
Abstract
Purpose
This study aimed to assess the burden of metabolic syndrome among people living with HIV (PLWH) on dolutegravir (DTG)- and efavirenz (EFV)-based regimens.
Methods
A hospital-based comparative cross-sectional study design was implemented from May 5, 2022, to August 5, 2022.
Results
The overall prevalence of metabolic syndrome was 18.6% (32/172) for all regimens, with 25.6% (22/86) for the DTG- and 11.6% (10/86) for the EFV-based regimens (P = .019). Body mass index ≥ 25 kg/m2 (adjusted odds ratio [AOR] = 3.04; 95% confidence interval [CI]: 1.13-8.14), CD4 count ≥ 500 cells/mm3 (AOR = 3.01; 95% CI: 1.09-8.28), insufficient physical activity (AOR = 2.60; 95% CI: 1.00-6.72), and DTG-based regimen (AOR = 2.86; 95% CI: 1.14-7.20) were associated with metabolic syndrome.
Conclusion
The prevalence of metabolic syndrome was significantly higher among PLWH on DTG-based regimens. This signifies that DTG-treated patients should be advised on lifestyle adjustments to prevent the development of metabolic syndrome.
Introduction
The implementation of combination antiretroviral therapy (ART) has substantially benefited people living with HIV (PLWH) in terms of quality of life, body immunity improvement, increased survival, and psychological boost.1–3 Despite these beneficial effects, long-term toxicities are starting to appear with prolonged use of ART, posing new challenges to the effective management of HIV infection.4–6 Exposure to ART treatment can induce lipodystrophy, dyslipidemia, and insulin resistance, which increases the risk of developing metabolic syndrome.7,8 Metabolic syndrome is a health condition that comprises abdominal obesity, hypertension, dyslipidemia, and insulin resistance. 9 It is a major public health concern in many parts of the world due to its strong association with a 5-fold risk of type 2 diabetes mellitus and a 2-fold risk of cardiovascular diseases. 10 Therefore, diagnosing metabolic syndrome early could help prioritize interventions to reduce the risk of these cardiometabolic diseases and improve the long-term health of PLWH. 11
The worldwide occurrence of metabolic syndrome among PLWH has been approximated to be around 16.7% to 32.3%. 12 A meta-analysis carried out in Sub-Saharan Africa indicated that metabolic syndrome is more common in PLWH, with a prevalence of 21.5% compared to 12% in the general population. 13 In Ethiopia, the pooled prevalence of metabolic syndrome among PLWH ranges from 21.54% to 38.28%. 14
Antiretroviral treatments have changed over time, and certain medications with significant metabolic side effects have been eliminated from the treatment guidelines. 15 In response to reports of primary resistance to non-nucleoside reverse transcriptase inhibitors (NNRTIs) exceeding the recommended 10% threshold, the World Health Organization (WHO) endorsed the use of dolutegravir (DTG), a second-generation integrase inhibitor, in both first- and second-line therapy. 16 Consequently, many countries in Sub-Saharan Africa have adopted DTG-based regimens as their first-line ART due to their high resistance barrier, improved tolerability, and decreased drug interactions.17,18 Nevertheless, despite their favorable tolerability profile, DTG-based ART has been linked to weight gain and hyperglycemia,19,20 which are risk factors for metabolic syndrome.
There is minimal research available on the impact of metabolic syndrome in the age of improved ART medications like DTG. The existing evidence is conflicting, with certain studies indicating a reduction in metabolic syndrome with DTG-based regimens,21,22 while others suggest a significant link between DTG-based regimens and metabolic syndrome.23,24 For instance, a cross-sectional study conducted in Zambia involving 635 PLWH on NNRTIs (efavirenz [EFV] and nevirapine [NVP]), PIs (lopinavir/ritonavir and atazanavir/ritonavir), and integrase inhibitors (DTG) found that PLWH on a DTG-based regimen had elevated blood pressure (BP), waist circumference (WC), and dyslipidemia associated with metabolic syndrome. 23 Conversely, a recent study from Tanzania found that a DTG-based regimen does not affect the prevalence of metabolic syndrome. 25
To the best of our knowledge, there are no reports on the burden of metabolic syndrome and its associated factors among PLWH on DTG and EFV-based regimen, particularly in the study area. Therefore, this study aimed to compare metabolic syndrome among PLWH on DTG- and EFV-based regimen, as well as identify factors associated with an increased risk of metabolic syndrome in this population.
