
Abstract
Background
Following its approval by the US Food and Drug Administration in January 2021, clinics have moved to implement the first long-acting antiretroviral regimen (cabotegravir [CAB] and rilpivirine [RPV]) into routine care.
Methods
In this qualitative implementation study, we characterize health worker experiences with the introduction of CAB/RPV into a safety net HIV clinic in the Southeastern US during the first 10 months of service integration. Interviews were analyzed using directed content analysis and results were synthesized using the updated Consolidated Framework for Implementation Research.
Results
Health workers described both successes and challenges. Successes included strong awareness of and enthusiasm for CAB/RPV and the integration of supportive resources over time. Challenges included inconsistent communication about logistics, perceived pressures on human resources, and concerns about structural barriers affecting patient access to care.
Conclusions
Findings highlight the resource demands of implementing CAB/RPV, and the complex array of factors that shape successful implementation.
Introduction
Effective antiretroviral therapy (ART) treatment for persons with HIV interrupts HIV transmission and reduces AIDS-related mortality.1–4 Historically, ART typically included daily oral medications, but recent advances have extended the dosing interval through innovations in longer-acting therapies, including long-acting injectable ART (LAI-ART). These agents offer a compelling alternative to daily oral ART.5,6 The first completely long-acting regimen (cabotegravir [CAB] and rilpivirine [RPV]) was approved by the US Food and Drug Administration (FDA) in January 2021 for use among people with HIV who are virally suppressed. 7 Phase III studies have demonstrated that these combination injections are safe and non-inferior to standard oral therapy for maintaining HIV viral suppression when dosed every 4 or every 8 weeks.8–12
Although CAB/RPV is more widely available in the US, a transition to every-two-month in-clinic injections presents a significant shift in visit burden for both patients and health systems. Early scholarship examining the integration of CAB/RPV into clinics in the US suggests health workers perceive this treatment modality to be acceptable and appropriate, but identify potential barriers to implementation.13–15 At least two cluster implementation trials, one in the US and another in Europe, have tested strategies to support facilities and providers in the roll-out of CAB/RPV.16,17 Both studies observed an overall decrease in implementation concerns during the follow-up periods, though persistent barriers remained through the end of the trials.16,17
Most clinics have navigated CAB/RPV integration without the training and support from structured studies. As a result, clinics have adjusted or adapted their procedures, staffing models, and patient selection to reflect local constraints and priorities. Lessons learned from these processes provide important insight into how clinics may prepare as innovations in long-acting injectable treatments evolve both within infectious disease praxis and beyond.6,18 In this qualitative implementation study, we use in-person interviews to characterize health worker experiences with the introduction of CAB/RPV into a safety net HIV clinic in the Southeastern US during the first 10 months of service integration.
Methods
Study Design and Setting
This qualitative study was embedded within a broader mixed-methods study of barriers and facilitators to LAI-ART implementation. The study was conducted at the University of North Carolina Infectious Disease (UNC ID) clinic. UNC ID is a safety net clinic that engages around 2000 patients with HIV annually. The clinic is supported by Ryan White funding and is actively engaged in multiple research studies, including as a site for early-phase efficacy trials of CAB/RPV. The first non-trial patient received CAB/RPV in August 2022. In the first year of CAB/RPV implementation, 47 patients with HIV initiated CAB/RPV. Among these patients, the median age was 44 years, 76.6% were male, and 53.2% were non-Hispanic Black. 19
Recruitment and Data Collection
We purposively recruited health workers involved in the early design and implementation of CAB/RPV programming at UNC ID. Sampling focused on capturing a range of experiences among key stakeholders. 20 To be eligible for participation, health workers needed to be 18 years of age, an employee of UNC ID, and involved, even peripherally, in LAI-ART integration or patient management. This included but was not limited to: LAI-ART prescribers (medical doctors, nurse practitioners, physician assistants), social workers, benefits counselors, nurses, medical assistants, pharmacists, pharmacy technologists, and front-desk staff. Those not meeting these criteria were ineligible for participation. All participants provided written informed consent prior to study initiation and were offered $50 for their participation; this incentive was considered minimal and unlikely to introduce bias. Semi-structured interviews were conducted between February and October 2022, preceding and following the first non-trial patient receiving LAI-ART. The decision to cease recruitment was made in collaboration with the researcher collecting the data; recruitment was stopped when data saturation had been achieved. 21 Participating health workers were asked about their experiences with or perceptions of offering CAB/RPV as a treatment option for their patients, as well as any perceived challenges or opportunities in incorporating or expanding access to CAB/RPV in the clinic. All interviews were conducted in English, audio-recorded, and transcribed with identifying information removed.
