
Abstract
Switching from efavirenz (EFV) to dolutegravir (DTG) is increasingly common due to DTG's superior efficacy and tolerability, yet its metabolic impact in Southeast Asian populations remains unclear. We conducted a single-center retrospective cohort study (January 2019–December 2022) involving adults on EFV-based antiretroviral therapy for at least 6 months before transitioning to DTG. Weight, body mass index, lipid profiles, fasting blood glucose (FBG), renal function, and alanine transaminase (ALT) were measured at baseline, Month 6, and Month 12. Among 493 participants (mean age 47.6 years; 69% female), mean weight increased from 63.8 to 65.6 kg at Month 12 (P < .001). TC, low-density lipoprotein cholesterol (LDL-C), and triglycerides decreased, while high-density lipoprotein cholesterol (HDL-C) declined and FBG modestly improved. Estimated glomerular filtration rate (eGFR) dropped by 25% (P < .001). Higher baseline HDL-C was protective against significant weight gain (OR 0.11 per 10 mg/dL, P = .030). EFV-to-DTG switching leads to weight gain, mixed metabolic effects, and notable eGFR decline, supporting regular monitoring.
Introduction
The advancements in antiretroviral therapy (ART) have significantly improved overall outcomes, allowing individuals with human immunodeficiency virus (HIV) to live longer and maintain a quality of life similar to the general population. Despite these strides, people living with HIV (PLWH) face an elevated risk of cardiovascular diseases, which includes hypertension, coronary artery disease, stroke, and vascular complications, compared to those who are not PLWH.1-3 This heightened risk is attributed to chronic inflammation directly resulted from HIV infection itself, long-standing immune activation, adverse effects of ART, and other well-known risk factors such as smoking, obesity, and sedentary lifestyles.4,5 Thus, an effective HIV management must go beyond sustained viral suppression, emphasizing the importance of reducing cardiovascular risk to safeguard patients’ long-term health.
According to Thailand National Guidelines on HIV/AIDS treatment and prevention 2021/2022, the recommended first-line regimen is comprised of 2 nucleotide reverse transcriptase inhibitors and one integrase strand transfer inhibitor (INSTI) as in a single tablet formula. 6 Dolutegravir (DTG) is the INSTI available in Thailand since August 2013 and has been registered in Thailand National List of Essential Medicines since October 2021. The use of DTG as a first-line regimen is due to its excellent efficacy to suppress the virus and less incidence of drug-resistance.7,8 With the inclination usage of DTG as the drug of choice, recent studies have found that PLWH who switched ART to DTG-based regimen experience significant weight gain (SWG).9-11 Previous studies, NAMSAL and ADVANCE, conducted in Cameroon and South Africa respectively, have demonstrated an SWG of at least 10%.12,13 Due to growing concerns about the metabolic effects of DTG, studies have also been conducted to investigate lipid changes after switching regimen. Data showed safer lipid profiles for DTG in combination ART and provide a treatment option for patients who may have other risk factors for metabolic syndrome. 14
Although African cohort studies have reported substantial weight gain after DTG initiation, population-level differences in ethnicity, genetics, diet, and body composition may influence metabolic responses in Southeast Asian populations. For instance, differences in CYP2B6 polymorphisms (more common in African populations) affecting efavirenz (EFV) metabolism, variation in UGT1A1 differs across populations (the UGT1A16 variant, which is frequently found in Asian populations, whereas UGT1A128 predominates in African American populations), or average baseline body mass index (BMI) may influence postswitch outcomes. Accordingly, this study aims to characterize these effects within a Thai cohort.15,16
Another potential metabolic side effects associated with DTG is its impact on blood glucose levels. While former generations of ART, such as protease inhibitors, were frequently linked to insulin resistance and incidence of hyperglycemia, novel agents like DTG have been considered less likely to cause significant glycemic disturbances. 17 Nonetheless, emerging studies have suggested that DTG may still have an effect on glucose metabolism, potentially contributing to changes in blood sugar levels in some individuals. 18
However, there have been scarce studies exploring the impact of DTG on weight change and metabolic consequences after switching ART-regimen among the Thai population. Moreover, there was a major change in the 2022 Thailand policy, resulting in the National Health Security Office discontinued the procurement of the previous EFV-based medication replacing it with a DTG-based drug. Consequently, healthcare providers were required to switch medications for patients covered under the universal health coverage program, in line with government policy. Thus, this study intents to examine weight change, lipid profiles, fasting blood glucose (FBG), renal function, and liver enzyme as well as factors contributing to weight gain.