Method and Materials
Study Design and Setting
A hospital-based comparative cross-sectional study was conducted at the ART clinic of Dessie Comprehensive Specialized Hospital (DCSH). Dessie Comprehensive Specialized Hospital is found in Dessie town, which is located 401 km from Addis Ababa, the capital city of Ethiopia. In DCSH, there is a separate ART clinic that gives services to PLWH. As of April 1, 2022, the hospitals serve about 6550 PLWH; among these, 5076 were on DTG + lamivudine (3 TC) + Tenofovir disoproxil fumarate (TDF), and 381 were on EFV + 3 TC + TDF. The clinic offers care to patients from nearby rural areas and towns. Presently, ART clinic of DCSH provides comprehensive health services in the following areas: voluntary counseling and testing, prevention of mother-to-child transmission of HIV, follow-up care for PLWH for ART therapy, and treatment of opportunistic infections.
Study Populations and Study Processes
The study was carried out from May 5, 2022, to August 5, 2022. All PLWH aged ≥18 years who had received DTG- and EFV-based regimens for at least 6 months were included. However, patients with known diabetes mellitus or hypertension before ART initiation, thyroid disease, liver disease, renal disease, and pregnant and lactating women were excluded from this study.
Sample Size Determination and Sampling Technique
The G* power statistical power analysis version 3.1 program was used to determine the total number of study participants. The sample size was determined based on an alpha (α) of 0.05, a power (1-β) of 0.9 (90%), with a DTG to EFV-based regimen ratio of 1:1, 2-independent groups mean t test, and an effect size (d) of 0.5. The resulting sample size was determined to be 172 participants, with 86 in the DTG-based group and 86 in the EFV-based group. A purposive sampling technique was applied to select study participants.
Data Collection Procedure
Data on sociodemographic, behavioral, and clinical characteristics were collected using a questionnaire adapted from the WHO STEP-wise approach to chronic disease risk factor surveillance26,27 via patient interviews and chart reviews. After the participants were asked for their consent, an interviewer-administered questionnaire was used to gather sociodemographic and behavioral characteristics of the participants. The patient's chart review was used to collect the clinical characteristics of the participants. Procedures for the collection of data on variables such as anthropometric (weight, height, WC) and BP were standardized prior to being used for actual patient data collection. All the measurements were carried out under the standard operating procedure by trained data collectors (nurses) under strict supervision for the quality of the data. Anthropometric measurements like WC were measured on the midpoint between the inferior angle of the ribs and the suprailiac crest, with the erect stand-up position following normal out breathing by a flexible inelastic tape to the nearest 0.1 cm. Bodyweight was determined to the nearest 100 g using a Tanita scale, and height was measured to the nearest 1 mm using a stadiometer. After that, the body mass index (BMI) was calculated using kg/m2 formula. Blood pressure was measured using a mercury sphygmomanometer. Blood pressure was assessed as the average of the two measurements taken at intervals longer than 5 min after the patient had been sitting for at least 5 or 30 min for those who take hot drinks like coffee.
Blood Samples Collection
A laboratory technologist collected about 5 mL of blood from each study subject after an overnight or a minimum of 8 h of fasting from the antecubital vein to determine the fasting blood glucose (FBG) level and lipid profiles. The blood samples were analyzed for FBG level and lipid profile (total cholesterol, high-density lipoprotein cholesterol [HDL-C], and low-density lipoprotein cholesterol) through the enzymatic method using a Siemens Dimension EXL 200 System clinical chemistry laboratory.