Data Analysis
We used directed content analysis to analyze the interview transcripts. 22 The codebook was designed to align with Proctor et al.'s taxonomy of implementation outcomes, which defines the constructs of acceptability, adoption, appropriateness, cost, feasibility, fidelity, penetration, and sustainability. 23 Two authors independently piloted the codes and code definitions. The same two authors coded all interview transcripts and resolved any discrepancies through discussion, bringing in a third author as necessary. All coding was completed in ATLAS.ti V.23.
Results synthesis was guided by iterative discussion of emergent themes and organized according to the updated Consolidated Framework for Implementation Research (CFIR). 24 The CFIR is a determinants framework comprised of five domains (innovation, outer setting, inner setting, implementation process, and individual characteristics) and 48 intersecting constructs (Figure 1). 24 Within each domain, key ideas were thematically summarized to characterize health worker experiences implementing CAB/RPV. As interviews occurred both prior to and following the first non-trial patient receiving LAI-ART at UNC ID, salient differences in stakeholder responses between these two periods were noted in the synthesis process; results were not formally stratified by implementation phase.

The updated Consolidated Framework for Implementation Research, adapted from Damschroder et al. (2022), the Center for Implementation Research, and Rutstein et al. (2025).24–26 This figure visualizes the updated Consolidated Framework for Implementation Research and highlights key constructs described by the participants in this study. The outer setting, inner setting, and individual characteristics are placed in concentric circles. These are linked to the innovation (i.e., CAB/RPV) by implementation processes.
Ethics
This study was approved by the UNC Chapel Hill Institutional Review Board (21-2517).
Results
Interviews were conducted with 15 health workers involved in the implementation of CAB/RPV between February and October 2022. Interviewees represented diverse roles within UNC ID; we interviewed eight medical doctors, two advanced practice practitioners, one nurse, and one stakeholder from each of social work, pharmacy, finance, and clinic administration. Alongside interviews, multiple implementation activities took place at UNC ID both leading up to and following the first non-trial patient receiving LAI-ART in August 2022. Prior to the first patient, UNC ID held a CAB/RPV process mapping workshop; assembled a multidisciplinary, CAB/RPV-specific team; developed a clinic-level standard operating procedures (SOP); created electronic medical record (EMR) “dot phrases” for CAB/RPV initiation; and hired a dedicated nurse coordinator to oversee the LAI-ART program. Following the first patient, a second process mapping workshop was held. Figure 2 illustrates the timing of these implementation activities relative to the timing of the interviews conducted.

Timeline of initial implementation activities and key informant interviews, from January to October 2022. This figure visualizes the month(s) in which initial implementation activities, process mapping workshops, and key informant interviews took place. Leading up to the first non-trial initiation of CAB/RPV in August 2022, UNC ID conducted a process mapping workshop in January; assembled a multidisciplinary, CAB/RPV-specific team in February; developed a clinic-level standard operating procedures (SOP) in March; activated electronic medical record “dot phrases” for CAB/RPV initiation in June; and hired a dedicated nurse coordinator to oversee the LAI-ART program in July. A second process mapping workshop was conducted in late August following the first non-trial patient receiving CAB/RPV. Health workers were interviewed throughout this period, with most being interviewed in the first and third quarters of 2022.
