
Abstract
Background
Dolutegravir (DTG)-based antiretroviral therapy (ART) has been associated with weight gain and obesity which are also linked to hepatocellular dysfunction. Despite these associations, the link between obesity indices and hepatocellular damage among people living with human immunodeficiency virus (PLWH) on DTG-based ART remains poorly understood. This study examined the association between obesity indices and elevated serum transaminases, markers of liver damage, among PLWH on DTG-based ART in Southwestern Uganda.
Methods
We conducted a cross-sectional study among 212 PLWH aged 18years and above who had been on DTG-based ART for ≥1 year at Municipal Health Centre IV, Southwestern Uganda. Data was collected using a semi-structured questionnaire. Anthropometric measurements were taken, and a blood sample collected from each participant for laboratory measurement of serum alanine and aspartate transaminase activity.
Results
Elevated serum transaminase activity was found in 12.7% (27/212, 95% confidence interval (CI): 8.9%-18.0%) of participants. Participants with elevated transaminases had significantly higher median waist-to-hip ratio (0.88 vs 0.83, P < 0.001) and waist circumference (WC) to body mass index (BMI) ratio (3.56 vs 3.42, P = 0.026) compared to those with normal activity. In multivariate analysis, only WC/BMI ratio remained significantly associated (aOR = 3.68; 95% CI: 1.11-12.16; P = 0.033) with elevated serum transaminase activity. At an optimal cut-off of 3.45; sensitivity = 78%, specificity = 52%), WC/BMI had significantly predictive power, (area under the curve= 0.651; 95% CI: 0.580-0.722) for elevated serum transaminase activity.
Conclusion
WC/BMI ratio is a potential predictor of elevated transaminases among PLWH on DTG-based ART in South western Uganda.
Plain Language Summary Title
Using Waist Size Compared to Body Weight to Detect Liver Damage in Ugandan Patients on Dolutegravir
Plain Language Summary
People living with HIV are now living longer because of improved antiretroviral therapy (ART). Dolutegravir (DTG) is a common HIV medicine in Uganda because it works well and has fewer side effects than older treatments. However, some people taking DTG have been found to gain weight and develop liver problems. The liver plays an important role in keeping the body healthy, so any damage can affect long-term wellbeing. Detecting liver problems early is especially important in Uganda, where regular blood tests may not always be available.
In this study, we looked at whether simple body measurements, such as waist size and body mass index (BMI), can help identify people with liver damage. We enrolled 212 adults living with HIV who were taking DTG-based treatment for at least one year at Mbarara Municipal Health Centre IV. We measured their height, weight, and waist and hip size, and we tested their blood for liver enzymes called ALT and AST; markers of liver injury.
We found that about 13 in every 100 participants had elevated liver enzymes, meaning possible liver damage. Those with liver problems tended to have more fat around their waist. A measurement called the waist-circumference-to-BMI ratio (WC/BMI ratio) was strongly linked to elevated liver enzymes. People with a higher WC/BMI ratio were nearly four times more likely to have liver damage.
Our findings suggest that a quick, low-cost measurement like WC/BMI ratio could help health workers identify HIV patients at risk of liver disease especially in clinics with limited access to laboratory testing. Routine monitoring of weight and waist size may help protect the long-term health of people taking DTG.
Introduction
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) remains a significant global health burden, affecting approximately 39 million people worldwide. 1 In Uganda, where HIV prevalence is high, Dolutegravir (DTG)-based antiretroviral therapy (ART) has been widely adopted to enhance treatment outcomes due to its high genetic barrier to resistance and favorable safety profile. 2 However, emerging evidence suggests a growing prevalence of metabolic complications among people living with human immunodeficiency virus (PLWH) on DTG, including abnormal obesity indices and elevated serum transaminases, which are critical markers of liver injury.3,4 This raises concerns about the potential impact of DTG-based ART on liver function, 5 especially in resource-limited settings like Uganda, where routine monitoring may be inadequate.
