicate removal and 467 articles were excluded through title and abstract screening. Then, 100 full-text articles were screened. Out of these studies, 70 were excluded (full-text not available, n = 8; no proper comparator, n = 46; no osteobiologic specified, n = 14; no cage in the intervention group, n = 3; systematic review, n = 5; sample size < 10, n = 2). Three additional studies were identified from hand searching bibliographies of included studies or identified systematic reviews. After this process, 38 articles were included.
Study Characteristics
Study Design and Patient Demographics of Included Studies.
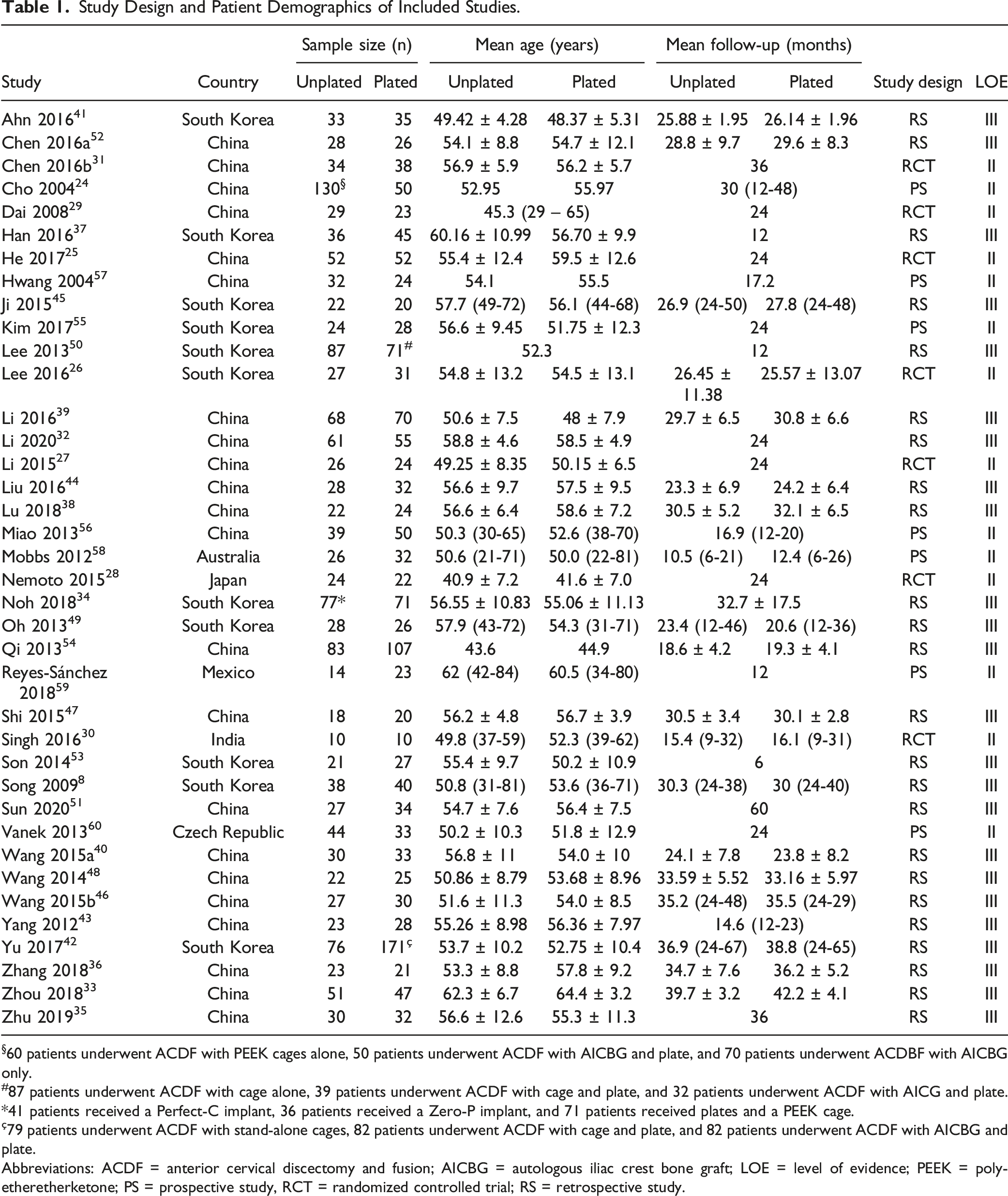
§60 patients underwent ACDF with PEEK cages alone, 50 patients underwent ACDF with AICBG and plate, and 70 patients underwent ACDBF with AICBG only.
#87 patients underwent ACDF with cage alone, 39 patients underwent ACDF with cage and plate, and 32 patients underwent ACDF with AICG and plate.
*41 patients received a Perfect-C implant, 36 patients received a Zero-P implant, and 71 patients received plates and a PEEK cage.
ç79 patients underwent ACDF with stand-alone cages, 82 patients underwent ACDF with cage and plate, and 82 patients underwent ACDF with AICBG and plate.
Abbreviations: ACDF = anterior cervical discectomy and fusion; AICBG = autologous iliac crest bone graft; LOE = level of evidence; PEEK = polyetheretherketone; PS = prospective study, RCT = randomized controlled trial; RS = retrospective study.
Risk of Bias
For RCTs, we found 2 studies with an overall risk of bias identified as “some concerns”28,29 and 6 as “high risk”24-27,30,31 (Supplementary Figure 1). The MINORS tool was adopted to assess the quality of evidence of included NRCTs, with a mean total score of 18.14/24 (Supplementary Table 1). No significant publication bias was detected for most outcomes, except for satisfaction (Supplementary Figure 2).
Osteobiologics
DBM was utilized in 7 studies.33,37,42,43,45,49,55 β-TCP was used alone27,29,32,51,56,60 and in combination with HA41,58 or locally excised osteophytes. 47 AICBG was employed in the form of milled cancellous bone8,25,28,30,46,48,59 or as a tricortical interbody graft.24,30,42,50 Allograft was used exclusively 53 or as an alternative to AICBG. 50 Local autologous bone graft was utilized alone,31,39,54 in combination with a calcium sulfate graft, 57 or with .25 mg rhBMP-2.36,38,40,44 In the study by Noh et al. 34 1 cm3 of a graft containing both DBM and rhBMP-2 was utilized alone to fill cages in all treated patients. Chen et al. 52 used a porous bioceramic artificial bone graft to fill the cages, while Zhu et al. 35 adopted an unspecified synthetic bone graft. In the study by Lee and coauthors, 26 cages were filled with a mixture of type I collagen and HA soaked in BMA harvested from the iliac crest.