Innovation
Evidence Base
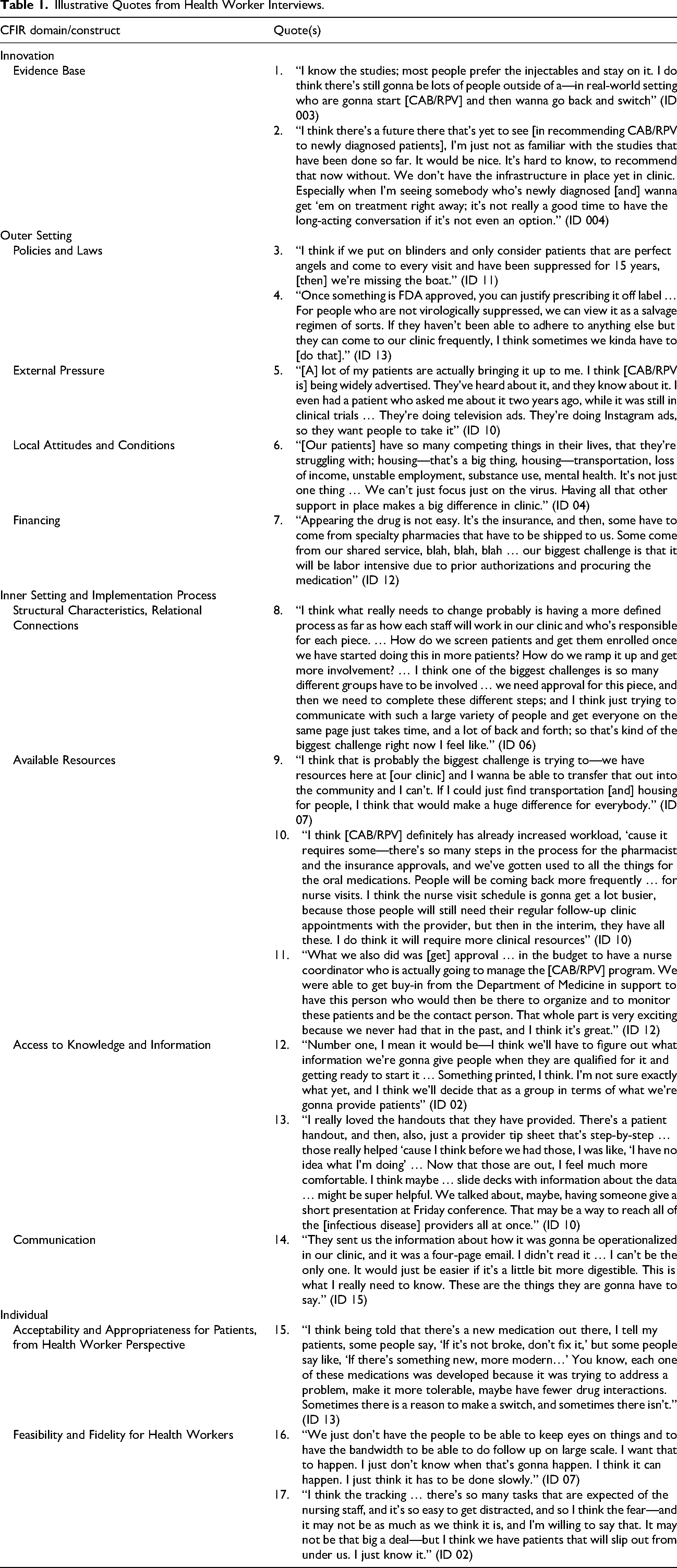
When reflecting on CAB/RPV itself, a few health workers described evidence gaps at the time of their interviews and explained how this would affect CAB/RPV in clinical practice. Some expressed uncertainties regarding the translation of trial evidence into real-world settings, where circumstances such as missed appointments, or the desire to switch back to oral therapy, may be more common among patients (Table 1, Quote 1). Others expressed apprehension about using CAB/RPV in hypothetical scenarios where they were working with patients who were newly diagnosed with HIV and not virally suppressed (Table 1, Quote 2).
Illustrative Quotes from Health Worker Interviews.
Relative Advantage
Despite these concerns, there was general excitement about the potential of CAB/RPV to reduce the burden daily oral ART can place on patients, especially in the context of treating a highly stigmatized disease like HIV. Some of this excitement came from trial evidence demonstrating CAB/RPV is a non-inferior option to standard care (oral ART) and could offer a relative advantage for patients who prefer a more discrete, longer acting medicine. At the same time, health workers acknowledged that CAB/RPV is a fundamentally different type of treatment option; as such, the choice to initiate CAB/RPV would ultimately be shaped by their patients’ preferences and perceptions of its acceptability and feasibility.
Outer Setting
Policies and Laws
When discussing patient eligibility and prescribing practices for CAB/RPV, several health workers referred to federal agencies like the FDA which regulate the approval, use, and safety of medications in the US. In discussing these agencies, stakeholders expressed concern about CAB/RPV eligibility. At the time of their interviews, CAB/RPV was only approved for virally suppressed patients. Health workers described how this focus on viral suppression may mean excluding patients who struggle with adherence—a group that many believed would benefit most from a longer-acting treatment alternative (Table 1, Quote 3). Two health workers described the need to create clinic-specific guidance that speaks to the preferences and needs of the patients served (Table 1, Quote 4).