Methods
A retrospective single-center, closed-cohort study was conducted at Ramathibodi Hospital (a 1200-bed tertiary care hospital, Bangkok, Thailand). This study was approved by The Human Research Ethics Committee of the Faculty of Medicine Ramathibodi Hospital, Mahidol University. This study adhered to the ethical principles of the Declaration of Helsinki and Good Clinical Practice guidelines. Given the retrospective design of the study and the use of previously collected, deidentified data, the requirement for informed consent was waived by the ethics committee. Inclusion criteria required PLWH, identified based on ICD-10 diagnostic codes in the Electronic Medical Records, with an age of 18 years or older, to have received EFV-based regimen for at least 6 months before switching to DTG-based regimen, to comply with the government policy, and were in the cohort during January 2019 through December 2022. According to the Thai National Guidelines, virological suppression should be documented within 1 year before switching. The crude data regarding the virological level was not collected. To minimize confounding variables, we ascertained that all patients were on the same regimen, which is tenofovir disoproxil fumarate (TDF), emtricitabine plus EFV, before switching and prescribed the same new regimen, which is TDF, lamivudine (3TC) plus DTG. Exclusion criteria included presence of drug resistance mutations at baseline, medication nonadherence (defined as adherence less than 95%), pregnancy, severe illnesses (defined as serious and life-threatening medical conditions that require urgent or intensive in-hospital care) such as active opportunistic infections, malignancy, or conditions requiring systemic immunomodulators that could potentially affect body weight within 6 months prior to switch, or incomplete or missing data.
Baseline characteristics were collected from electronic medical records and included demographic, clinical, and laboratory data. The laboratory data were distinctly obtained under fasting conditions to ensure interpretability. Changes in body weight and BMI, FBG, lipid profiles including total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglyceride (TG), renal function (creatinine or Cr, estimated glomerular filtration rate or eGFR), and liver enzyme (alanine transaminase [ALT]) were assessed at Month 6 and Month 12 postswitch. It merited consideration that this was a retrospective designed study, thus the assessments for each scheduled visit (Month 6 and Month 12) were obtained within predefined time windows (eg, ±30 days).
The primary outcome of this study was the change in body weight (kg) at Month 12 after switching from an EFV-based regimen to a DTG-based regimen. A multilevel mixed-effects linear regression model was used to analyze repeated measures of body weight at baseline, Month 6, and Month 12. This model was specified with random intercepts for each participant (random intercept only) to account for within-subject correlation over time which was modeled as a categorical variable (no random slopes were included). Baseline body weight was included as the measurement at time 0 in this model. Changes in BMI were analyzed similarly. Secondary outcomes included changes in FBG, lipid profiles (TC, HDL-C, LDL-C, and TG), renal function, and liver enzyme, and the results were analyzed in a similar manner. Data were reported as the means (standard deviation, SD) for continuous variables with normal distribution, the median (interquartile range, IQR) for continuous variables without normal distribution, and the percentage for categorical variables.