Operational Definitions
Metabolic syndrome: Based on IDF 2005 criteria, metabolic syndrome was diagnosed if central obesity (WC of ≥94 cm for men and ≥80 cm for women) was accompanied by any two of the following risk factors: raised TG level (≥150 mg/dL) or presence of treatment for this lipid abnormality; low HDL-C (<40 mg/dL for men or <50 mg/dL for women) or presence of treatment for this lipid abnormality; systolic BP ≥ 130 mm Hg and/or diastolic BP ≥ 85 mm Hg or pharmacological treatment of previously diagnosed hypertension and raised FBG (≥100 mg/dL) or previously diagnosed T2DM. 28
Regarding physical activity: Vigorous-intensity activities are activities that require hard physical effort and cause large increases in breathing or heart rate for at least 10 min continuously (eg, running, carrying or lifting heavy loads, digging, or construction work). 29 Moderate-intensity activities are activities that require moderate physical effort and cause small increases in breathing or heart rate for at least 10 min continuously. 29
Sufficient physical exercise: Adults should do at least 150 to 300 min of moderate-intensity aerobic physical activity, or at least 75 to 150 min of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate-intensity and vigorous-intensity activity per week and otherwise insufficient. 30
Low fruit and vegetable intake was defined as consuming less than five servings of fruit and vegetables per day. 31 For raw green leafy vegetables, 1 serving = 1 cup; for cooked or chopped vegetables, 1 serving = ½ cup; for fruit (banana, orange etc…), 1 serving = 1 medium size piece; for chopped, cooked, and canned fruit, 1 serving = ½ cup; and for juice from fruit, 1 serving = ½ cup. 32
Educational status: A person was designated as uneducated if they had not formal education; while a person was recognized as educated if they had at least completed primary school. 33
Viral loads >
Data Processing, Analysis, and Presentation
The data were cleaned, coded, and entered into Epi Data version 4.6 and exported to the Statistical Package for Social Science version 26 for analysis. Descriptive analysis was carried out and results were presented using tables and figures. Categorical variables were presented as number and percentage, computed using the chi-square test to detect differences between the groups. Bivariable and multivariable binary logistic regression models were used to investigate the relationships between outcome variables and potential associated factors. For the final analysis, variables with P-values <.25 in bivariable logistic regression were fitted into the multivariable logistic regression model. The crude odds ratio and adjusted odds ratio (AOR) with 95% confidence intervals (CIs) were reported. Variables having a P value of <.05 at 95% CI with multivariable logistic regression were considered statistically significant. The variance inflation factor (VIF) was found to be acceptable when multicollinearity among selected independent variables was tested (since the VIF was less than 2 in our study). The Hosmer and Lemeshow's test was used to assess the goodness of fit of the final logistic model.
Results
Sociodemographic and Behavioral Characteristics of the Participants
A total of 172 PLWH on ART (86 DTG- and 86 EFV-based ART) were enrolled. The proportion of patients with an age greater than 45 was 51.2% and 38.4% in the DTG- and EFV-treated patients, respectively (P = .092). There were 61.6 and 57% female participants in the DTG and EFV groups, respectively (P = .535). Between our study groups, a statistically insignificant difference was detected in all of their sociodemographic and behavioral characteristics that are described in Table 1
Sociodemographic and Behavioral Characteristics of PLWH on DTG- and EFV-Based Regimens at DCSH.