External pressure
Several observed that patients were generally aware of CAB/RPV by way of radio and television commercials, reflecting some of the early marketing for this new treatment alternative (Table 1, Quote 5).
Local Attitudes and Conditions
When asked about barriers to HIV treatment, every interviewee expressed concerns about equitable access to care or support. Nearly all identified structural and environmental factors, such as socioeconomic inequality and distance to clinic, as barriers impacting access to CAB/RPV, and patients’ experience of HIV care more generally (Table 1, Quote 6). Concerns around access to and engagement in care were of particular concern to several stakeholders who viewed the switch to CAB/RPV as a significant commitment given the high frequency of clinic visits required. In describing these barriers, health workers appreciated that for some patients, a high level of engagement in their HIV care is neither feasible nor a priority amid other demands in their lives, such as work or caregiving responsibilities.
Financing
A minority of stakeholders acknowledged that the Ryan White Program provides financial support to the clinic, and one observed that this funding is what made it possible to create and hire additional staff to support CAB/RPV implementation. Multiple health workers described the complexities of navigating payment/insurance systems to procure CAB/RPV, including the challenge of acquiring prior authorizations (Table 1, Quote 7), with one observing that the time spent waiting for approvals can create delays in treatment initiation. Two health workers noted that while the HIV Medication Assistance Program (HMAP) and Ryan White Program support access to HIV care for those without adequate insurance coverage, patients must renew their participation in these programs by resubmitting paperwork on a regular basis, which patients may forget or de-prioritize.
Inner Setting and Implementation Process
Structural Characteristics, Relational Connections
Multiple stakeholders foresaw scheduling complexities and staffing limitations as the most challenging aspects of CAB/RPV implementation. In their reflections, health workers underscored the need for streamlined prescribing and follow-up processes, accompanied by designated support systems to ensure adequate staffing. Several also described the need to create new clinic-level policies and protocols, with one of the earlier interviewees emphasizing the need to finalize the clinic's SOP prior to roll-out. This was seen to be especially important to clarify roles among UNC ID workers and improve coordination between UNC ID and other health system departments (Table 1, Quote 8). A later interview indicated that the tension between unclear roles and staffing was a primary concern in program roll-out and took time to resolve.
Available Resources
Stakeholders noted that existing clinic-level resources at UNC ID, such as social workers, benefits assistance, and transportation programs, help bridge some of the gaps patients face in navigating outer-setting barriers to HIV care, though these resources are finite (Table 1, Quote 9). Regarding human resources, multiple respondents interviewed in the early implementation process, prior to any non-trial patients receiving CAB/RPV, expressed concerns about staffing. Several noted that scale up may not affect staff equally, with most of the work falling to persons usually responsible for getting patients into clinic regularly (e.g., nurses). A few expressed that having dedicated staff for CAB/RPV-specific processes would be helpful, such as nurse navigators or coordinators to handle appointment scheduling, tracking, and patient outreach. It was also recommended to have staff champions available for technical support when challenges arose, such as a point person for specific questions related to changing regimens or navigating insurance approvals. As more non-trial patients received CAB/RPV at the clinic, interviews conducted later in the implementation process confirmed the pressure that scale up placed on existing human resources (Table 1, Quote 10) but also indicated that a dedicated nurse coordinator had been hired to specifically support CAB/RPV implementation (Table 1, Quote 11).
Access to Knowledge and Information
Beyond dedicated personnel, some stakeholders emphasized the need for educational materials for both patients and health workers. For example, several expressed a desire for printed materials to hand out to patients as well as resources to help health workers counsel patients on CAB/RPV. Interviews conducted earlier in the implementation process indicated this as a need (Table 1, Quote 12), whereas interviews conducted later in the implementation process indicated these supports had been provided and were helpful (Table 1, Quote 13). One health worker noted that the EMR dot phrase was useful in reminding them what to discuss with patients. When asked whether additional supports would be valuable, some suggested educational sessions, whether through training, videos, or virtual materials, could ensure a greater number of health workers were familiar with CAB/RPV and prepared to answer patient questions.
Communications
Some respondents reported that unclear roles and miscommunications during the roll-out of CAB/RPV were barriers to the initial implementation process. As protocols and procedures were later formalized, one stakeholder emphasized the importance of communicating these more directly to prescribers in an easy-to-digest format (Table 1, Quote 14).