Despite the widespread rollout of DTG-based ART, there is a paucity of localized studies examining its effects on liver function, particularly the prevalence of elevated serum transaminases and associated risk factors. Existing data from other regions suggest that metabolic syndrome components, such as central obesity, dyslipidaemia, and insulin resistance, are common among patients on DTG and may predispose them to liver damage.3,6 However, the extent to which these metabolic changes influence liver function in Ugandan populations remains poorly understood. This gap in knowledge limits the ability to develop targeted interventions to prevent liver complications and optimize HIV treatment outcomes 7 in such setting.
Emerging evidence highlights a potential link between obesity indices and liver enzyme abnormalities. Central obesity, commonly measured by waist circumference (WC) and body mass index (BMI), is a known predictor of metabolic syndrome and has been associated with liver dysfunction, including non-alcoholic fatty liver disease and elevated transaminases. 4 Given that DTG is associated with weight gain and changes in fat distribution, 3 it is plausible that obesity indices may serve as key predictors of liver enzyme elevation in patients on DTG-based ART. However, data specific to Uganda are lacking, emphasizing the need to explore these associations in local HIV populations to inform treatment strategies. 7 This study aimed to investigate the association between obesity indices (BMI, waist-to-hip ratio (WHR), waist-to-height ratio, WC, and WC/BMI ratio) and elevated serum transaminases among patients receiving DTG-based ART at Mbarara Municipal Health Centre IV, Uganda.
Materials and Methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies. 8
Study Design, Setting, Population, Eligibility Criteria, and Sampling Procedure
This study was a descriptive and analytical cross-sectional study conducted among PLWH who had received DTG-based ART for a period of at least 1 year at Mbarara Municipal Health Centre IV ART clinic, located in South Western Uganda, Kamukuzi division, Mbarara City along Mbarara - Kabale road. The facility serves neighboring districts such as Kiruhura, Ibanda, Rwampara, Sheema, Isingiro, and populations within the city. The study included male and female patients aged 18 years and above who had been on DTG-based ART for at least 12 months and had provided written informed consent. Patients with missing medical records, pregnant or lactating women, those with interrupted treatment, and individuals attending the clinic for acute illness were excluded. Participants with a documented diagnosis of hepatitis B and/or hepatitis C were also excluded from the study. Study participants were selected through systematic sampling from adult HIV patients on DTG-based ART attending the clinic.
Sample Size Determination
The Keish Leslie formula of 1965 was used to determine the minimum required sample size using the following assumptions: 5% precision and a 95% confidence interval (CIs), the Z-statistic of 1.96, and 16.16% proportion of PLWH on efavirenz based regimen with elevated serum alanine transaminases (ALT) in India.
9

where n is required sample size,
Z is Z-statistic for a level of confidence, P is expected prevalence, and D is precision.

Therefore, the minimum sample size of 208 study participants was required in this study.
Study Variables
The primary dependent variable in this study was elevated serum transaminase levels. The independent variables were grouped into three categories: socio-demographic factors, clinical factors, and HIV and/or ART-related factors. Socio-demographic factors included age, sex, education level, religion, employment status, and marital status. Clinical factors comprised hypertension, family history of hypertension, family history of diabetes mellitus, overweight, obesity, WC, waist-to-height ratio, WHR, WC/BMI ratio, smoking status, alcohol consumption, and physical activity. HIV and/or ART-related factors included duration of HIV infection, duration on DTG-based ART, and viral load. ALT levels were considered elevated if >45 U/L in males and >34 U/L in females, 10 while aspartate transaminase (AST) was classified as high when >35 U/L in males and >31 U/L in females. 10 Hypertension was defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg. 11 BMI was categorized as normal weight (≤ 24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (≥30 kg/m2). 12 Waist-to-height ratio was deemed abnormal if ≥0.5, while WC cut-offs were >80 cm for females and >94 cm for males. 13 Additionally, WHR was considered abnormal if ≥0.85 for females and ≥0.9 for males.13,14
Data Collection
Data collection was conducted from March 15, 2024, to May 18, 2024. Participants who provided informed consent were interviewed by trained research investigators using a structured questionnaire to obtain information on socio-demographic, clinical, and HIV/ART-related factors. This procedure was repeated until the required sample size was achieved. Anthropometric measurements, including height and weight for calculating BMI, and waist and hip circumferences for determining WHR, were obtained by a clinician. Blood pressure was measured using a digital sphygmomanometer, with two readings taken at 5-minute intervals, and the mean value recorded as the participant's blood pressure. Participants’ weight and height were measured using a portable weighing and height scale. Waist and hip circumferences were assessed using a non-stretchable ergonomic circumference measuring tape. Two measurements were taken for each parameter, and a third measurement was obtained if the difference between the first two readings exceeded 3 cm. The mean of the two or three readings was then recorded as the final waist or hip circumference.
