
Abstract
Introduction
: Dolutegravir (DTG)-based antiretroviral therapy (ART) use has been associated with excessive weight gain, increasing the risk of dyslipidemias such as hypercholesterolemia. We assessed the prevalence of, and associated factors with dyslipidemia among adults on DTG-based ART.
Materials and methods
We conducted a cross-sectional study among 281 systematically sampled adults on DTG-based ART for ≥ 6 months at Kira Health Centre IV, Wakiso District, Central Uganda. Data were collected through structured questionnaires, medical record reviews, anthropometric measurements, and laboratory biomarker analysis. Logistic regression was used to determine associated factors, and the predictive performance of obesity indices was evaluated using receiver operating characteristic (ROC) curve analysis.
Results
The prevalence of dyslipidemia was 44.1% 95% CI: 38.4%–50.0%. Low high-density lipoprotein (HDL) cholesterol was the most common abnormality, affecting 39.9% of participants, followed by elevated total cholesterol at 5.7% [95% CI: 3.51–9.11] and elevated low-density lipoprotein (LDL) cholesterol at 5.0%. High waist circumference (WC) was significantly associated with dyslipidemia; (aPR: 1.93, 95% CI: 1.15–3.24, p = .013), and demonstrated a significant ability to predict dyslipidemia with area under the curve (AUC) of 0.577 [95% CI: 0.511–0.644]. The AUC for WC in predicting hypercholesterolemia, elevated LDL-C, and low HDL-C were 0.702 (95% CI: 0.547–0.857), 0.729(95% CI: 0.590–0.867), and 0.548 (95% CI: 0.481–0.616) respectively.
Conclusion
Dyslipidemia is prevalent among adults on DTG-based ART, and is potentially associated with high WC.
Introduction
Worldwide, there were an estimated 38 million HIV-positive individuals in 2021, and 680,000 (1.79%) of them died from AIDS-related causes. 1 Sub-Saharan Africa continues to be the most impacted region, home to more than two-thirds of all people living with HIV (PLHIV) worldwide. 2 With over 55% of all PLHIV occurring in Eastern and Southern Africa, this region has the largest burden. 2 About 1.3 million adults ( ≥ 15 years old) in Uganda were estimated to have HIV in 2020, accounting for more than 90% of the country's total HIV prevalence. 3 Furthermore, in Uganda, HIV-related deaths ranked as the third most common cause of death in 2019. 4 Antiretroviral therapy (ART) has, however, been widely implemented, which has greatly decreased death rates and increased the life expectancy of PLHIV. ART expansion is particularly important in reducing adult mortality. 5
Dolutegravir (DTG) is the recommended first-line and second-line ART regimen for PLHIV, including pregnant women and those of reproductive age, according to the World Health Organization (WHO). Evidence supporting DTG's greater effectiveness, simplicity of use, and decreased frequency of adverse effects in comparison to alternative ART alternatives supports this suggestion. 6 Uganda's Ministry of Health (MoH) implemented DTG in conjunction with tenofovir (TDF) and lamivudine (3TC) as the recommended first-line treatment for adults with HIV in accordance with these guidelines. 7
Notwithstanding its advantages, the use of DTG-based ART is linked to a number of metabolic issues, such as dyslipidemia.8–10 Older ART regimens, like those that contain DTG, have been linked in studies to decreased levels of HDL and increased levels of total cholesterol (TC). 11 Furthermore, compared to non-nucleoside reverse transcriptase inhibitors (NNRTIs) like efavirenz, current data indicates that DTG and other integrase strand transfer inhibitors (INSTIs) may be more likely to cause dyslipidemia. 12 Furthermore, PLHIV on DTG-based regimens have shown considerable increases in TC and LDL levels, according to clinical trials carried out in African populations.13,14 According to a study conducted in North Ethiopia, the prevalence of dyslipidemia was 75% (48/64) in the group receiving efavirenz-based ART and 79.7% (51/64) in the group receiving DTG-based ART. 15
In Uganda, studies have mostly examined diabetic mellitus (DM) and hyperglycemia in PLHIV receiving DTG-based ART,16,17 with little attention paid to dyslipidemia. An important risk factor for non-communicable diseases such as diabetes, cardiovascular disease, and hypertension is poorly controlled dyslipidemia. 18 However, lipid profile screening is not routinely performed among PLHIV in Uganda, inclusive of Kira Health Centre IV, Wakiso District, Uganda due to limited data availability and financial constraints. Yet, data from the HMIS of Kira for the months of November and December showed 12/30 patients with dyslipidemia of those whose lipid profiles were assessed. The current national guidelines for monitoring PLHIV on DTG-based regimens emphasize glycemic assessment but lack recommendations for routine lipid profile screening. 19 Given the uncertainty surrounding the prevalence and risk factors of dyslipidemia in PLHIV on DTG-based therapy, this study aimed to determine the prevalence and associated factors of dyslipidemia among adults receiving DTG-based ART at Kira Health Centre IV, Wakiso District, Uganda.