Individual
Adoption and Acceptability Among Health Workers
All but two stakeholders mentioned having conversations with patients about CAB/RPV, and health workers further expressed enthusiasm at the prospect of additional, non-daily ART options. Many felt comfortable talking about CAB/RPV, though a few expressed a desire to feel more familiar with the logistics for prescribing CAB/RPV within the clinic.
Acceptability and Appropriateness for Patients, from Health Worker Perspective
Stakeholders described various approaches to counseling patients about CAB/RPV. Many expressed their patients were excited to have CAB/RPV as an option, and health workers anticipated it could be beneficial for those who no longer want to take a daily pill or desire a simplified treatment regimen. However nearly all concurrently acknowledged that CAB/RPV may not be a good option for everyone depending on a patient's preferences, be that a fear of needles, concern about convenience and frequent visits for injections, or adverse effects (Table 1, Quote 15).
While there was a general deference to patient preference, health workers concurrently highlighted the importance of a patient's environmental and social circumstances in making shared treatment decisions, including access to transportation, housing and job stability, or medication costs. Prescribers noted they would consider possible drug interactions, history of resistance to the pharmaceutical components of CAB/RPV, and other clinical circumstances in which CAB/RPV may not be appropriate or preferred compared to oral ART. For example, while longer-acting forms of ART may be particularly suitable for people who struggle with adherence to daily ART, prescribers expressed concerns about non-adherence to CAB/RPV (i.e., missing injection appointments). A few health workers highlighted the promise of future LAI-ART innovations, where the half-life of the treatment is longer, and patient visit burden is reduced.
Feasibility and Fidelity for Health Workers
With the initial roll-out of CAB/RPV, stakeholders in earlier interviews expressed concerns about its feasibility given limited staffing and the anticipated workload for activities such as scheduling follow-up injections (Table 1, Quote 16). Health workers also expressed concern about the amount of time additional appointments might take, as well as their ability to track and monitor patient attendance. One nursing staff member expressed uncertainty about their ability to sustain patient tracking (Table 1, Quote 17). In later interviews, health worker concerns about feasibility were less focused on staffing and more focused on logistics coordination and streamlining the multi-step process of prescribing, acquiring, and administering CAB/RPV in addition to patient follow-up.
Discussion
These findings underscore the complexity of integrating new interventions like CAB/RPV into clinical practice. UNC ID undertook an intentional process of implementation planning and engaged health workers in various roles in the months leading up to delivering the first dose of CAB/RPV to a non-trial patient. In their reflections on the first 10 months of service integration, health workers described both successes and challenges across all five CFIR domains. Successes included the strong awareness of and enthusiasm for CAB/RPV among health workers, as well as the integration of new resources to support implementation (e.g., hiring a nurse coordinator, developing educational materials for patients and health workers). Challenges included inconsistent communication about implementation logistics and perceived pressures on scarce human resources. These align with those documented by a growing number of studies examining early CAB/RPV implementation in the US, each of which have highlighted the resource demands of implementation and the complexities of coordinating CAB/RPV procurement and administration.14,27–35
Consistent with other studies of CAB/RPV implementation,27,29,30,32,34 challenges related to the inner setting and implementation process CFIR domains were frequently discussed among the health workers interviewed in our study. In rolling out CAB/RPV, the clinic was short staffed, and interviewees early in the implementation process expressed concern about keeping up with the expected administrative demands of implementation. For some, these concerns created apprehensions about how the subsequent roll-out process would proceed. Health workers were particularly worried about the workload of patient tracking and appointment follow-up, which were noted to increase as more patients received CAB/RPV. Interviewees later in the implementation process reflected that additional supports—such as educational materials, the EMR dot phrases, and the hiring of a dedicated nurse coordinator to lead the CAB/RPV program—were helpful and improved their confidence in the implementation process and coordination over time. While additional health information technology strategies such as automated appointment reminders were not discussed at length in our interviews, these types of tools may also be useful in supporting health workers by promoting efficient clinic-level workflows and patient-level engagement.36,37
Separate from tracking and appointment follow-up, multiple implementation studies have highlighted prior authorization processes for CAB/RPV procurement, including appeals in the case of insurance denials, as major challenges that not only incur administrative burdens but also delay treatment initiation.28,30,32–34 These same challenges were observed in our study, where the complexities of navigating health insurance systems, including prior authorizations, were considered barriers to implementation. To lessen these challenges, there have been calls to streamline patient eligibility and prior authorization processes across insurance carriers as policy-level supports.30,33 In our study, some participants suggested that having a dedicated staff member, such as a financial or benefits counselor, could also be a valuable clinic-level resource.