A 4 mL venous blood sample was collected from each participant using red-top Vacutainer tubes. Serum was separated within 1 hour of collection by centrifugation at 1000 rpm for 5 min using a centrifuge with a 10 cm radius, and subsequently stored at 2-8 °C until analysis at the end of each day. Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were determined by the spectrophotometric method using a clinical chemistry analyzer at Mbarara Municipal Health Centre IV, Mbarara City. The analyzer performed automatic incubation, photometric measurements, and calculations at specific wavelengths using designated reagents. Calibration was conducted using AutoCal, and both normal and pathological quality control samples were analyzed daily prior to running the study samples. All procedures adhered strictly to the manufacturer's instructions for both the analyzer and reagents.
Statistical Analysis
The research investigators double entered the collected data into Microsoft excel at the end of each study day. At the end of data collection, the research data was exported to STATA version 17 Software for analysis. The research investigators compared all studied variables by the primary outcome variable (elevated serum transaminases) at a univariate level to test statistical difference between the two groups.
Categorical variables were summarized using frequencies and proportions, and then a Chi square test or Fischer's exact test was used to compare their distribution between the two groups of the outcome variable. A P-value < 0.05 value was considered to be statistically significant. Continuous variables were tested for normality using Shapiro-wilk normality test and were all not normally distributed (P-value <0.05). These were all summarized using median with interquartile range (IQR) and a non-parametric test, ie, Wilcoxon rank-sum test was used to compare their medians between participants with elevated serum transaminases and those with normal serum transaminases. A P-value was obtained and a P-value < 0.05 was considered statistically significant.
The proportion of patients with elevated levels of serum transaminases together with its 95% CIs was determined by dividing the total number of patients with elevated serum transaminases by the total number of study participants recruited and will be expressed as percentage. The studied factors were assessed using logistic regression model. Elevated serum transaminases were the binary dependent variable (1 = High, 0 = Normal). All independent variables, at bivariate level, was compared with high serum transaminase levels (serum transaminase levels that are dichotomized into high and normal levels). The associations were measured using odds ratios together with their 95% CIs, and the statistically significant odds ratios were indicated by a P-value less than 0.2 at the bivariate level. The variables that were clinically and/or statistically significant at this level were also assessed in the multivariable model to adjust for confounding effects. The final model's goodness of fit was assessed using the Hosmer-Lemeshow test, with a P-value >0.05 indicating a good fit (P = 0.5316 in our final model). The final multivariable model was also assessed for multicollinearity. The variance inflation factor was 1.84, which is well below the commonly accepted threshold of 5, indicating no evidence of severe multicollinearity among the included covariates. In the final multivariable model, associations were considered significant at a P-value ≤0.05.