Methods
Study Design, Population and Sampling Technique
Between September 2024 and December 2024, a descriptive and analytical cross-sectional study was carried out among adult HIV patients undergoing DTG-based ART. The study was conducted at Kira Health Centre IV, a government healthcare facility located on Mbogo Road in Kira Town Council, Kyadondo, Central Uganda. This health center serves a population of over half a million people from Kira Municipality and surrounding areas, providing comprehensive healthcare and specialized HIV services. The HIV clinic at Kira Health Centre IV offers services such as HIV testing and counseling, Prevention of Mother-to-Child Transmission (PMTCT/EMTCT), Safe Male Circumcision (SMC), ARTART and monitoring, health talk programs, and psychosocial support. The facility has approximately 1600 active PLHIV attending the ART clinic, with the majority coming from Kira and Namugongo Divisions. Over 90% of these patients are on DTG-containing regimens, making the site well-suited for this study.
Male and female patients aged 18 years and above who had been on DTG-based ART for at least six months were included in this study upon providing informed written consent. Patients with missing medical records, those who were bedridden, those with a history of using lipid-lowering therapy, and individuals unable to speak were excluded from the study. A systematic sampling technique was used to recruit study participants, ensuring a representative selection from the ART clinic's patient population.
Sample Size Determination
The Keish Leslie formula of 1965 was used to determine the minimum required sample size using the following assumptions; 19.3% proportion of adult HIV patients on DTG-based ART with hypercholesterolemia at Mengo Hospital in Kampala, Uganda,
10
5% precision and a 95% confidence interval and the Z-statistic of 1.96.


By considering a 10% nonresponse rate, the minimum sample size for this study was 263 participants
Therefore, the minimum sample size of 263 study participants was considered for this study.
Study Variables
Dyslipidemia was the primary outcome variable. The independent variables were categorized as social-demographic factors, behavioral factors, clinical factors, and HIV and/or ART-related factors. The social-demographic factors included age, sex, and education level, religion, employed status, marital status. The behavioral factors included smoking status, alcohol consumption, sleep duration, sleep quality, and physical activity. Clinical factors included hypertension, family history of hypertension, Diabetes Mellitus, family history of Diabetes Mellitus, family history of hypertension, overweight, Obstructive sleep apnea, obesity, WC, waist to height ratio, and waist to hip ratio. HIV and/or ART-related factors included duration with HIV-infection, duration on DTG-based ART, and viral load.
Data Collection Tools, Procedures and Operational Definitions
A structured Questionnaire was used to collect data on the social-demographic factors, behavioral, clinical factors and HIV and/or ART-related factors. Medical records were also reviewed to collect data regarding duration with HIV infection, most recent viral load result, and duration on DTG-based ART. The most recent viral load result in the participant's file was considered and categorized as < 200 and ≥ 200copies/mL. Physical activity was assessed using the International Physical Activity Questionnaires (IPAQ) 20 and categorized as < 600 (Low), 600–3000 (Moderate), and > 3000 (High) MET-minutes/Week. Obstructive sleep apnea was assessed using Stop Bang scoring model and classified as High risk and low risk. 21 Additionally, a professional nurse working under the lead investigators’ supervision took blood pressure (BP) and anthropometric measurements (weight, height, WC, and hip circumference (HC)) from the study participants. Blood pressure was measured using a digital sphygmomanometer. The blood pressure for this study was determined by taking the mean of two blood pressure readings that were collected five minutes apart. Systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg were considered high blood pressure. 22 A portable weight and height scale was used to measure the participant's height and weight. Based on height and weight, body mass index (Kg/m2) was determined and classified as < 25, 25–29.9, and > 30. 23 The waist and hip circumferences were measured using a non-stretchable Seca Ergonomic Circumference Measuring Tape. A third measurement was only made if the discrepancy between the first two circumference values was more than three centimeters. The mean of two or three measurements was used to calculate the waist and hip circumferences. For women, a high WC was defined as greater than 80 cm, and for men, greater than 94 cm.. 24 Waist and hip circumferences were used to compute the waist to hip ratio, which was deemed excessive if it was ≥ 0.85 for women and ≥ 0.9 for men. 25 Consuming fewer than five servings of fruits and vegetables per day was considered low fruit and vegetable intake. 26