Operation Time
Operation time was reported in 23 studies.24,25,27-29,32-36,38-40,43,44,46-48,51-54,59 ACDF without anterior plating resulted in a shorter operation time in most studies compared to plated procedures,24,28,29,32-36,38-40,43,44,46,51,52 whereas only a few studies reported no significant differences between the two groups.25,48,53,54,59 Only 2 studies reported a longer mean operation time in the unplated group compared to the plated group.27,47
Blood Loss
Mean intraoperative blood loss was reported by 23 studies.24,25,27-29,32-36,38-40,43,44,46-48,51-54,59 In 11 studies, unplated procedures were characterized by a significantly lower amount of blood loss compared to plated surgeries,24,25,33,34,39,40,44,46,51-53 while no significant differences in terms of intraoperative blood loss were reported in remaining studies.27-29,32,35,36,38,43,47,48,54,59
Length of hospital stay
LOS was reported in days in 8 studies.29,34,35,39,51,57,58 Noh et al. 34 reported that patients treated with Perfect-C or Zero-P stand-alone cages had a significantly lower LOS compared to the plated group. Similarly, Hwang et al. 57 showed that patients in the unplated group tended to have an inferior LOS if compared to patients undergone anterior plating. Likewise, in another study by He and colleagues, 25 LOS in the unplated group was lower than in the plated group. However, no significant difference in terms of LOS was reported in other studies.29,35,39,51,58
Radiographic Fusion
Twenty-nine assessed radiographic fusion following ACDF with or without anterior plating. Bone fusion was mainly defined based on the presence of bridging trabecular bone between the endplates,24,26,27,29-33,35,36,38-40,42-46,49,51,54,55,57,58,60 absence of a radiolucent gap between the cage or graft and the endplate,24,27,29,31-33,35,36,38-40,42-47,49,54,55,57,58 limited angular motion or translation between vertebral bodies at fused segments at flexion-extension X-rays24,27,29,39,45,47,49,51,54,55,57,58,60 or limited motion between spinous processes at fused segments at flexion-extension X-rays30-36,38,40-44,50,54 (Supplementary Table 4). These criteria were consistent with the ones defined by the study of Oshina et al. 61
22 studies investigated fusion rate in 1- and 2-level ACDF, while 11 studies assessed such an outcome in 3- and 4-level ACDF. According to our meta-analysis, no significant differences were found between unplated and plated ACDF surgeries at both 1 and 2 levels (overall pooled RR = .99, 95% CI = .96 to 1.01, P = .24, I2 = 0%; Figure 3A) as well as at 3 and 4 levels (overall pooled RR = 1.00, 95% CI = .97 to 1.02, P = .78, I2 = 0%; Figure 3B). Following 1- and 2-level ACDF, 98.1% of patients achieved a solid fusion in the unplated group and 98.8% in the plated group, with reported fusion rates ranging from 50% and 75% at 1 month,
24
72-100% and 87.5-100% at 3 months,24,29,36,38,40,58 41.6-100% and 64.1-100% at 6 months,24,29,50,58 63.2-100% and 79.5-100% at 1 year,24,50 100% and 100% at 18 months,
54
78.8-100% and 91.4-100% at 2 years,32,33,36,38,39,41,45,49,55,60 86-100% and 90.3/100% at 3 years,26,34,42 100% and 100% at 4 years
46
in unplated and plated groups, respectively. Following 3- and 4-level ACDF, 96.4% of patients achieved a solid fusion in the unplated group and 94.7% in the plated group, with reported fusion rates ranging from 50% and 75% at 1 month,
24
72-100% and 87.5-100% at 3 months,24,44,47 72-100% and 92-100% at 6 months,24,43 87-100% and 91.7-100% at 1 year,24,43,51,57 100% and 100% at 18 months,
54
91.2-100% and 92.9-100% at 2 years,33,39,47 93.3-100% and 94.7-100% at 3 years,31,35 100% and 100% at 5 years
51
in unplated and plated groups, respectively. Collectively, most included studies did not report significant differences in terms of fusion rate between patient treated with unplated or plated ACDF at the analyzed timepoints. When analyzing fusion rates based on the diverse osteobiologics used, no significant differences were found. In studies using DBM alone, fusion rate were 100% vs 100% at 3 years,
33
91.3% vs 96.4% at 1 year,
43
95% vs 100% at 2 years,
45
96.43% vs 96.15% at 2 years,
49
and 82.4% vs 94% at 2 years
55
in unplated and plated groups, respectively. The use of β-TCP led to fusion rates of 100% vs 100% at 6 months
29
and at 2 years,32,60 and 92.59% vs 97.06% at 1 year
51
in unplated and plated groups, respectively. β-TCP was also employed in combination with HA (leading to fusion rates of 78.8% vs 91.4% at 2 years
41
and 96.2% vs 100% at 6 months
58
between the two groups) or local autologous bone graft (with fusion rates of 83.3% in the unplated group and 90% in the plated group at 6 months and 100% in both groups at 2 years
47
). Milled AICBG packed into the cages was associated with fusion rates of 78.9% vs 97.5% at 2 years,
8
92% vs 96% at 1 year and 96% vs 100% at 2 years,
28
and 100% vs 100% at 3 months
46
in unplated and plated groups, respectively. AICBG employed as a structural tricortical interbody graft alone resulted in fusion rates of 87%, while the addition of plating increased such ratio up to 98% at 1 year.
24
In the study by Singh et al.
30
both unplated patients treated with milled AIBCG-filled cages and plated patients with interbody tricortical AICBG reached a 100% fusion rate at 6 months. Yu et al.