SWG was defined as a weight increase of at least 5% from baseline to 12 months. 19 Not only SWG has an impact on esthetic concerns but also contributes to health issues as well. Recent evidence substantiated chronic inflammation as one of the major risk factors for cardio-metabolic diseases, and overweight appeared to be the key factor of increased systemic inflammation. 20 A univariate logistic regression analysis was initially performed to identify potential predictors of SWG. Variables with P < .1 in univariate analysis were included in a subsequent multivariate logistic regression. In addition, sex and baseline BMI (were included in the multivariate model based on clinical relevance, regardless of univariate significance. Adjusted odds ratios (OR) and 95% confidence intervals (CI) were calculated for each factor. All tests were 2-sided, and a P-value < .05 was considered statistically significant. Statistical analyses were conducted using STATA version 18 (StataCorp, College Station, Texas, USA). Given that 137 participants experienced SWG, the final multivariable model included 6 predictors, yielding approximately 23 events per variable; this ratio suggested a minimal risk of overfitting.
Results
A total of 493 PLWH were included in the study as shown in Figure 1. The mean age (SD) was 47.6 (11.8) years, with 69.8% of the cohort being female. Most patients had a CD4 count ≥200 cells/mm3 (90.7%) with a median CD4 count (IQR) of 528 cells/mm3 (376-693). Of all, 11.6% had a history of opportunistic infection. Comorbidities were present in 62.1% of patients, with dyslipidemia and hypertension being the most common conditions (Table 1).

People living with HIV enrollment and study flow chart.
Baseline Characteristics of 493 People Living With HIV Who Had Switched From Efavirenz-Based Regimen to Dolutegravir-Based Regimen.

Abbreviations: IQR, interquartile range; SD, standard deviation.
Switching from EFV- to DTG-based therapy resulted in statically significant increase in body weight and BMI (Table 2 and Figure 2). The mean (SD) baseline body weight was 63.8 (13.5) kg, which increased to 65.1 (13.8) kg at Month 6 and 65.6 (13.8) kg at Month 12. These changes represented a 1.9% increase at Month 6 and a 2.7% increase at Month 12, both of which were statistically significant (P < .001). Similarly, BMI showed a corresponding increase, rising from a baseline value of 23.3 (4.0) kg/m2 to 23.7 (4.1) kg/m2 at Month 6 and 23.9 (4.2) kg/m2 at Month 12 (P < .001).

Mean change in body weight and body mass index.
Mean Change in Body Weight and Body Mass index.
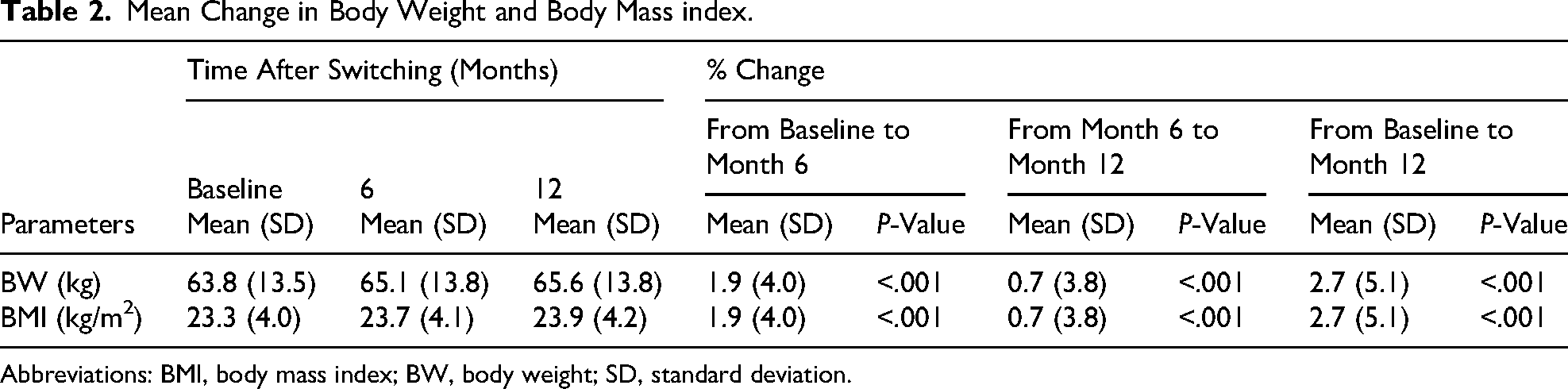
Abbreviations: BMI, body mass index; BW, body weight; SD, standard deviation.