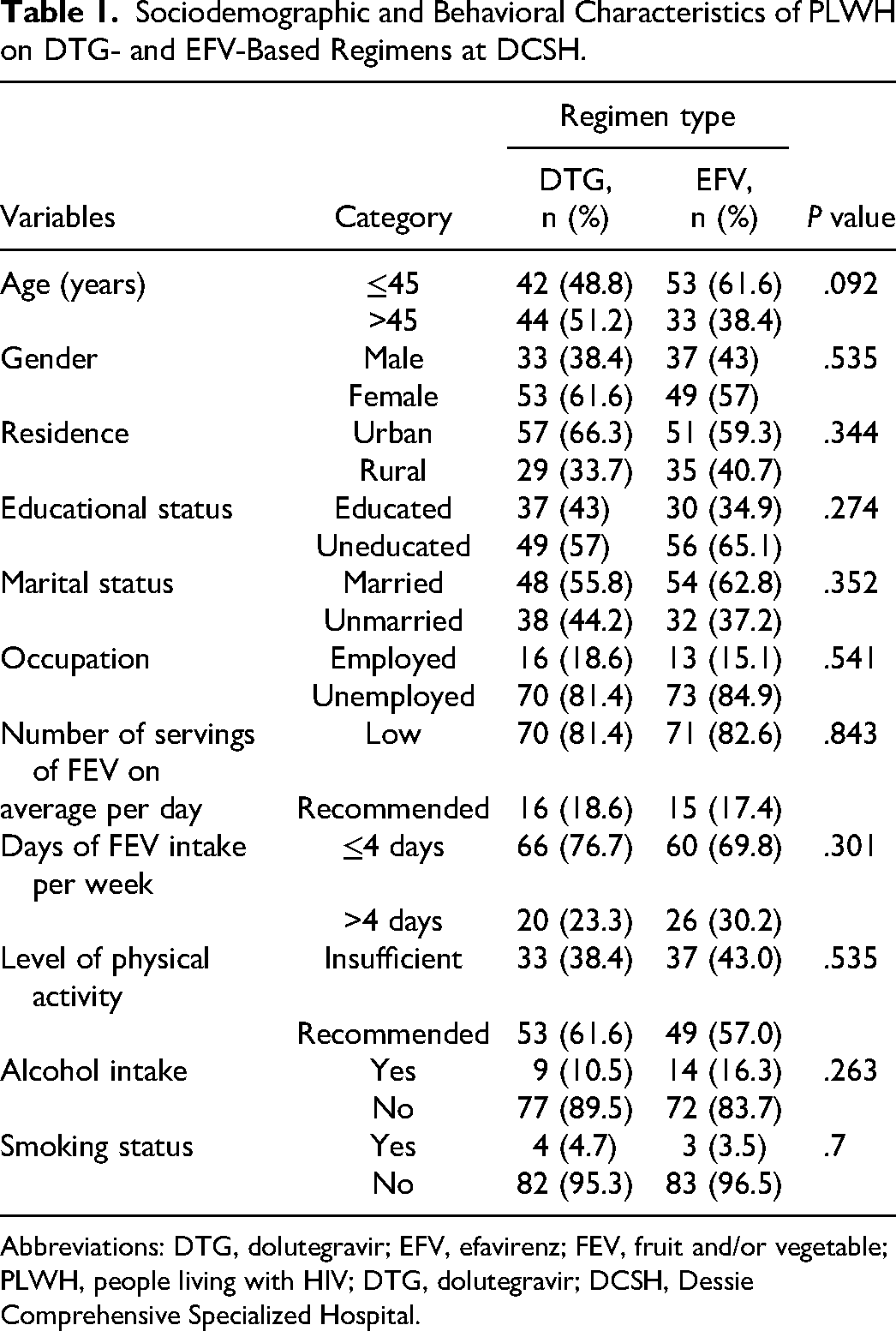
Abbreviations: DTG, dolutegravir; EFV, efavirenz; FEV, fruit and/or vegetable; PLWH, people living with HIV; DTG, dolutegravir; DCSH, Dessie Comprehensive Specialized Hospital.
Clinical, Anthropometric, and Biochemical Characteristics of the Participants
This study demonstrates that 65.1% of patients on the DTG-based regimen and 73.3% on the EFV-based regimen had a CD4 count of <500 cells/mm3 (P = .248). About 25.6% of DTG and 16.3% of EFV-treated patients had a BMI ≥ 25 kg/m2 (P = .134). In addition, 61.6% of the DTG and 43% of the EFV-prescribed patients had low HDL-C levels (P = .015) (Table 2).