42
compared the fusion rate of cages filled with DBM with or without plating and interbody tricortical AICBG with anterior plating, resulting in 97.37%, 96.34% and 97.78% fused segments at 2 years, respectively. Similarly, Lee and colleagues
50
compared fusion in allograft-filled stand-alone cages with or without plating and AICBG with anterior plating. At 6 months, fusion rate was 41.6%, 64.1% and 70%, while at 1 year it reached 63.2%, 79.5% and 87.1%, respectively. Conversely, Hwang et al.
57
reported that the use of cages filled with autologous bone graft chips and calcium sulfate graft was associated with a fusion rate of 90.6% in the unplated group and 91.7% in the plated group. The use of .25 mg rhBMP-2 with autologous bone graft led to fusion rates of 91.3% vs 95.2%
36
and of 86.4% vs 87.5%
38
at 3 months, and 100% vs 100% at 6 months40,44 and 3 years36,38 in unplated and plated patients, respectively. In their study, Noh et al.
34
used 1 cm3 of a graft containing both DBM and rhBMP-2, resulting in complete fusion in 88% unplated patients and 95% plated patients at 3 years. Zhu and coauthors
35
adopted an unspecified artificial bone graft and reported a fusion rate of 93.3% and 94.7% in unplated and plated groups, respectively. Lee et al
26
filled the cages with a blend of type I collagen, HA and BMA harvested from the iliac crest, which led to complete fusion in 88.9% unplated patients and 90.3% plated patients at 6 months. Forest plots of radiographic fusion rates following 1- and 2-level (A) and 3- and 4-level ACDF in unplated vs. plated surgeries. (B).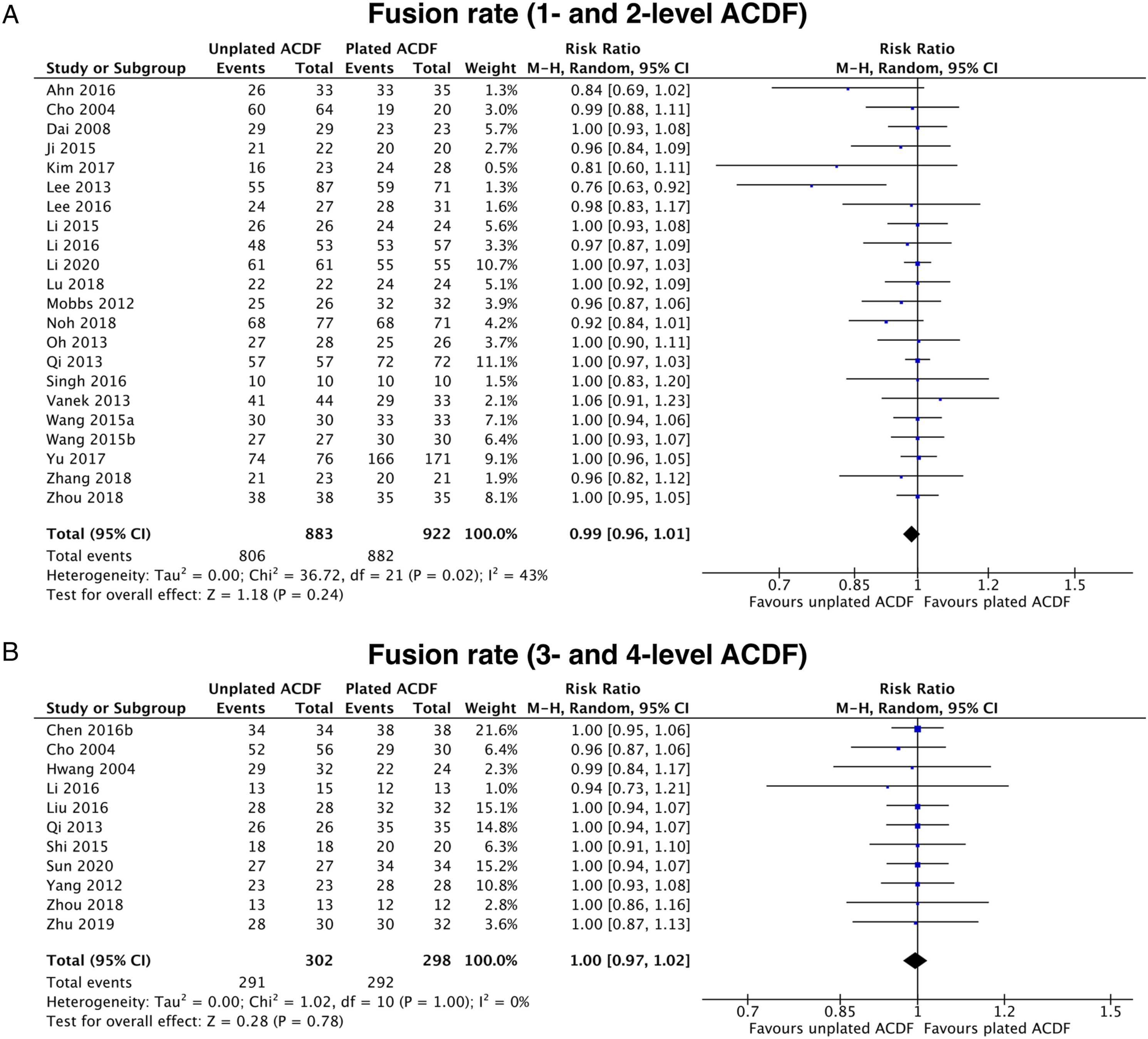
Additional Radiological Parameters
Cervical alignment (CA) was the most investigated radiological parameter in included studies and was calculated as the Cobb angle between C2 and C7 lower endplates in a plain lateral X-ray. The majority of studies assessing CA showed no significant difference between unplated and plated patients.25,28,29,31-34,36-41,43,44,46,47,49,54-57,60 Contrariwise, other studies reported a more substantial preservation of CA in the plated group, especially at later follow-ups.35,42,51,59 Similar to CA, most studies did not report a significant difference in terms of segmental angle between unplated and plated groups.8,28,29,32,34,35,41,49,50,52,59 No significant difference between groups was detected in all included studies34,35,37,38,41,42,50,57,60 except Li et al. 39 who reported a higher reduction of segmental height in the unplated group compared to the plated group only at the final follow-up. Disc height was not significantly different between groups in most studies.8,25,34,40,49,55,59 Prevertebral soft tissue swelling (PSTS) was defined as the distance between the anterior margin of fused segments and the posterior margin of the trachea in a plain lateral X-ray. No significant difference was reported in most studies28,34,53 except in Yang et al. 43 who detected an increased PSTS in the plated group at 48 h and 2 months, although no difference was seen at 6 months.