Significant improvements were observed in lipid profiles after switching to the DTG-based regimen. TC levels decreased from 196.2 (42.5) mg/dL at baseline to 179.3 (39.6) mg/dL at Month 6 and 179.4 (38.8) mg/dL at Month 12, corresponding to a reduction of 12.1% and 13.4%, respectively (P < .001). HDL-C levels decreased from 49.1 (14.5) mg/dL at baseline to 44.9 (11.9) mg/dL at Month 6 and 45.2 (12.1) mg/dL at Month 12, reflecting a decline of 11.3% at Month 6 and 9.9% at Month 12 (P < .001). LDL-C levels improved, declining from 124.7 (33.4) mg/dL at baseline to 115.2 (33.1) mg/dL at Month 6 and 117.2 (37.7) mg/dL at Month 12 (P < .001). TG levels, nonnormal distribution, also showed significant reductions, with the median level decreasing from 117 mg/dL (IQR: 83-174) at baseline to 99 mg/dL at Month 6 and 100.5 mg/dL at Month 12 (P < .001).
FBG showed modest but significant reductions over the study period. The mean baseline FBG was 99.4 (16.3) mg/dL, which decreased to 98.4 (20.3) mg/dL at Month 6 and 97.3 (19.8) mg/dL at Month 12. While the reduction at Month 6 did not reach statistical significance (P = .052), the decrease observed at Month 12 was statistically significant (P = .001). However, renal function showed notable changes during the study. Serum creatinine increased from 0.9 (0.3) mg/dL at baseline to 1.1 (0.5) mg/dL at Month 6 and remained at 1.1 (0.3) mg/dL at Month 12 (P < .001). In contrast, the eGFR decreased significantly, from 95.0 (20.0) mL/min/1.73 m2 at baseline to 80.3 (20.9) mL/min/1.73 m2 at Month 6 and 77.0 (19.9) mL/min/1.73 m2 at Month 12, representing a 25% decline from baseline to Month 12 (P < .001). The observed decline in eGFR is consistent with DTG's known inhibition of renal creatinine secretion via organic cation transporter 2 (OCT2) and multidrug and toxin extrusion protein 1 (MATE1) transporters, which may overestimate true GFR reduction. The magnitude of eGFR reduction observed is greater than that typically described in non-Asian cohorts and may be attributable to both transporter-mediated increases in serum creatinine and possible underlying renal effects, especially in populations with a high burden of comorbidities. ALT levels also showed significant declines during the study period. The median baseline was 36 mg/dL (IQR 26-52.5), which decreased to 33 mg/dL (IQR 24-48) at Month 6 and 32 mg/dL (IQR 23-47) at Month 12 (P = .001) (Figures 3 and 4).

Mean and median change in lipid profiles, fasting blood glucose, and liver enzyme. Abbreviations: ALT, alanine transaminase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol; TG, triglyceride.

Mean change in renal function.
At Month 12, 137 out of 493 patients (27.8%) met the criteria for SWG (≥ 5% weight increase from baseline). Univariate analysis of SWG is shown in Table 3. Presence of chronic kidney disease and lower baseline HDL-C level showed significant associations with SWG in univariate analysis. In the multivariate analysis (which included sex and baseline BMI as covariates), only a higher baseline HDL-C level remained a significant protective factor against SWG. For every 10 mg/dL increase in baseline HDL-C, the odds of SWG decreased by 89% (OR 0.11, 95% CI [0.02-0.80], P = .030). Other factors, including sex and baseline BMI, were not significantly associated with SWG after adjustment (Table 4).