Lastly, the principal investigators used Yellow (SST) vacutainer vacuum vials to obtain approximately 4 ml of venous blood samples from each study participant. Within an hour of the blood being drawn, the serum was separated and kept in a freezer at −20 °C. The samples were properly wrapped in dry ice at the conclusion of the week and sent to the Jinja Regional Referral Hospital Laboratory Co., a government SANAS-accredited laboratory with Accreditation Number: M0730, for testing. Their registration number is AHPC 16/10131G. The Roche Cobas c311 clinical chemistry analyzer (provided and maintained by national vendor Medisell) was used to measure the concentrations of serum total cholesterol, LDL-C, HDL-C, and triglycerides. In addition to performing up to 800 tests per hour, the analyzer also automatically handles all reagent and sample pipetting, incubation, photometric measurements, and calculations, reducing the error rate. The Roche c311 chemistry analyzer was calibrated using Cfas and cfas Lipids, and both normal and pathological quality control samples, such as PCC1 and PCC2, were run on the analyzer each time before research samples were run. SOPs of the laboratory and the manufacturer's instructions for running QCs and samples on this machine were closely adhered to.
According to the National Cholesterol Education Program Adult Treatment Panel III guideline, dyslipidemia is defined as LDL-C ≥ 130 mg/dL, TC ≥ 200 mg/dL, TG ≥ 150 mg/dL, and HDL-C < 40 mg/dL for men and < 50 mg/dL for women, occurring alone or in combination. Since we employed a random sample to determine the lipid profile and triglycerides are impacted by a non-fasting condition, serum triglycerides were not taken into account as a parameter in our study's definition of dyslipidemia.
Statistical Analysis
After being double-entries into Microsoft Excel, the gathered data was exported to STATA version 17 software for analysis. Using the Shapiro–Wilk normality test, the continuous variables (WC, body mass index, and waist to hip ratio) were examined for normality; they were not (p ≤ .05) normally distributed. These were summarized using the median (interquartile range: IQR) and a non parametric test; the Mann–Whitney U test was used to compare the medians of individuals with and without the outcome variable (dyslipidemia) in order to determine whether there were any statistical differences between the two groups. P values less than .05 were regarded as statistically significant. Both proportions (percentages) and frequencies were used to summarize categorical variables.
By dividing the number of participants with dyslipidemia by the total number of research participants recruited, the proportion of study participants with dyslipidemia and its 95% CIs were calculated. The percentage was then displayed graphically using a pie chart. A Chi square test or Fischer's exact test was used to assess the prevalence of dyslipidemia across the various levels of each categorical independent variable. P values less than .05 will be regarded as statistically significant.
The studied factors were assessed using modified Poisson regression since the prevalence of dyslipidemia was more than 10%. 27 Dyslipidemia was binary dependent variable (0 = absent, 1 = present). All independent variables, at bivariate level, were compared with the dependent variable. The prevalence ratios and their 95% CI were used to measure the associations, and a P value ≤.2 at the bivariate level indicated statistically significant prevalence ratios. The multivariable model evaluated the factors that were statistically and/or clinically significant at this level. By removing some of the variables from the multivariate model, precision, accuracy, and collinearity were taken into account in the multivariate analysis without significantly compromising the model's validity. P-values ≤ .05 were deemed significant for relationships in the final multivariable model.
The significant associated factors were evaluated for their predictive performance in the discrimination of study participants between those with and those without dyslipidemia using Receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) was a measure of the predictive performance and the AUC whose 95%confidence interval does not include the null value of 0.5 was considered a significant predictor.