Dysphagia
Dysphagia was evaluated by the Bazaz’s criteria (17 studies8,27,28,31,34-36,38-40,43,44,46-48,52,56), the Swallowing Quality of Life (SWAL-QOL) questionnaire (3 studies31,43,54) and only mentioned in other studies.25,30,33,51,53,57,58,60 Considering intermediate timepoints as more representative of surgery-related outcomes, dysphagia was reported in 28/903 (3.1%) patients in the unplated group and 121/952 (12.7%) patients in the plated group. This difference was statistically significant from meta-analysis of pooled results of included studies (overall pooled OR = .29, 95% CI = .19 to .43, P < .00001, I2 = 0%; Figure 4). Indeed, most studies showed an increased risk of dysphagia following anterior plating, although symptoms tended to be progressively relieved with time.27,33,35,36,38,39,43,44,48,51,53 In the study of Qi et al.
54
dysphagia evaluated with the SWAL-QOL questionnaire was increased in both groups post-operatively without any statistical significance. Subsequently, scores improved more steadily in the unplated group at 2 months, 6 months and at the final follow-up, even if the difference was statistically significant only at the 3 month-timepoint. Likewise, Wang et al.
40
showed no significant difference between groups in terms of dysphagia at 2 weeks after surgery, although statistical significance was reached at 6 months. Similarly, Miao,
56
Mobbs,
58
Singh
30
and coauthors reported a decreased incidence of post-operative dysphagia in the unplated group, even though no statistical analysis was performed. Conversely, no significant intergroup difference at any timepoint was reported in remaining studies.8,28,31,46,52,60 Forest plot of dysphagia following unplated vs. plated ACDF.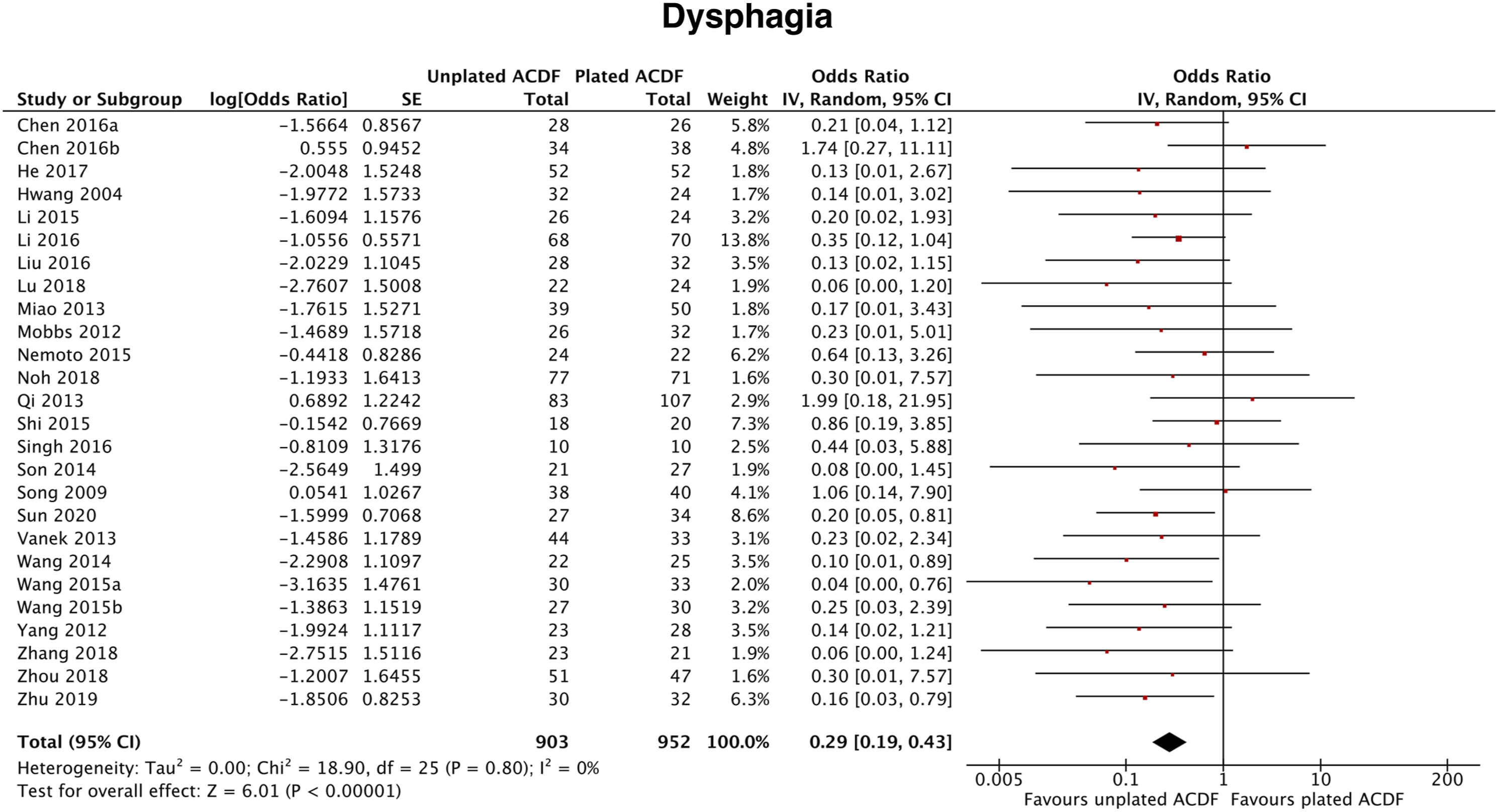
Complications
The most commonly reported complication was cage subsidence, which was significantly more frequent in the unplated group in the majority of studies,8,24,29,35,37,42,47,49-52,55 with values ranging from 3.70-66.6% compared to 0-47.06% in the plated group. However, no statistically significant difference between the two groups was reported in other studies.28,33,34,38,39,41,57 Cage subsidence was also more pronounced in the unplated group in other studies,30,57-59 although no statistical analysis was performed. Adjacent level ossification development (ALOD) was described in 3 studies28,31,34 and was significantly more frequent in the plated group, with rates ranging from 22.58-63.6% compared to 0-12.5% in the unplated group. Other less frequently described complications included nerve injury, cerebrospinal fluid leak, pseudoarthrosis, hardware migration, implant loosening, epidural hematoma, and were not significantly different between groups.25,33,35,38,39,42,51,54,57,58 While no intergroup significant difference in terms of ASD was described in some studies,8,35,38,41,44,48,49,58 others reported an increased ASD rate in the plated group (2.8-24%) compared to unplated patients (0-15.9%).27,33,36,51
Pain
Neck and arm pain were evaluated using the VAS scale in 20 studies.8,26-30,32,34,35,37,39,41,42,50,54-59 All studies reported a significant improvement of pain in both unplated and plated groups compared to preoperative baseline at all subsequent follow-up timepoints. Furthermore, no statistical difference in terms of pain intensity was detected between the two groups in most studies. This was also demonstrated by meta-analysis of pooled VAS values from included studies (overall pooled MD = .02, 95% CI = −.25 to .29, P = .89, I2 = 83%; Figure 5). Differently, Ahn et al.