Clinical, Anthropometric, and Biochemical Characteristics of PLWH on DTG- and EFV-Based Regimens at DCSH.

Abbreviations: CD4, cluster of differentiation 4; HIV, human immunodeficiency virus; ART, antiretroviral therapy; AIDS, acquired immune deficiency syndrome; WHO, World Health Organization; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; DTG, dolutegravir; EFV, efavirenz; PLWH, people living with HIV; DCSH, Dessie Comprehensive Specialized Hospital.
P < .05.
The Magnitude of Metabolic Syndrome Among Study Participants
The prevalence rate was estimated based on the IDF definition and found to be 18.6% (32/172) among all participants. The prevalence of metabolic syndrome shown in Figure 1 was 25.6% (22/86) and 11.6% (10/86) among DTG- and EFV-treated patients (P = .019). In terms of the prevalence of metabolic syndrome components, low HDL-C (61.6%) was the most prevalent in the DTG group, followed by elevated TG levels (44.2%), whereas in the EFV group, elevated TG levels (48.8%) were the most prevalent, followed by low HDL-C (43%).

Prevalence of metabolic syndrome among people living with HIV (PLWH) on dolutegravir (DTG) and efavirenz (EFV)-based regimens at Dessie Comprehensive Specialized Hospital (DCSH).
Factors Associated With Metabolic Syndrome Among PLWH on DTG and EFV-Based ART