Results
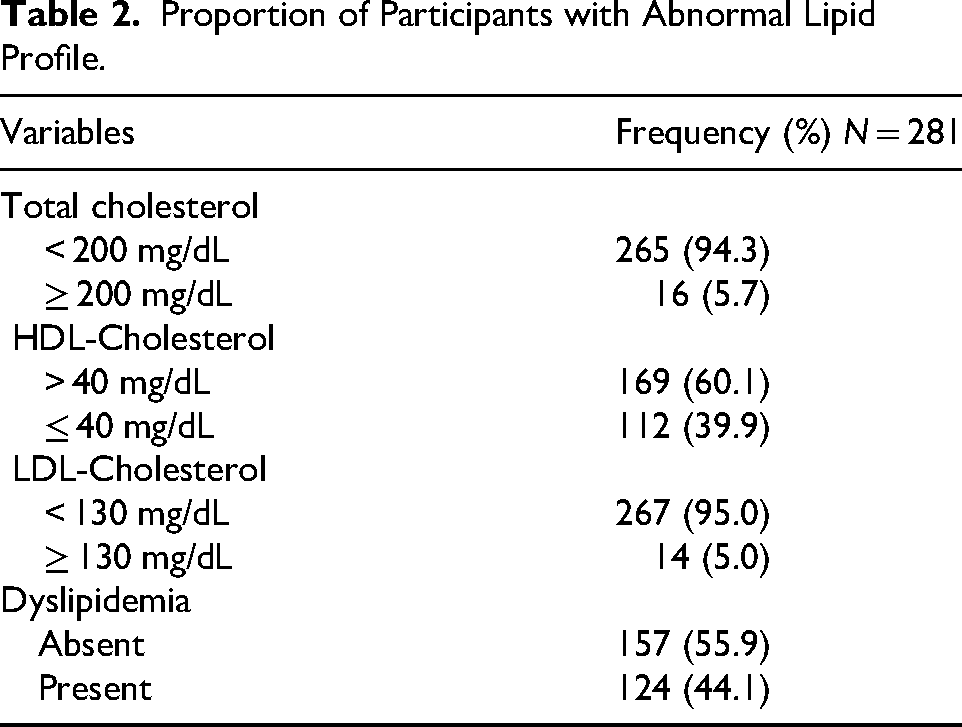
Out of 281 study participants, 124 had dyslipidemia, giving an overall prevalence of 44.1% (124/281) 95% CI: 38.4% - 50.0% (Figure 1), indicating a considerable burden of lipid abnormalities among PLHIV on DTG-based ART in Central Uganda. Total cholesterol levels were elevated (≥ 200 mg/dL) in 5.7% of participants, while the majority (94.3%) had total cholesterol levels within the normal range ( < 200 mg/dL). High-density lipoprotein cholesterol (HDL-C) was reduced ( ≤ 40 mg/dL) in 39.9% of participants, highlighting a significant proportion at risk for cardiovascular complications due to low protective lipoprotein levels. In contrast, low-density lipoprotein cholesterol (LDL-C) was elevated (≥ 130 mg/dL) in only 5.0% of participants, suggesting a relatively low prevalence of high atherogenic lipoprotein levels in this cohort (Table 2).
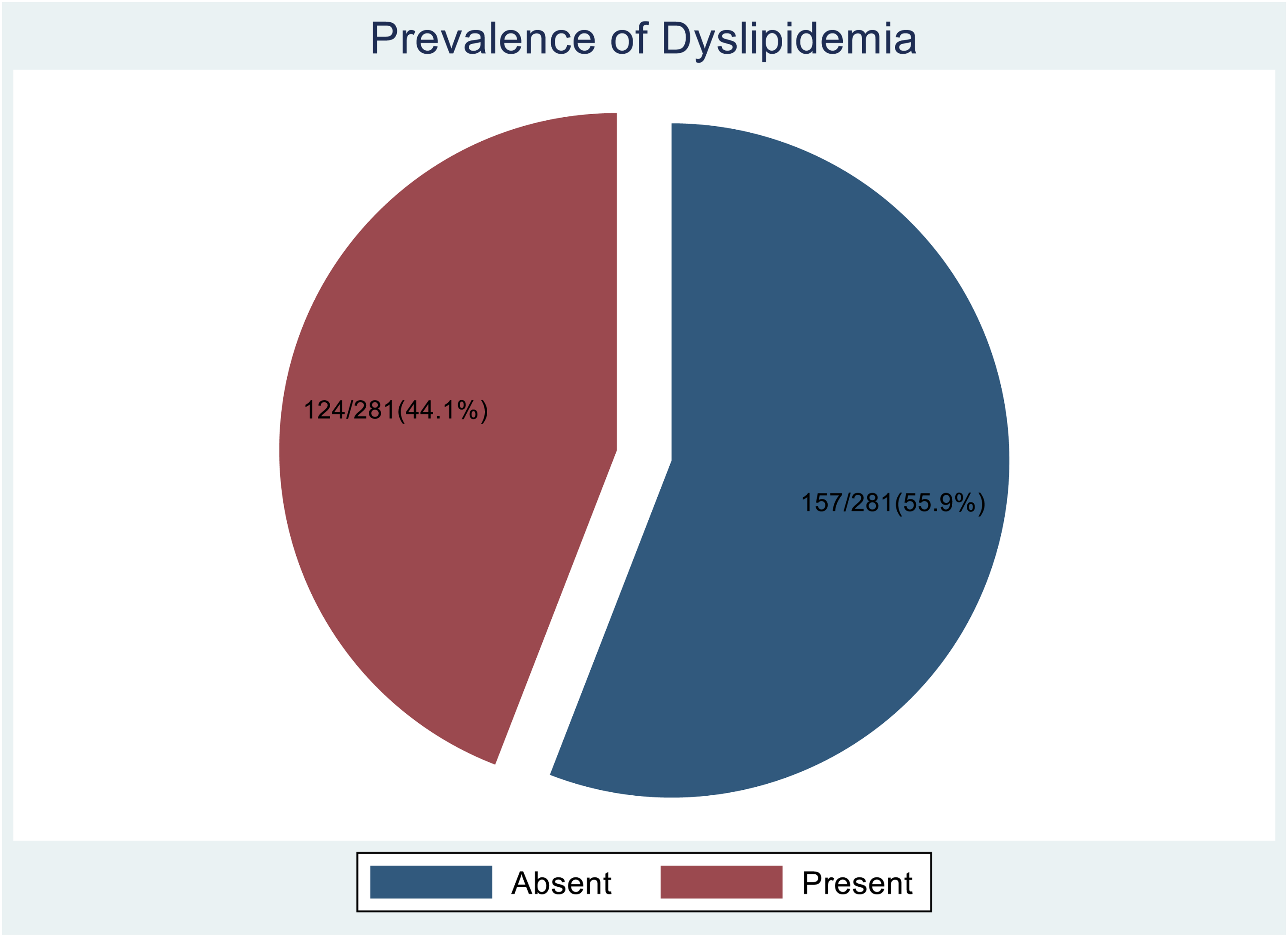
A Pie Chart Showing Proportion of Study Participants with Dyslipidemia.
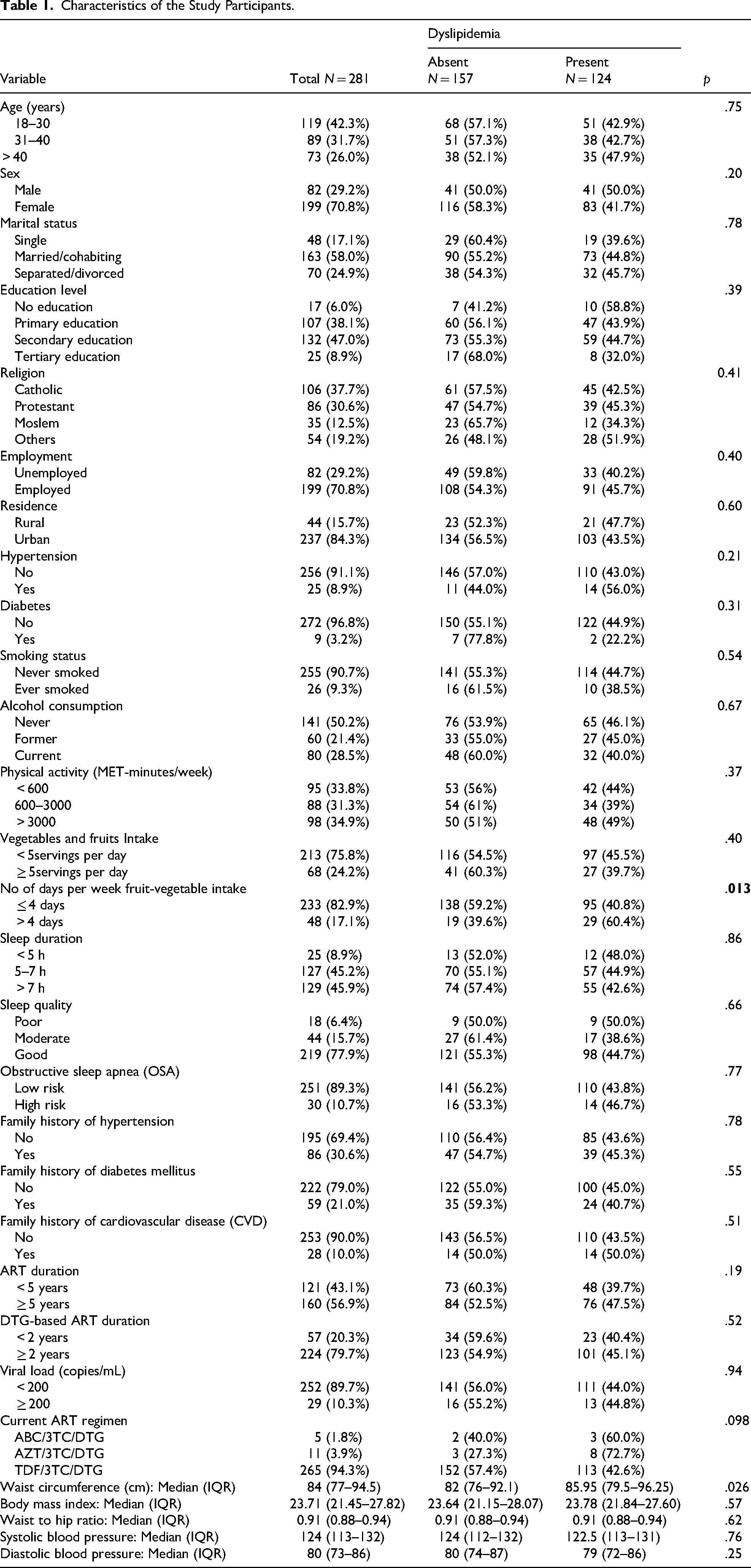
Table 1 presents the sociodemographic, lifestyle, clinical, and anthropometric characteristics of 281 participants enrolled in our study categorized by dyslipidemia status. The majority were female (70.8%), aged 18–40 years (74%), married or cohabiting (58.0%), with secondary education (47.0%), and resided in urban areas (84.3%). No sociodemographic factors were significantly associated with dyslipidemia (p > .05). Hypertension (8.9%) and diabetes (3.2%) were uncommon and not significantly associated with dyslipidemia (p = .21 and p = .31, respectively).