41
reported that VAS scores for neck pain were significantly higher at 12 months and 24 months in the unplated group compared to patients treated with anterior plating. Conversely, no significant difference was found regarding arm pain. Similarly, Song et al.
8
showed that VAS scores for arm and neck pain were comparable in the two groups until 6 months post-operatively, whereas VAS scores resulted significantly lower in the group treated with cage and plate compared to the unplated group at 12 and 24 months. Likewise, Zhu et al.
35
reported that the neck pain VAS score was significantly higher in the unplated group compared to the plated group at 3 years, but not earlier. In the study by Kim et al.
55
VAS scores for arm pain were not significantly different between the cage-only and the cage-with-plate groups treated with 1-level ACDF, while in patients treated with a 2-level fusion the score was significantly lower in the unplated group only at the 12 month-timepoint, with not significant scores at all other timepoints. Lee et al.
50
reported that patients undergone ACDF with cage or AICBG and plate showed better mean VAS neck pain and arm pain scores compared to patients treated with a stand-alone cage at 6 months and 12 months. In another study, Reyes-Sanchez et al.
59
reported that the mean VAS score was significantly lower in patients treated with a PEEK cage alone compared to patients fused with a plate-graff or plate and cage after 1 year. On the other hand, Yu and colleagues
42
showed that post-operative VAS score for neck pain was significantly lower in patients treated with cage alone and cage and plate compared to patients with AIBCG and plate, except at the final follow-up. Forest plot of pain following unplated vs. plated ACDF.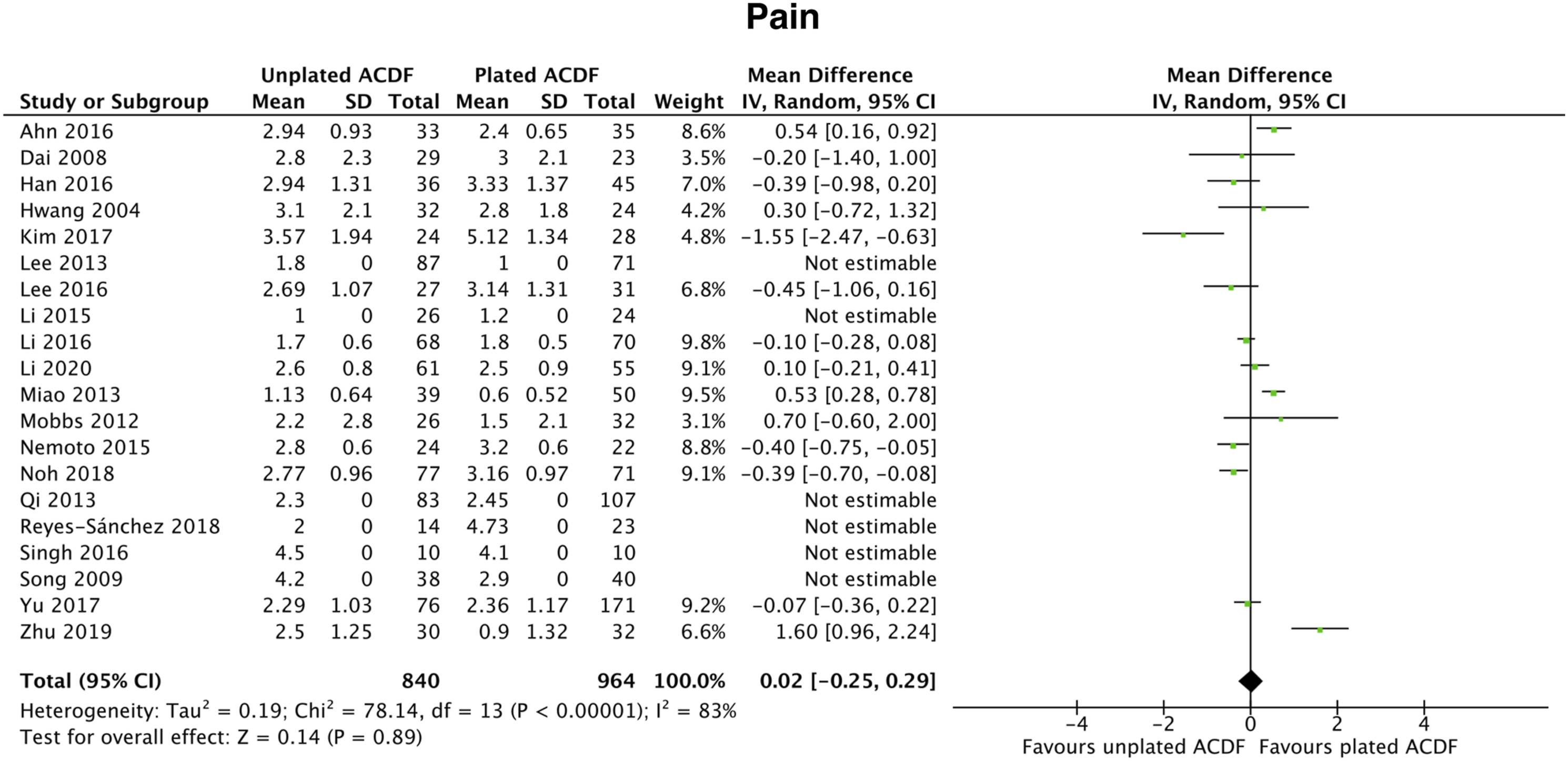
Disability
Disability was evaluated by the JOA (19 studies25,27,29,31-33,35,36,38-40,43,44,46-48,52,56,57), mJOA (2 studies51,53), NDI (21 studies25,26,31,33-36,38-40,42-44,46,47,51,52,54,55,59,60), ODI scores (1 study
58
) and Prolo Scale (1 study
24
). All studies reported a significant improvement of overall function in both unplated and plated groups compared to preoperative baseline at all subsequent follow-up timepoints. Furthermore, no statistical difference in terms of disability was encountered between the two groups in most studies, except two. In the study by Kim et al.