Mean and Median Change in Lipid Profiles, Fasting Blood Glucose, Renal Function, and Liver Enzyme.

Abbreviations: ALT, alanine transaminase; Cr, creatinine; eGFR, estimated glmerular filtration rate; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SD, standard deviation; TC, total cholesterol; TG, triglycerides.
Factors Associated With Significant Weight Gain by Univariate Analysis.

Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; Cr, creatinine; eGFR, estimated glomerular filtration rate; ALT, alanine transaminase.
Discussion
The result from this study provides insightful information regarding the weight gain and metabolic effects of switching from an EFV- to a DTG-based regimen in Thai PLHW. The findings highlight significant increases in body weight and BMI. On the other hand, laboratory results showed a notable decrease in lipid profiles, FBG, and ALT levels over a 12-month period postswitch. While the declination in metabolic parameters showed a promising result, eGFR also significantly decreased over a period of study, which might reflect a reduction in renal function despite the direct inhibitory effect of the drug.
The observed increases in body weight and BMI align with previous studies conducted in other populations, ADVANCE trial in South Africa and the NAMSAL trial in Cameroon, further confirming the metabolic impacts of DTG in diverse ethnic groups. These studies highlighted the fact that women and individuals with lower baseline body weight experienced the greatest weight gain. 21 Similarly, in our study, a higher proportion of participants were female with 69.8% of the cohort, which may partly explain the observed weight changes. However, the multivariate did not show significant associations between the sex and the impact on weight change, which might be the result of a relatively small cohort size. The mechanism underlying weight gain with DTG remains unclear but may involve a reduction in weight-suppressive effects of EFV. 22
Our study demonstrated significant improvements in lipid profiles, including reductions in TC of 13.4%, LDL-C of 25.5%, and TG of 31.5%. These findings are consistent with both the ADVANCE and NAMSAL trials.12,13 Unexpectedly, HDL-C levels decreased by approximately 10% in our study which contrasts with findings from previous study in Uganda. 23 Lower HDL-C levels may counterbalance the lipid benefits of DTG. The observed 10% reduction in HDL-C may attenuate the cardiovascular benefit of improvements in LDL-C and TG. This finding contrasts with some prior studies and warrants further investigation into whether it reflects a unique metabolic response in Thai individuals or is related to other factors like dietary basis. In contrast to findings from Kigongo et al in a Ugandan cohort, where HDL-C remained unchanged following DTG initiation, a significant decrease was observed in our study, potentially reflecting ethnic differences in DTG-associated lipid metabolism or baseline cardiovascular risk profiles. This accentuates the importance of holistic cardiovascular risk assessment beyond lipid profiles alone. 24 Furthermore, a multivariate analysis in our study established higher baseline HDL-C levels as a protective factor against SWG, with a 10 mg/dL increase in HDL-C reducing the odds of SWG by 89%. This finding complements observations from the ADVANCE trial, which noted that patients with higher HDL-C levels may have the baseline of healthier lifestyle habits, thus making them less likely to experience excessive weight gain.
FBG showed a modest but significant reduction in our study, consistent with the ADVANCE trial, which found no evidence of worsening glycemic control with DTG. Although statistically significant, the mean FBG reduction of 2.1 mg/dL is of uncertain clinical relevance, meaning it may not translate into reduced diabetes risk. Unfortunately, HbA1c data were unavailable to confirm glycemic trends. Nevertheless, no patients developed new-onset diabetes during follow-up. However, there is a case series from Ethiopia reporting the emergence of newly diagnosed type 2 diabetes in PLWH after switching to a DTG-based ART regimen within 10 months postswitch. 25 Additionally, hyperglycemia was also reported in several DTG trial studies such as SPRING-2, SINGLE, and VIKING-3.26-28 However, our study differs from these trials, as our study design involves “switching” ART regimen, whereas the mentioned trials involve initiating a new medication in new and ART-naïve cases. This may result in varied outcomes and adverse effects. The proposed mechanism of DTG-induced hyperglycemia is still controversial, but some suggested it may involve glucose transport alterations and increase hepatic gluconeogenesis via a decrease in magnesium levels.29,30 This suggests that DTG may have a neutral effect on glycemic parameters in Thai populations compared to EFV, which is known for its association with hyperglycemia in some patients.