Characteristics of the Study Participants.
Proportion of Participants with Abnormal Lipid Profile.
Lifestyle factors, including smoking (9.3%), alcohol consumption (28.5%), and physical activity levels, did not show significant associations with dyslipidemia prevalence (p > .05). However, the prevalence of dyslipidemia was significantly higher in the participants with frequent vegetative intake ( > 4 days/week) compared to their counterparts ( > 4 days/week), 60.4% versus 40.8%, p = .013. Sleep patterns, OSA risk, family history of metabolic disorders, ART duration, and viral load suppression were not significantly associated with dyslipidemia.
The median WC was significantly higher in participants with dyslipidemia (85.95 cm, IQR: 79.5–96.25) compared to those without (82 cm, IQR: 76–92.1) (p = .026). However, body mass index (BMI) and waist-to-hip ratio did not show significant associations (p = .57 and p = .62, respectively). Systolic and diastolic blood pressures also did not differ significantly by dyslipidemia status (p = .76 and p = .25, respectively). The majority of study participants had been on DTG-based ART for ≥ 2 years, with no significant difference in the observed prevalence of dyslipidemia in this group compared to those who had been on DTG-based ART for < 2 years ((45.1%) versus 40.4%, p = .52) (Table 1).
Table 3 presents the factors associated with dyslipidemia among PLHIV on DTG-based ART. After adjustment for confounding effects, increased WC was significantly associated with a higher prevalence of dyslipidemia (aPR: 1.93, 95% CI: 1.15–3.24, p = .013).
Factors Associated with Dyslipidemia.

Abbreviations: cPR, crude prevalence ratio; aPR, adjusted prevalence ratio. The cPR reflects the unadjusted association between independent variables and outcome variable (dyslipidemia), whereas the aPR indicates the association after controlling for potential confounding variables in multivariable regression analysis.
Predictive Performance of WC for Dyslipidemia and Abnormal Lipid Parameters
Figures 2–5 illustrate the ROC curves assessing the predictive ability of WC for dyslipidemia, hypercholesterolemia, low HDL-cholesterol, and high LDL-cholesterol. The predictive ability of WC for dyslipidemia and abnormal lipid parameters was assessed using ROC curve analysis, with the AUC and its 95% confidence interval (CI) serving as the key performance measure. AUC values closer to 1 indicate stronger discriminatory ability. A parameter is considered significantly predictable by WC if the 95% CI of the AUC does not include the null value of 0.5, which indicates random classification. The optimal cut-off point for WC was also determined alongside its sensitivity and specificity for each lipid abnormality.