55
NDI scores were significantly lower in the unplated group compared to the plated group following 1-level ACDF at 3 months, 12 months and 24 months. However, no statistical difference was detected in terms of NDI score in patients undergone 2-level ACDF in both groups. Similarly, Reyes-Sanchez et al.
59
reported that patients treated with a PEEK cage alone showed a significantly lower mean NDI score at 1 year compared to patients treated with anterior plating. In the study by Cho et al.
24
authors reported that post-operative function and working status assessed with the Prolo scale were better in the cage-only group than in the AICBG only group. However, there were no statistically significant differences between the cage-only and the plated group. Overall, this was reflected by the results of our meta-analysis (overall pooled SMD = .03, 95% CI = −.09 to .14, P = .64, I2 = 0%; Figure 6). Forest plot of disability following unplated vs. plated ACDF.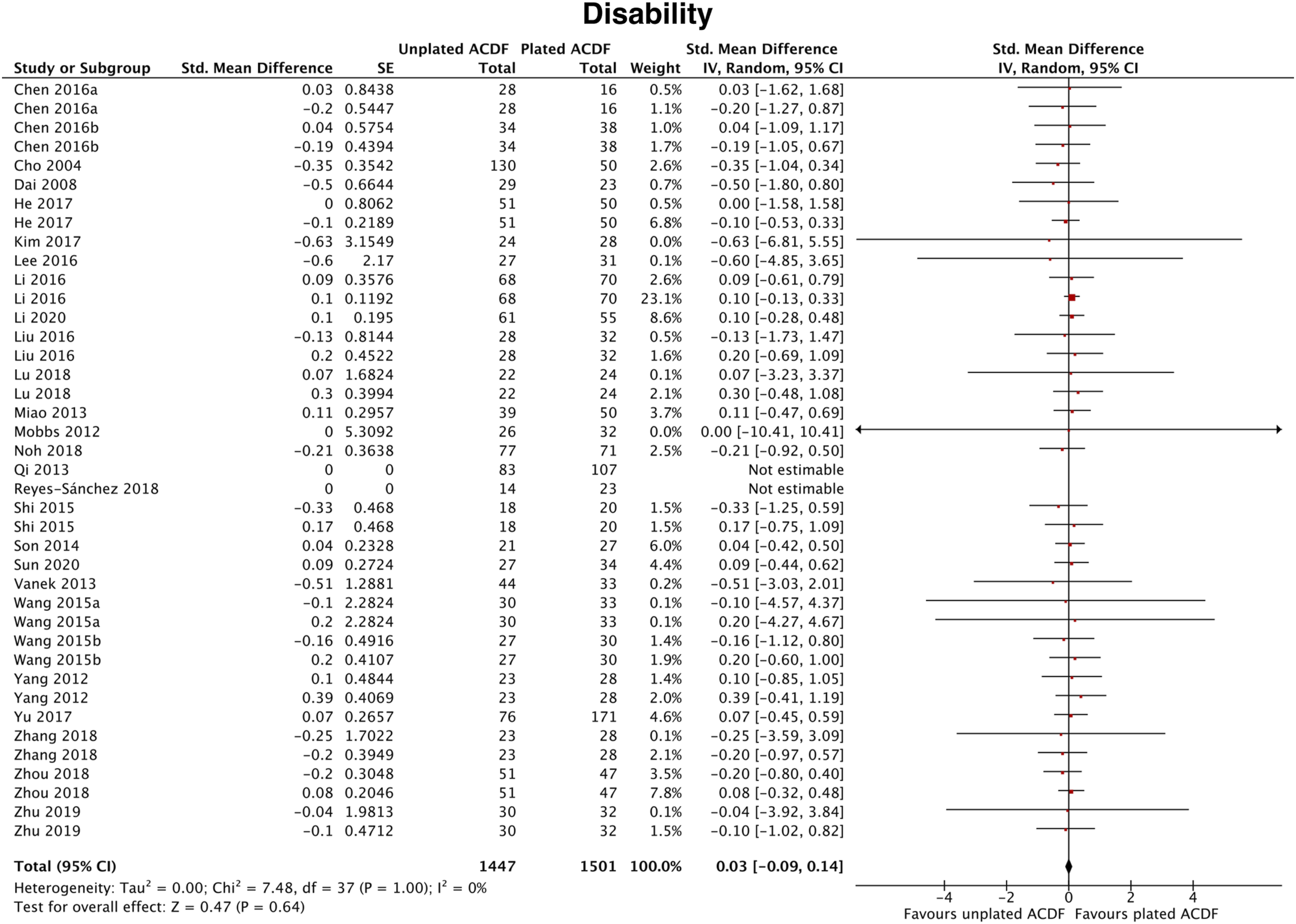
Satisfaction
Patient satisfaction was evaluated by Odom’s criteria (10 studies28,30,33,35,44,50,52,56,58,60), SF-36 (2 studies39,51), PSI (1 study
58
), and Robinson’s criteria (4 studies8,42,45,49). All studies reported that patient satisfaction was substantially achieved after surgery in both unplated and plated groups, with “good” to “excellent” outcomes an improved functional status compared to preoperative conditions. Interestingly, no statistical difference was encountered between the two groups in all included studies. This was also confirmed by meta-analysis of pooled data from included studies (overall pooled SMD = -.11, 95% CI = -.37 to .15, P = .40, I2 = 93%; Figure 7). Forest plot of satisfaction following unplated vs. plated ACDF.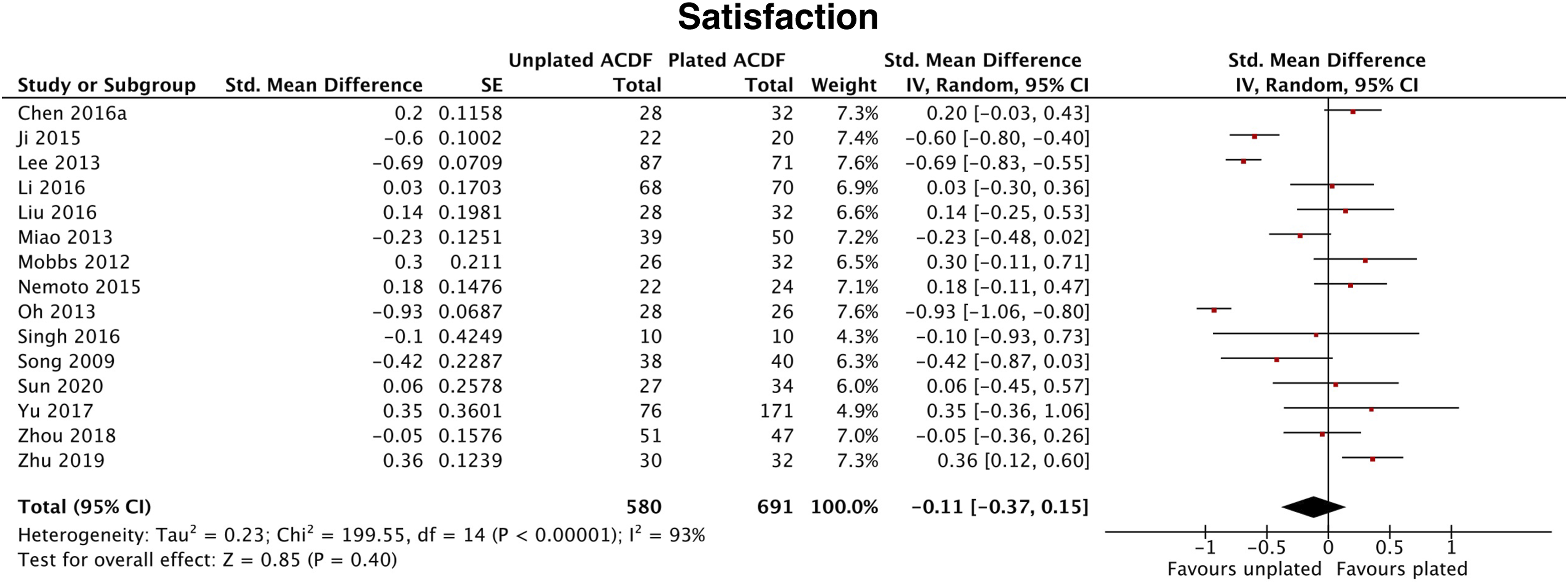
Discussion
The purpose of this review was to assess the role of osteobiologics in increasing spine fusion rate and affecting other key outcomes in patients undergoing unplated ACDF compared to subjects receiving anterior plating. According to the results of this study, no substantial differences in terms of fusion rate and PROs were reported between plated and unplated procedures, independently of the use of osteobiologics. However, patients receiving unplated ACDF demonstrated a significantly lower rate of post-operative dysphagia, despite often being transitory and solved at later follow-ups in both groups.
Although the use of a tricortical interbody AICBG with subsequent plating has historically been regarded as the gold standard in obtaining a solid fusion in ACDF, several alternatives have been proposed to overcome the frequent donor site morbidity as well as post-operative dysphagia, higher ASD and risk of hardware failure associated with the use of plates. 2 These are mainly represented by interbody cages that can be filled with a wide armamentarium of different materials with distinct osteoinductive, osteoconductive and osteogenic properties, as well as diverse costs, handling characteristics and availability on the market.62,63 Optimization of implant technology, surgical techniques and biological augmentation have demonstrated the possibility to achieve a solid fusion using stand-alone cages without the need for anterior plating, 64 although with increased rates of pseudarthrosis, cage subsidence and post-operative kyphosis. 65