Age, gender, educational status, duration of ART, duration of HIV infection, CD4 count, current regimen type, BMI, and physical activity had a P-value <.25 in bivariable analysis and were fitted into the multivariable binary logistic regression model for final analysis. After adjusting for all these variables in multiple logistic regressions, BMI ≥ 25 kg/m2 (AOR = 3.04; 95% CI: 1.13-8.14; P = .027), CD4 count ≥ 500 cells/mm3 (AOR = 3.01; 95% CI: 1.09-8.28; P = .033), insufficient physical activity (AOR = 2.60; 95% CI: 1.00-6.72; P = .049), and DTG-based regimen (AOR = 2.86; 95% CI: 1.14-7.20; P = .025) were significantly associated with metabolic syndrome (Table 3).
Factors Associated With Metabolic Syndrome Among PLWH on DTG-Based and EFV-Based Regimens at DCSH.
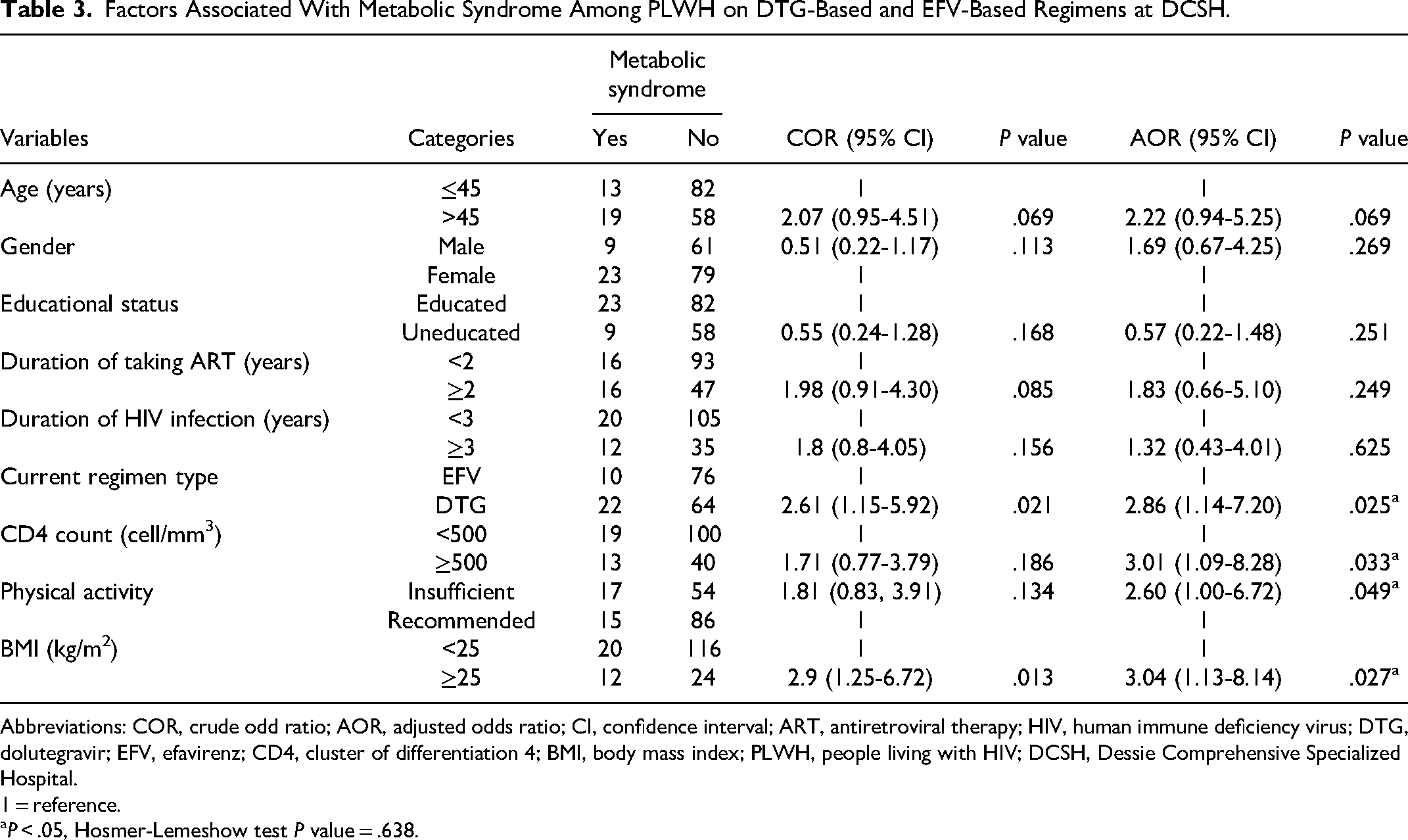
Abbreviations: COR, crude odd ratio; AOR, adjusted odds ratio; CI, confidence interval; ART, antiretroviral therapy; HIV, human immune deficiency virus; DTG, dolutegravir; EFV, efavirenz; CD4, cluster of differentiation 4; BMI, body mass index; PLWH, people living with HIV; DCSH, Dessie Comprehensive Specialized Hospital.
1 = reference.
P < .05, Hosmer-Lemeshow test P value = .638.
Discussion
There has been a paucity of data on the potential burden of metabolic syndrome and other cardiometabolic factors among PLWH on DTG and EFV-based regimens in Africa, particularly in Ethiopia. This study aimed to determining the prevalence and predictors of metabolic syndrome among DTG and EFV-based regimens receiving patients.