Receiver Operating Characteristic Curve Showing Predictive Ability of Waist Circumference for Dyslipidemia.

Receiver Operating Characteristic Curve Showing Predictive Ability of Waist Circumference for Hypercholesterolemia.

Receiver Operating Characteristic Curve Showing Predictive Ability of Waist Circumference for HDL-Cholesterol.

Receiver Operating Characteristic Curve Showing Predictive Ability of Waist Circumference for LDL-Cholesterol.
WC demonstrated a significant ability to predict dyslipidemia, hypercholesterolemia, and elevated LDL-C. However, it was not a significant predictor of low HDL-C in this study.
The AUC for WC in predicting dyslipidemia was 0.577 (95% CI: 0.511–0.644), indicating a moderate ability to discriminate between individuals with and without dyslipidemia. The optimal WC cut-off point was 80.0 cm, with a sensitivity of 73% and specificity of 43%, suggesting that individuals with a WC ≥ 80.0 cm have a higher likelihood of having dyslipidemia. Since the 95% CI does not include 0.5, WC is a significant predictor of dyslipidemia in this population (Figure 2).
The AUC for WC in predicting hypercholesterolemia (Total Cholesterol ≥ 200 mg/dL) was 0.702 (95% CI: 0.547–0.857), suggesting a good predictive ability. The optimal WC cut-off was 102.3 cm, with a sensitivity of 44% and a specificity of 94%, implying that WC is a significant predictor of hypercholesterolemia, as the confidence interval does not include 0.5 (Figure 3). Individuals with WC ≥ 102.3 cm are at a higher risk of having hypercholesterolemia.
The AUC for WC in predicting low HDL-Cholesterol level was 0.548 (95% CI: 0.481–0.616), with an optimal WC cut-off of 80.0 cm, a sensitivity of 72%, and a specificity of 41%. Since the 95% CI includes 0.5, WC does not significantly predict low HDL-Cholesterol level, indicating a weak discriminatory ability (Figure 4).
For LDL-C, the AUC was 0.729 (95% CI: 0.590–0.867), and the optimal WC cutoff was 84.8 cm. Sensitivity and specificity at this cutoff were 94% and 54%, respectively. WC was therefore noted to have a significant and good predictivity power to discriminate between individuals with and without elevated LDL-C levels ( ≥ 130 mg/dL) as the confidence interval of AUC does not include 0.5. Individuals with WC ≥ 84.8 cm are at a higher likelihood of having elevated LDL-C levels (Figure 5).
Discussion
This study revealed a notable prevalence of dyslipidemia among PLHIV on DTG-based ART in Central Uganda, with 44.1% (95% CI: 38.4%–50.0%) of participants presenting with lipid abnormalities. The most frequent lipid abnormality observed was low high-density lipoprotein cholesterol (HDL-C), affecting 39.9% of participants. These findings raise significant clinical concerns given the role of low HDL-C in increasing the risk of cardiovascular diseases, particularly among patients already burdened by chronic conditions like HIV.28,29 While DTG has been favored for its potent virologic suppression and tolerability, emerging evidence, including the present study, highlights the metabolic complications associated with its use.8–10
In Uganda's general non-HIV adult population, dyslipidaemia prevalence has generally been lower than the 44.1% we observed. For example, Bazil et al. (2019) found dyslipidaemia in about one-third of community adults. 30 The 2014 WHO STEPS survey reported only 6.7% of Ugandan adults with raised total cholesterol. 31 Similarly, an older rural Uganda study found 75% prevalence. 32
The findings from our study align closely with those from Nigeria and Ethiopia, where prevalence rates of 44.7% and 55.2% were reported, respectively. 33 This similarity could be due to comparable sociodemographic characteristics of the study populations and similarities in ART regimens. Additionally, these studies were conducted in resource-limited settings where routine metabolic monitoring is uncommon, potentially resulting in a shared burden of undetected and unmanaged dyslipidemia.
However, the observed prevalence in our study is below that reported in Kampala at Mengo Hospital, where 78.0% of participants on DTG-based ART had dyslipidemia, with low HDL-C recorded in 72.1% of cases. 11 These differences could be due to variations in the demographic profiles of participants, particularly age and sex. Notably, participants in the study at Mengo had a higher median age and a greater proportion of females, factors known to influence lipid profiles. Furthermore, lifestyle factors such as levels of physical activity and dietary patterns may have differed between the two study populations, contributing to the observed variation. Comparatively, studies from Ethiopia have reported high dyslipidemia rates among people on ART, reaching 63.9%, 34 while a systematic review from the region reported a pooled prevalence of 67.32%. 35 An even higher prevalence of 86.6% was reported in Eritrea, 36 further highlighting the substantial burden of dyslipidemia among HIV-positive patients across different African settings.