Radiographic Outcomes
In accordance with previous studies,65-67 spine fusion was demonstrated in the majority of patients, with no statistically significant differences when comparing unplated vs. plated ACDF nor single- vs. multi-level procedures. However, solid fusion tended to be achieved later in unplated patients, even if not affecting fusion rate at the final follow up, except in a few studies reporting a higher 24 or lower 26 fusion rate in subjects treated with stand-alone cages. Similar fusion rates may be associated with comparable stability and range of motion characteristics of unplated and plated implants, as demonstrated by previous biomechanical evaluations.68-70 With regards to the relationship between fusion and different osteobiologics employed, it is difficult to draw scientifically sound conclusions due several reasons. First, a wide heterogeneity of osteobiologics has been used in included studies, with 10 different products mentioned and utilized alone or combined, with no information about quantity and quality in most instances. Furthermore, none of the studies specifically performed a subgroup analysis to investigate the putative adjuvant role of the osteobiologic adopted in promoting fusion in unplated procedures compared to plated surgeries. In addition, small sample sizes, lack of randomization, different number of operated levels as well as different cage material, design and volume of internal cavity further limited additional evaluations. Such aspects have been previously pointed out by the systematic reviews of Buser et al.71,72 which concluded that the absence of significant differences among the diverse osteobiologics in cervical spine fusion may be primarily due to the low evidence and high risk of bias characterizing clinical studies on the topic. Similar to fusion rate, no significant differences in terms of most radiological parameters were found among included studies. However, some studies reported a better preservation of cervical lordosis in patients treated with anterior plating, especially at later follow-ups, when progressive loss of lordosis may have occurred due to increased subsidence rate and lack of anterior support in unplated ACDF. 10 On the other hand, a few authors demonstrated that disc height tended to decrease faster in unplated patients, possibly as an expression of more frequent cage subsidence, which is in part prevented by adding anterior plating.51,52 According to our results, solid fusion was achieved independently of plating, although requiring additional time with the use of stand-alone cages, probably due to the less stable biomechanical environment. At this point, due to the insufficient evidence regarding the effect of osteobiologics, their role in augmenting bony fusion remains uncertain.