To evaluate the predictive ability of the WC/BMI ratio for identifying participants with elevated serum transaminases, we conducted a receiver operating characteristic (ROC) curve analysis. ROC analysis was selected because it is an established method for evaluating the diagnostic or discriminative performance of a continuous biomarker in classifying a binary outcome. The area under the curve (AUC) was computed to quantify the overall discriminative performance of the WC/BMI ratio. An AUC value closer to 1.0 indicates better predictive power, whereas an AUC of 0.5 suggests no better classification than chance. Predictive performance was considered statistically significant if the 95% CI for the AUC did not include the null value of 0.5. Additionally, the interpretation of AUC values is summarized as: AUC 0.90-1.00 = Excellent; 0.80-0.89 = Good; 0.70-0.79 = Fair; 0.60-0.69 = Poor; 0.50-0.59 = Failure. 15
Results
Study Flow Chart
Narrative of the Study Flow Chart
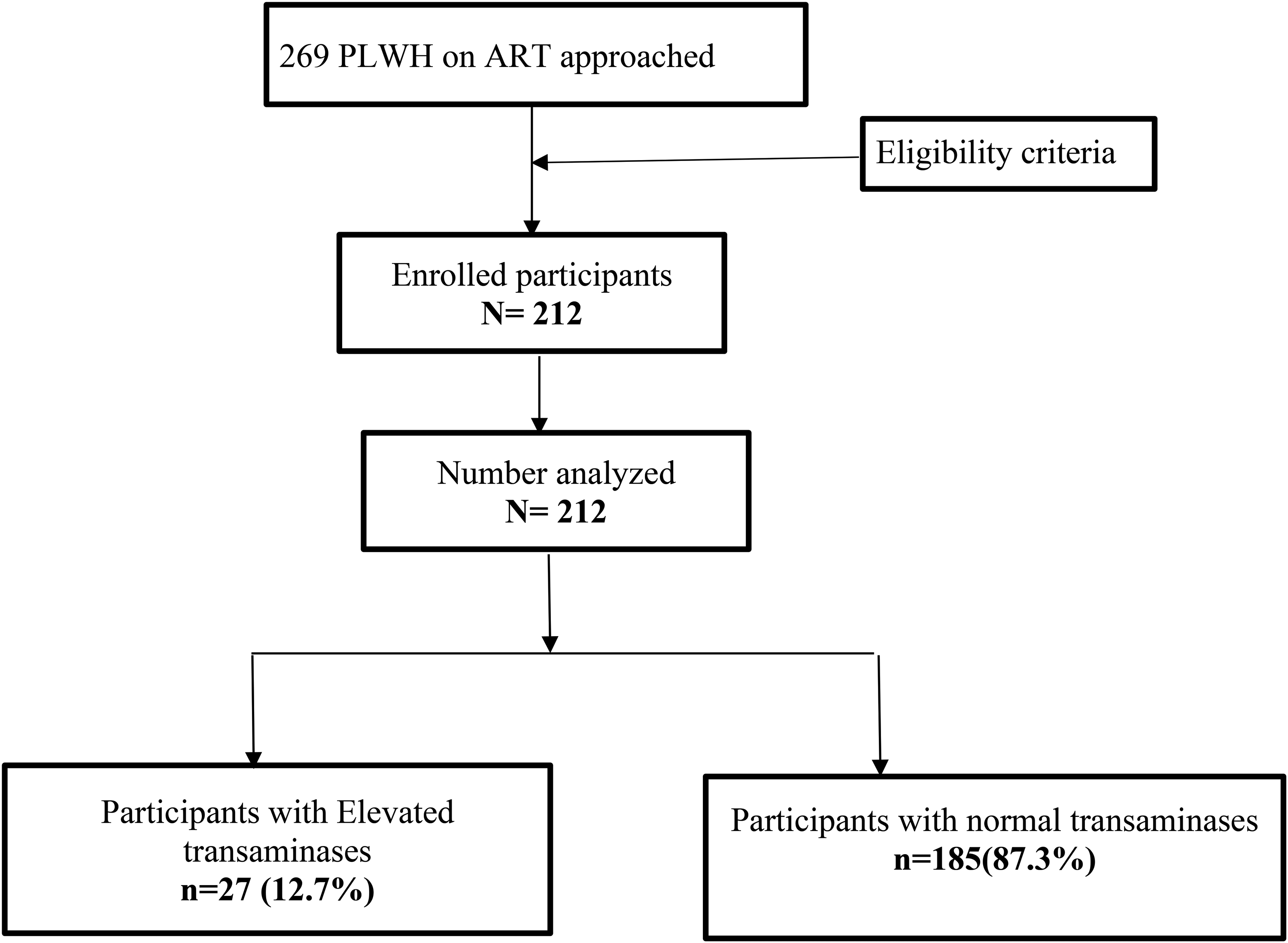
A total of 269 PLHIV on ART were initially approached for study participation. After applying the eligibility criteria, 212 participants were enrolled. All 212 participants were included in the final analysis. Among these, 27 participants (12.74%) had elevated serum transaminases, while 185 participants (87.26%) had normal levels of serum transaminases.