On the other hand, in this study, WC was associated with dyslipidemia. Participants with higher WC had nearly twice the risk of dyslipidemia (aPR = 1.93, 95% CI: 1.15-3.24, p = .013). This is in line with earlier findings showing that WC is a good predictor of lipid abnormalities.37,38 In our ROC analysis, WC showed moderate predictive ability for overall dyslipidemia (AUC = 0.577), and stronger performance for predicting hypercholesterolemia (AUC = 0.702) and elevated LDL-C (AUC = 0.729). These findings are corroborated by studies in Ethiopia and Kenya that identified WC as a strong predictor of adverse lipid profiles among PLHIV.38,39 Therefore, in environments with limited resources where thorough lipid testing may not be regularly available, WC can be used as an easy and trustworthy screening method for dyslipidemia.
Overall, the study highlights that while DTG remains a cornerstone of HIV management due to its virologic efficacy and favorable tolerability profile, its potential contribution to the development of dyslipidemia cannot be overlooked. These findings emphasize the need for integration of metabolic monitoring, including WC assessments and, where feasible, lipid profiling into HIV care services.
Conclusions
Our study reveals a significant prevalence of dyslipidemia among individuals on DTG-based ART in Central Uganda, with WC emerging as a key predictor of lipid abnormalities.
Recommendations
Given the predictive value of WC for hypercholesterolemia, we recommend incorporating routine WC measurements alongside periodic lipid profiling into HIV care for patients on DTG-based ART. Early identification of dyslipidemia should be followed by lifestyle interventions including weight management. Where abnormalities persist or are severe, initiation of lipid-lowering therapy such as statins should be considered in line with existing guidelines. Future research should focus on understanding the mechanisms linking DTG to lipid abnormalities, evaluating cost-effective screening strategies, and developing tailored interventions to reduce cardiovascular risk in this population.
Study Strengths and Limitations
This study had several notable strengths. The use of a systematic sampling technique enhanced the representativeness of participants recruited from the ART clinic, thereby minimizing selection bias and improving the generalizability of the findings to similar settings in Central Uganda. Standardized and rigorous measurements were employed throughout the study, with anthropometric parameters assessed using validated protocols and lipid profiles measured in an accredited laboratory, ensuring high data quality and reliability. Additionally, the specific focus on DTG-based ART regimens addressed a timely and important clinical issue, as DTG is increasingly being adopted as the first-line therapy globally, yet its long-term metabolic consequences remain insufficiently understood.
However, the study was not without limitations. The exclusion of triglyceride measurements due to the use of non-fasting blood samples. Since triglycerides are a critical component of the lipid profile, the overall burden of dyslipidemia may have been underestimated. Conducting the study at a single health facility may also limit the external validity of the findings, as differences in population demographics or healthcare delivery practices across regions could influence dyslipidemia patterns. Some subgroups within the sample, such as individuals with diabetes or smokers, were relatively small, limiting the statistical power to detect significant associations in these strata.
Footnotes
Abbreviations
Acknowledgements
We acknowledge the study participants who agreed to take part of our study.
Ethical Approval and Informed Consent
The Mbarara University of Science and Technology Faculty Research Committee (FRC) granted ethical approval for this work under approval number MUST/MLS/24-02U. Prior to performing the study, administrative clearance was also acquired from Kira Health Center IV's Office of the In-charge. Prior to participation in this study, each participant provided written informed consent. The 1975 Declaration of Helsinki's ethical criteria (1964) were followed in this study protocol. Each study participant was assigned a code that could not be linked to them in order to maintain participant confidentiality. Additionally, participants were made aware that their involvement in the study was completely voluntary and free, and they could leave at any moment.
Authors’ Contributions
FT, CNB, HS, TW, FB, JS participated in conceptualization of the study and data collection. CNB did data analysis and results interpretation. FT, CNB, HS, TW, FB, JS, ES, MJM, EN, SO, CN, JAW, BM, WA, LOO contributed to writing the first draft of the manuscript with CNB, LOO, BM providing critical revisions. All authors read and approved the first manuscript.
Consent for Publication
All authors consented to the publication of this research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The dataset generated and analyzed during this study is available upon request from the corresponding author.