In this study, the prevalence of metabolic syndrome was 25.6% (22/86) among the DTG and 11.6% (10/86) among the EFV-treated patients. This finding is higher compared with the ADVANCE and NAMSAL clinical trials. 35 In the ADVANCE clinical trial, metabolic syndrome was present in 10% of DTG and 7% of EFV-based ART-treated participants. In the NAMSAL clinical trial, metabolic syndrome was 14% in DTG and 5% in EFV-based ART-treated participants. However, our finding was lower than that of a cross-sectional study conducted in Zambia that showed the prevalence of metabolic syndrome in DTG is 30.08% (40/133) and 26.27% (248/944) in the NNRTI (EFV and NVP) group. 23 The discrepancy between the present study and other studies may be due to the difference in sample size and sampling technique, the differences in study approaches (different in patients’ selection criteria such as age, weight, and ART combinations), the difference in duration of ART treatment, and the difference in socioeconomic status. For instance, the ADVANCE and NAMSAL clinical trials were conducted with a larger sample size than the current study; in addition, the discrepancy in the result might be due to the fact that participants in clinical studies may be withdrawn due to treatment side effects. 35 Likewise, a cross-sectional study from Zambia was also conducted with a large sample size as compared with our study. 23
In comparing the prevalence of metabolic syndrome between the two groups, the study observed a higher prevalence rate in the DTG group (25.6%) compared to the EFV group (11.6%), with a statistically significant difference (P = .019). Although our study encountered challenges when comparing data to similar published studies that investigated the metabolic syndrome in PLWH on DTG and EFV-based ART in comparative studies, our findings contradicted those of studies conducted in Guatemala 36 and Tanzania. 25 The observed variation could be due to differences in sample size and the cutoff point to define metabolic syndrome. For example, a previous study from Guatemala had a larger sample size compared to the present study, and it utilized Latin American Diabetes Association criteria for metabolic syndrome as well as specific cutoff values for WC. In the Guatemalan study, the cutoff for central obesity in women was ≥90 cm, while in our study, it was ≥80 cm. Additionally, the cutoffs for elevated BP were 130/90 mm Hg in the Guatemalan study and ≥130/85 mm Hg in our study. 36 In addition, a study from Tanzania was also conducted with a larger sample size as compared with the present study. 25 Moreover, the higher prevalence of metabolic syndrome among PLWH on DTG-based ART may be attributed to a statistically significant difference in low HDL-C levels between those receiving DTG-based ART (61.6%) and those receiving EFV-based ART (43%) (P = .015). Previous clinical trials conducted predominantly among white populations showed that DTG had a neutral effect on lipid profile37,38; however, several recent studies conducted among black Africans revealed that DTG-based ART was associated with a high prevalence of low HDL-C levels.20,39–40 Therefore, race-specific data on the impact of the DTG-based ART on lipid profile are needed. On the other hand, the available data suggest that prolonged EFV therapy and its concentration are positively correlated with HDL-C levels. 41 The potential molecular mechanism by which EFV raises HDL-C levels is by reducing the expression of cholesterol ester transfer protein through antagonism of the lipid transcription factor. 42
The present study also attempted to identify the factors associated with metabolic syndrome among patients on ART. Accordingly, the odds of developing metabolic syndrome were 2.86 times greater in participants with a DTG-based regimen than in participants with an EFV-based regimen. Our finding was consistent with some previous studies on the association of a DTG-based regimen with metabolic syndrome. 43 This might be explained by recent research indicating that INSTIs, particularly DTG, may suppress the expression of adiponectin and leptin while upregulating the expression of pro-inflammatory cytokines such as interleukin-6, which could lead to weight gain and metabolic dysregulation.44,45 Therefore, ongoing clinical monitoring is essential for ART, particularly when choosing the initial treatment regimen and making decisions about switching or substituting medications. Clinicians need to assess patients’ overall risk factors through thorough clinical evaluations and implement suitable approaches to prevent and manage metabolic disorders. 46
In addition, we observed that BMI was significantly associated with metabolic syndrome. Participants who had a BMI ≥ 25 kg/m2 were 3.04 times more likely to have metabolic syndrome compared to participants who had a BMI < 25 kg/m2. This finding is consistent with other studies that showed a significant relationship between BMI and metabolic syndrome.47,48 The result could be explained by the contribution of increased body weight to central obesity, which leads to fat accumulation in the body. Fat deposits form artery plaque, which narrows arteries and capillaries, leading to elevated BP (hypertension) and decreasing insulin sensitivity (insulin resistance), consequently leading to a greater risk of metabolic syndrome.49,50 Thus, incorporating body fat measurements in HIV clinics would help to identify people at high risk of metabolic syndrome early on and institute lifestyle modifications to minimize the risk of metabolic syndrome and other noncommunicable diseases.