Perioperative Outcomes
Compared to plated ACDF, unplated procedures were associated with a shorter or similar operation time, with a few studies reporting longer operation time as a result of the learning curve required to perform the first cases in the cage-only cohort 27 and the difficulty to twist the screws of anchored cages due to unfavorable operative angle. 47
Furthermore, unplated ACDF also resulted in decreased or equal intraoperative blood loss, probably due to the lower extent of dissection and retraction to obtain a suitable exposure for plate positioning and reduced implant positioning time.25,33,34 Previous studies also showed that unplated ACDF was associated with a significantly lower intraoperative blood loss65,67 and a shorter operation time.65,67,73 Likewise, patients undergoing unplated ACDF showed a lower or similar LOS following surgery, which may be associated with the combination of reduced intraoperative blood loss and operation time as well as lower post-operative pain and complication rate. 34
Complications
Postoperative dysphagia is the most common complication following ACDF, resulting from a combination of soft tissue edema, hematoma, esophageal injury, and hardware adhesions. 74 Furthermore, severity of dysphagia has been directly correlated with plate thickness by Lee and colleagues. 50 Therefore, not surprisingly, dysphagia was significantly less common after unplated ACDF compared to plated procedures in the majority of included studies, although symptoms tended to be progressively relieved with time in the latter group. Dysphagia has also been reported in association with the use of BMP-2 in ACDF, independently of anterior plating. Indeed, previous studies have documented the release of several pro-inflammatory cytokines with consequent development of severe prevertebral swelling causing dysphagia and life-threatening dyspnea. 75 For this reason, the Food and Drug Administration has released an advisory on life-threatening complications associated with BMP-2 in cervical spine fusion, underlining that the use of such osteobiologic in cervical spine surgery is off-label. 76
Conversely, cage subsidence has most frequently been associated with the use of unplated cages in this study, as the lack of anterior fixation may slow down the fusion process and facilitate subsidence upon mechanical load. 77 This process has been correlated with the development of segmental kyphosis and hypermobility, with consequent cervical pain and disability. 41 As pointed out by previous studies, due to both different definitions of this phenomenon and doubtful clinical significance of asymptomatic radiographic subsidence, 77 further evaluations are needed to delineate its role. The incidence of ASD and ALOD was not significantly different between groups in most studies, however some reported an increased rate of ASD in association with anterior plating.27,28,31,33,34,36,51 Such a complication has been well known in the field, with an annual incidence of approximately 3% and a 10-year prevalence of 25% according to previous studies. However, radiographic evidence of degeneration does not automatically lead to clinical symptoms. Indeed, ASD may lead to reoperation in only 6-10% of cases. 78 The incidence of ASD and ALOD has been correlated with several factors, including length of fusion, proximity of the plate to adjacent intervertebral discs, higher rigidity of the construct with hypermobility of upper and lower levels adjacent to fusion levels, and extensive stripping of the anterior longitudinal ligament.28,79 Furthermore, ASD and ALOD are more frequent when fusion ends adjacent to C5–C6 and C6–C7, as such levels present with a greater range of motion and are thus more prone to degenerative changes. 80 On the contrary, unplated ACDF may result in lower ASD and ALOD rates mainly due to reduced rigidity and biomechanical stress to adjacent segments as a consequence of no plating. 81
Patient-reported outcomes
ACDF is usually associated with favorable outcomes in terms of pain, disability, satisfaction, and function irrespective of graft choice.11,82 However, some studies reported that patients undergoing unplated procedures lamented more pain compared to patients receiving anterior plating.8,35,41,50,55 This has been advocated by the progressive loss of lordosis due to cage subsidence and/or increased tension of the posterior cervical area due to pseudoarthrosis, both occurring more frequently with the use of stand-alone cages.
Limitations
There are several limitations to this study. First, the significant heterogeneity across studies in terms of design, number of operated levels, different type of implant, and osteobiologic used significantly limited solid conclusions to be made. Moreover, only 8 out of 38 studies were RCTs, and the majority of nonrandomized studies were retrospective, with an overall high risk of bias. Finally, the number of studies analyzed for each outcome varied consistently, which inevitably affected the amount of data available for each outcome measure.
Conclusions
In summary, available evidence suggests that both unplated and plated ACDF are associated with an improvement of patients’ pain, disability, and satisfaction, without significant intergroup differences. Unplated ACDF tended to be accompanied by lower blood loss, operation time and LOS, even if the small differences reported may have a doubtful clinical impact. In terms of radiographic outcomes, no significant difference regarding fusion rate and other parameters was noted, even if complete fusion was achieved earlier in plated patients. Due to the wide heterogeneity of osteobiologics used in included studies, their role on the achievement of solid fusion is still debated. With regards to complications, dysphagia was significantly more common following anterior plating but resolved over time, whereas cage subsidence was more frequent in unplated patients, although its role on sagittal balance and clinical outcomes is uncertain. Considering the very low overall quality of evidence of available studies as per the GRADE assessment, no solid conclusions can be drawn. Well-designed RCTs with rigorous description of employed treatment strategies are needed to evaluate the efficacy of osteobiologics in improving spinal fusion in unplated ACDF compared to plated ACDF.
Supplemental Material
Supplemental material - The Role of Osteobiologics in Augmenting Spine Fusion in Zero-Profile and Unplated Anterior Cervical Discectomy and Fusion Compared to Plated Constructs: A Systematic Review and Meta-analysis
Supplemental material for The Role of Osteobiologics in Augmenting Spine Fusion in Zero-Profile and Unplated Anterior Cervical Discectomy and Fusion Compared to Plated Constructs: A Systematic Review and Meta-analysis by Gianluca Vadalà, Luca Ambrosio, Sergio De Salvatore, Daniel K. Riew, S. Tim Yoon, Jeffrey C. Wang, Hans-org Meisel, Zorica Buser, and Vincenzo Denaro in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.