Characteristics of Study Participants
A total of 212 participants were included in the study (Table 1), of whom 25% were male and 75% female, with a median age of 39 years (IQR: 33-49). Most participants were married or cohabiting (60.4%), while 12.7% were single and 26.9% were separated or divorced. Regarding education, over half (50.9%) had completed primary education as highest level of education, 30.7% had secondary, 9% had tertiary education, and 9.4% had no formal education. The majority were Protestants (52.8%), followed by Catholics (38.2%) and Muslims (9%). Most participants were employed (84.4%) and resided in rural areas (59%). Concerning lifestyle characteristics, 91% were non-smokers, 5.7% had ever smoked, and 3.3% were active smokers, while 69.3% reported no alcohol consumption, 27.4% were current drinkers, and 3.3% were former drinkers. Physical inactivity was common, reported by 64.2% of participants. Viral load was undetectable in 74.1% of respondents, whereas 25.9% had detectable levels. We did not observe significant differences in the distribution of participant characteristics between those who had elevated serum transaminases and those who had normal serum transaminase levels (P-value >0.05) with the exception of WHR and WC/BMI ratio.
Characteristics of Study Participants Stratified by Serum Transaminase Status.
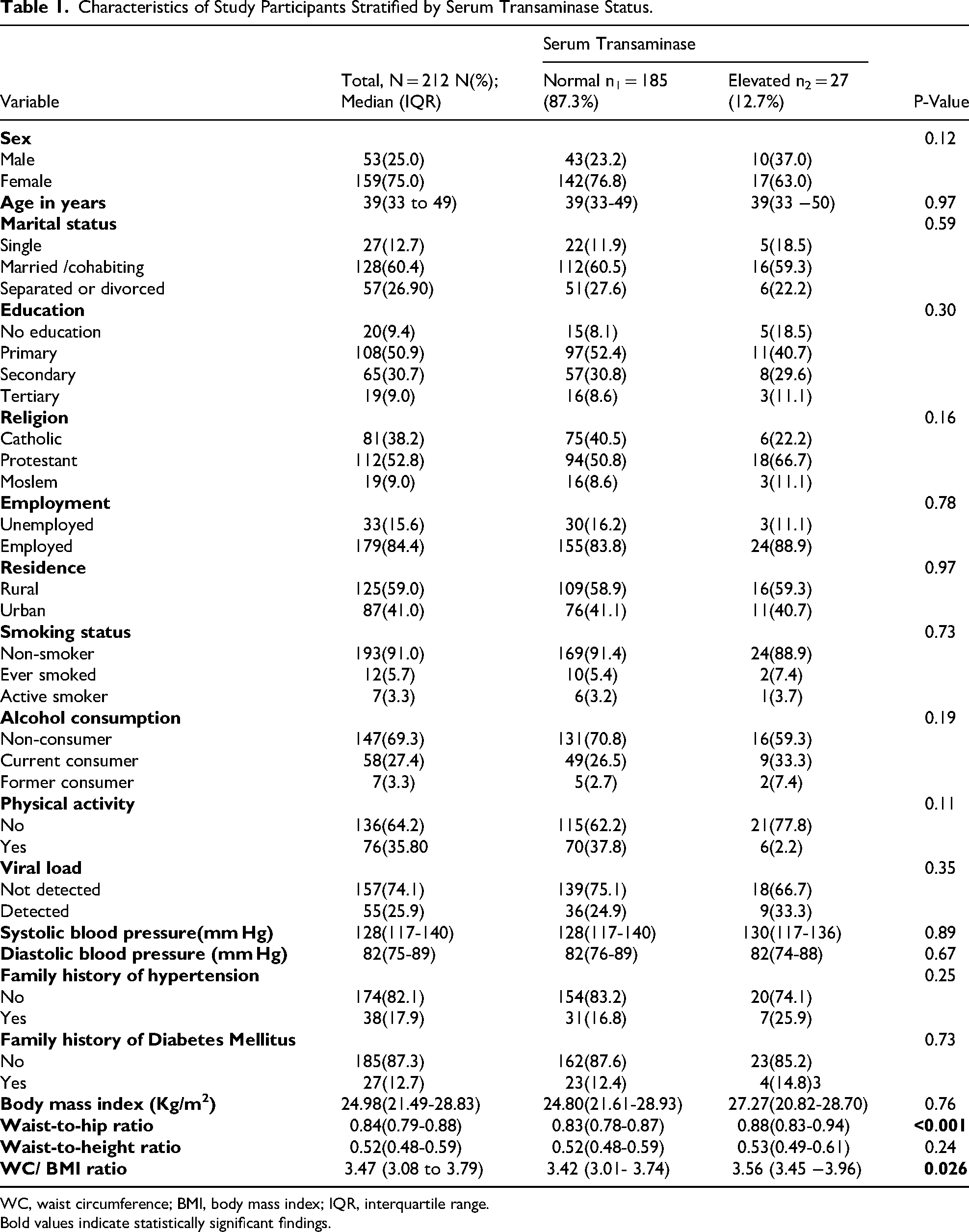
WC, waist circumference; BMI, body mass index; IQR, interquartile range.
Bold values indicate statistically significant findings.
Prevalence of Elevated Serum Transaminases