Furthermore, CD4 count was also significantly associated with metabolic syndrome. The odds of developing metabolic syndrome were approximately three times greater in patients with a CD4 count ≥500 cells/mm3 than in patients with a CD4 count <500 cells/mm3. This significant association was observed in other similar studies.47,51 One explanation for the higher CD4 count being associated with metabolic syndrome is that these participants with restored immune systems have been living with HIV and on ART for longer period of time and may be experiencing cumulative effects of the disease or antiretroviral drugs. 52
Moreover, insufficient physical activity was found to be associated with the development of metabolic syndrome. Participants who had insufficient physical activity were 2.60 times more likely to develop metabolic syndrome compared to those participants who had recommended physical activity. This finding is supported by the study among PLWH on ART in South Africa, 53 Guatemala, 54 and Ethiopia. 55 This association might be explained by the fact that an imbalance in energy, caused by an excessive energy intake and insufficient physical activity, is a key factor leading to obesity and the onset of metabolic syndrome. This association might be explained by the effect of adequate physical activity on burning more energy, which helps prevent the buildup of fat and weight gain. 56 In addition, physical activity reduces metabolic risks by improving physiological parameters such as systemic inflammation, insulin resistance, blood lipid profile, HIV-associated lipodystrophy, and WC.57,58 Thus, the risk of metabolic syndrome is increased by insufficient physical exercise.
As a strength, to the best of our knowledge, this was the first study in Ethiopia that attempted to assess the burden of metabolic syndrome among PLWH on DTG and EFV-based regimens, hence ultimately adding to the limited data. Despite the aforementioned strength, this study has several weaknesses. This is a comparative cross-sectional study; thus, we cannot associate causal relationships between the factors and outcomes under study. In addition, the study sample size was small and the sampling coming from one hospital at a specific period; thus, it is difficult to generalize the findings to larger populations. Moreover, the study did not include healthy controls as a comparative group which would have provided better insight into the role of HIV infection and ART.
Conclusion and Recommendation
Overall, this study demonstrated an elevated degree of metabolic syndrome in PLWH on ART. Also, the prevalence of metabolic syndrome was significantly higher in the DTG group than in the EFV group. This signifies that PLWH on ART (especially DTG-treated patients) should be advised on lifestyle adjustments to prevent the development of metabolic syndrome. DTG-based regimen, higher CD4 count, insufficient physical activity, and increased BMI were significantly associated with metabolic syndrome among PLWH on ART. So, there is a need for close monitoring of BP, blood glucose levels, and serum lipid profiles of PLWH on ART, with special attention focused on patients with a higher BMI, a higher CD4 count, insufficient physical activity, and those on a DTG-based regimen. Finally, we propose that researchers conduct a prospective cohort study with a larger sample size to draw an exact conclusion regarding the burden of metabolic syndrome among PLWH on DTG and EFV-based regimens.
Footnotes
Abbreviations
Authors’ Note
Ethics Approval and Informed Consent: The study was carried out in accordance with the ethical principles of the Declaration of Helsinki. The ethical clearance was obtained from the Ethical Review Board of the University of Gondar, School of Medicine (reference number: 677/04/2022). An official permission letter was also obtained from the managers of DCSH. Written informed consent was obtained from all study participants before the data collection, after discussing the purpose and method of the study. The study participants were informed that they had the complete right to discontinue or refuse participation. COVID-19 infection prevention measures recommended by the WHO were strictly followed during data collection to reduce the risk of infection transmission. Availability Data and Materials: The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Acknowledgments
The authors would like to give our thanks to the data collectors, University of Gondar, and Dessie Comprehensive Specialized Hospital for their unreserved contributions.
Authors’ Contribution
MJ conceived the research idea, conducted the data analysis and interpretation, and wrote and reviewed the paper. AA, MG, BA, DS, and TB reviewed and approved the final paper. TB, DS, AA, NC, and MG analyzed the data and reviewed the drafts. MJ, the corresponding author, had the responsibility to submit the manuscript for publication. All the authors contributed to data analysis, drafted or revised the article, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.