Renal function, however, showed a notable decline in our study, with a 25% reduction in eGFR over 12 months. It is already known that DTG increases serum creatinine on an average of 10% to 15% due to the inhibition of renal transporters OCT2 and MATE1 and multidrug and toxin extrusion transporter 2-K (MATE2-K).31-34 This observed results aligns with findings from the ADVANCE and VIKING trials.13,35 However, the magnitude of decline in our study was more pronounced, potentially reflecting differences in baseline renal function or comorbidities among Thai PLWH. With a mean of 0.2 mg/dL increase in creatinine at Month 12 in Thai population, regular renal monitoring remains critical, especially for patients with preexisting renal conditions or those at risk of nephrotoxicity. Thorough investigations into renal dysfunction may be most applicable for patients experiencing early creatinine rising of ≥0.3 mg/dL. 36
The observed reduction in ALT from this study may suggest improved liver enzyme or reduced hepatic injury following the switch from EFV to a DTG-based regimen. DTG is associated with a better hepatic safety profile compared to EFV, which is known for its potential hepatotoxic effects. 37 Furthermore, factors like better viral suppression and lower inflammatory responses are observed in DTG more than EFV, which might have contributed to the improvement of liver enzyme levels. 38
Our study design does not permit distinction between effects of DTG initiation and EFV discontinuation. EFV is known to suppress weight and elevate lipids; thus, observed improvements in lipid profiles and weight gain may partly reflect removal of EFV's adverse effects. In other words, EFV has been associated with hyperlipidemia and weight suppression; accordingly, the observed lipid improvements and weight gain following regimen switch may, in part, represent reversal of EFV-related metabolic disturbances.
The study's strengths included its uniformity in ART regimens and inclusion of a well-defined Thai cohort, which fills a gap in the literature on metabolic changes in Southeast Asian PLWH. This study also represents the first moderate-scale investigation into the metabolic effects within Asian populations, highlighting the unrecognized differences that exist among various ethnic groups. The baseline characteristics are self-controlled which minimizes the confounding variables. However, the study's retrospective design and single-center setting limit its generalizability, and the sample size is relatively small. Additionally, the absence of a control group on continued EFV limits the ability to provide more robust evidence for the causal relationship between DTG and observed metabolic changes.
Conclusions
The transition from EFV- to DTG-based antiretroviral regimens resulted in noticeable weight gain and improvements in lipid profiles, including reductions in TC, LDL-C, and TG. However, a decline in HDL-C levels and renal function was also observed, which may have implications for cardiovascular aspects. Higher baseline HDL-C levels were identified as a protective factor against SWG, highlighting the role of baseline metabolic health in influencing outcomes. To optimize care for PLWH, routine monitoring of metabolic parameters and personalized interventions should be integrated into clinical practice when switching to DTG-based therapy. We recommended baseline and 6-month postswitch evaluation of body weight, lipid profile, renal function (serum creatinine and eGFR), and FBG in patients switching to DTG, with tailored counseling for individuals with preexisting obesity, dyslipidemia, or renal dysfunction.
Footnotes
Acknowledgements
Not applicable.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The research protocol was reviewed and approved by the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University (Approval No. MURA2024/76). Individual informed consent was waived due to the retrospective nature of the study, and no identifiable personal data were included.
Consent for Publication
Not applicable.
Authors’ Contributions
PC and SK made substantial contributions to the conception of the study. SK contributed to the design of the work. PC and SK interpreted the data. PC and SK drafted the manuscript. All authors approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.