Out of the 212 study participants that were recruited in this study, 27 had elevated serum transaminases giving an overall prevalence of 12.7% with a 95% CI of 8.9% - 18.0% as indicated in Figure 1. The prevalence of elevated alanine aminotransferase was 8.5% (18 out of 212) with a 95% CI of 5.4-13.1% while the prevalence of elevated aspartate aminotransferase was 7.1%(15 out of 212) with a 95% CI of 4.3-11.4%.

Prevalence of elevated serum transaminases.
Association Between Obesity Indices and Elevated Serum Transaminases
Participants with elevated transaminases had a significantly higher median WHR [0.88 (IQR: 0.83-0.94)] compared to those with normal transaminases [0.83 (IQR: 0.78-0.87)] (P < 0.001). WC/BMI ratio was also significantly higher among those with elevated transaminases [3.56 (IQR: 3.45-3.96)] compared to those with normal transaminases [3.42 (IQR: 3.01-3.74)] (P = 0.026) as indicated in Table 1.
After adjustment for confounders at multivariate analysis, only WC/BMI ratio was significantly associated with elevated serum transaminases with aOR: 3.68, CI (1.11-12.16), with a P-value of 0.033 as shown in Table 2. At an optimum cut-off point of 3.45 with a sensitivity of 78% and specificity of 52%, WC/BMI ratio was observed to have a significant power; AUC=0.651(95%CI: 0.580 0.722) to distinguish between participants with and without elevated serum transaminases as indicated in Figure 2.

Receiver operating curve showing predictive performance of WC/BMI ratio for elevated serum transaminases. WC, waist circumference; BMI, body mass index.
Factors Associated with Elevated Serum Transaminases.

P-value<0.05 indicates statistical significance; aOR, adjusted odds ratio; cOR, crude odds ratio. WC, waist circumference; BMI, body mass index; CI, confidence interval.
Discussion
The prevalence of elevated serum transaminases in this study was 12.7% (95% CI: 8.9-18.0) among PLWH on DTG-based therapy. This finding aligns with global studies reporting prevalence rates between 10% and 25% among HIV patients on ART, with higher rates observed in populations with concurrent metabolic disorders.16,17 In Sub-Saharan Africa, reported prevalence rates range from 8% to 15%, consistent with our findings. 16 The prevalence of elevated serum transaminases among patients on DTG-based ART in our study is notably higher compared to a similar study conducted at the Immunosuppression Syndrome Clinic of Mbarara Regional Referral Hospital, Uganda, where 9 out of 124 (7.3%) patients on DTG-based ART exhibited hepatotoxicity. 2 This discrepancy may be attributed to differences in study criteria; our study included patients who had been on DTG for at least 1 year, whereas the aforementioned study had patients on DTG for as little as 3 months. Consequently, our study's longer duration of exposure may account for the observed higher prevalence of elevated serum transaminases, suggesting a stronger association between DTG-based ART and hepatic enzyme elevation. In contrast, a study in Uganda found an overall prevalence of elevated serum transaminases at 18.8% (95% CI: 16.8-21.1), including 17.9% of patients on DTG-based ART, which aligns with the prevalence observed in our study. 16 Our prevalence was markedly higher than the 4.8% reported in an Ethiopian study of patients on Tenofovir Disoproxil Fumarate-based ART, 18 indicating that DTG may be more hepatotoxic compared to Tenofovir Disoproxil Fumarate. Additionally, our study's prevalence was lower than the 37% reported in a study conducted in the North Western region of Cameroon among patients on various ART regimens, including Tenofovir/Lamivudine/Efavirenz and Zidovudine/Lamivudine/Nevirapine. 19 This suggests a potentially stronger association between hepatotoxicity and the ART regimens used in the Cameroon study compared to DTG-based ART. Conversely, a prospective study in Ethiopia, which did not focus exclusively on DTG, reported a prevalence of elevated serum transaminases at 22.8% (72 out of 316), further supporting that DTG-based ART may exhibit a lower hepatotoxicity profile relative to other ART regimens.
Our study identified a significant association between the WC/BMI ratio and elevated serum transaminases (adjusted odds ratio [aOR] = 3.68, 95% CI: 1.11-12.16, P = 0.033). This suggests that individuals with a higher WC/BMI ratio are approximately 3.7 times more likely to exhibit elevated transaminases, highlighting the role of central obesity in hepatocellular dysfunction. Clinically, this finding is crucial, as it positions the WC/BMI ratio as a potential accessible, cost-effective marker for identifying patients at risk of liver damage in resource-limited settings. Globally, studies have established a link between obesity indices and liver dysfunction.16,18–20 In Sub-Saharan Africa, similar associations have been documented, though studies are fewer. 19 East African data, including Ugandan studies, have shown a positive but weaker correlation between general obesity markers and liver damage, potentially due to differences in dietary patterns and genetic predispositions.
The WC/BMI ratio demonstrated a significant predictive capacity for elevated serum transaminases, with an AUC of 0.651 (95% CI: 0.580-0.722) at an optimal cut-off of 3.45, achieving a sensitivity of 78% and specificity of 52%. This moderate predictive performance indicates that the WC/BMI ratio is a potential useful, though not definitive, tool for identifying patients at risk of hepatocellular damage. Clinically, its high sensitivity makes it valuable for screening purposes, particularly in settings with limited access to advanced diagnostic tools. However, the observed low specificity at the optimal cut-off of WC/BMI may lead to many false positives in screening limiting its potential utility as a standalone clinical screening threshold. Globally, similar obesity indices, such as the WHR, have been validated as predictors of liver dysfunction.21–23 Ugandan research remains limited in this area, though studies have emphasized the importance of anthropometric markers in assessing metabolic health in PLWH. Therefore, our findings are hypothesis-generating and provide a novel, foundation and context-specific evidence for future longitudinal studies with larger sample sizes and enhanced statistical power to mechanistically evaluate the association of WC/BMI ratio and other obesity indices for elevated serum transaminases among PLWH on DTG-based ART.
Conclusion
This study demonstrates that obesity indices, particularly the WC/BMI ratio, are significant predictors of elevated liver enzymes among HIV patients on DTG-based ART. The findings highlight the association between central obesity and hepatocellular dysfunction, emphasizing the metabolic impact of DTG-based therapy. These results underscore the need for routine liver function monitoring and metabolic risk assessment in patients receiving this regimen to optimize care and prevent liver-related complications in this vulnerable population.
Study Limitations and Recommendations
This study has some limitations that should be considered when interpreting the findings. First, the cross-sectional design precludes the establishment of causal or temporal relationships between the WC/BMI ratio and elevated serum transaminase levels. Consequently, the observed associations should be interpreted as correlational, and longitudinal studies are required to determine directionality and causality.
Second, liver injury was assessed solely using elevated serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels, without confirmatory imaging or histological evaluation. As such, the outcome reflects biochemical evidence of hepatic injury or stress rather than definitive structural liver disease, and misclassification of specific hepatic conditions cannot be excluded.
Third, although participants with documented hepatitis B and/or hepatitis C infection were excluded to minimize confounding from viral hepatitis, information on other important potential confounders was limited. These included the use of non-antiretroviral hepatotoxic medications, precise quantification of alcohol intake, and detailed histories of prior ART exposure. Therefore, residual confounding from unmeasured or incompletely measured factors may persist.
Fourth, lifestyle behaviors such as smoking, alcohol consumption, and physical activity were self-reported and are thus susceptible to recall and social desirability biases, which may have resulted in exposure misclassification.
Fifth, the study was conducted at a single ART clinic in South Western Uganda, which may limit the generalizability of the findings to other regions or populations with different genetic backgrounds, dietary habits, lifestyle patterns, or healthcare access. Although the clinic serves a large and heterogeneous catchment population encompassing both rural and semi-urban communities, findings may not fully represent all PLWH receiving DTG-based ART across Uganda. Additionally, while systematic sampling was employed to reduce selection bias and ensure feasibility within routine clinical care, sampling from a single facility may not fully capture national variability.
Despite these limitations, the study provides important preliminary and context-specific evidence on the association between the WC/BMI ratio and elevated serum transaminases among PLWH on DTG-based ART in a resource-limited, rural sub-Saharan African setting, where such data remain scarce.
In light of the above limitations, future and more powerful studies on the association of WC/BMI ratio and other obesity indices with elevated serum transaminases should employ multi-center and population-based designs to enhance generalizability and statistical power. Longitudinal approaches are needed to establish temporal and causal relationships between anthropometric indices and liver enzyme abnormalities. Incorporation of imaging modalities, objective measurements of lifestyle behaviors, comprehensive assessment of hepatotoxic exposures, and detailed ART histories will be essential to better characterize liver disease and elucidate underlying biological mechanisms in this population.
Footnotes
Abbreviations
Acknowledgements
We extend our heartfelt gratitude to the study participants, as well as the dedicated clinicians, laboratory personnel, and ART clinic staff at Mbarara Municipal Health Centre IV. Their unwavering support and collaboration were invaluable throughout the duration of this study.
Ethical Approval and Informed Consent
The Mbarara University of Science and Technology Faculty Research Committee (FRC) granted ethical approval for this study under approval number MUST/MLS/030. Prior to performing the study, administrative clearance was also acquired from Office of the City Clerk, Mbarara City. Prior to their participation in the study, each participant provided informed written consent. The 1975 Declaration of Helsinki's ethical criteria (1964) were followed in this study protocol. Each study participant was assigned a code that could not be linked to them in order to maintain participant confidentiality. Additionally, participants were made aware that their involvement in the study was completely voluntary and free, and they could leave at any moment.
Authors Contributions
CNB, PK, HM, MKM, CK, IN, AA, and SPR participated in conceptualization of the study and data collection. CNB did data analysis. CNB, PK, HM, CN, MKM, CK, IN, AA, J.T, MJM, ES, LA, VM, DT, and SPR contributed to writing the first draft of the manuscript with VM, SPR, and DT providing critical revisions. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The dataset used and or analyzed during the current study are available from the corresponding author upon reasonable request.