Implementation of LAI-ART shifts responsibility for ART adherence away from individual patients and towards health systems, 29 which can carry significant financial and operational implications, especially for clinics that function on limited resources. For example, to address the challenges mentioned above, CAB/RPV may require clinics to establish specific clinic flows, create multidisciplinary teams, hire new staff, or reconfigure health worker roles and responsibilities, should that infrastructure not already exist within the scope of their service.27–29,32,34 For safety net clinics like UNC ID that are supported by the Ryan White Program, such resource demands can be particularly difficult to meet.33–35 One national survey of HIV care providers found that those working in Ryan White clinics and in states that have not expanded Medicaid were up to three times as likely to report staffing challenges with LAI-ART roll-out. 33 The study's recommendation to expand Ryan White funding to support staffing and administration was affirmed by our findings, as the Ryan White Program enabled UNC ID to hire necessary staffing support. However, under the current US Administration, continued federal support for this and other HIV treatment and prevention programming remains very uncertain.38,39
Such concerns about clinic resources and responsibilities reflect an ongoing tension between inner and outer setting characteristics within the CFIR model, as the broader social and political landscape generates downstream impacts that not only shape the capabilities of clinics in implementing innovations like CAB/RPV, but also the accessibility of those interventions to patients. Health workers at UNC ID recognized that while the clinic has strong patient engagement programming, this is often not enough to address the complex socioeconomic needs of their patient population. As a result, stakeholders expressed concern that CAB/RPV may remain out of reach for patients who face structural barriers to care. Notably, multiple health workers observed that particular patient populations face intersectional challenges in accessing HIV care due to their age, rurality, sexual orientation, gender identity, race, and/or socioeconomic status. Such structural inequities are well-documented in the literature and raise a concurrent need to appeal to policymakers and institutions to advance policy-level interventions.33,35,40,41 In a separate analysis of UNC ID patients who were eligible for CAB/RPV during the first year of implementation, those that initiated CAB/RPV were more likely to live closer to the clinic and have a higher median number of care interactions in the last 24 months. 19 In our study, health workers observed a disconnect between the patients for whom CAB/RPV is currently indicated by the FDA (those with viral suppression and regimen stability) and the types of patients’ that may benefit most from longer-acting treatment (those who struggle with adherence, who may not be virally suppressed). These concerns are mirrored in other studies, where health workers emphasize that LAI-ART may be least accessible to those who need it most.27,29,31,32
While the initial FDA guidance aligns with the population from the clinical trials, there is emerging evidence around the use of LAI-ART in people with viremia, as well as populations navigating significant barriers to care. For example, one study demonstrated that viral suppression can be achieved among patients initiating LAI-ART with detectable HIV RNA levels and observed a relatively high frequency (87%) of “on time” visit attendance. 42 However, a separate study offered CAB/RPV to patients facing adverse social determinants of health and found that socioeconomic challenges such as unstable housing were critical factors that ultimately affected the ability to retain patients on a stable LAI-ART regimen. 31
A point that was mentioned but underexplored in our interviews was discussion of insights from other service lines (e.g., psychiatry, oncology, reproductive medicine) that offer analogous types of treatment options to their patients. 43 Shared learnings around implementation processes, particularly from service lines within the same health center, could inform best practices and provide a localized blueprint for implementation. Other studies have recommended sharing protocols between clinics, particularly as more consider offering CAB/RPV. 27 In the absence of national protocols, clinics like UNC ID have had to navigate the creation of protocols independently, highlighting opportunities for improved coordination. One project—the Accelerating Implementation of Multilevel Strategies to Advance Long-Acting Injectable for Underserved Populations (ALAI UP)—is addressing this through the provision of protocol templates and technical assistance, including tools and assistance for navigating CAB/RPV insurance processes, for participating clinics nationwide. 32
As protocols are developed, maintaining flexibility to adapt to evolving circumstances and barriers will be essential for programmatic sustainability. One US implementation trial found that while perceived barriers to CAB/RPV implementation declined with the use of a structured facilitation strategy and multi-component toolkit, implementation concerns persisted through the end of the 12-month follow-up period. 16 This observation mirrors our findings, where we noted that health worker discussion of challenges evolved during the first 10 months of service integration, particularly as programmatic leadership iteratively responded to identified needs. As more patients initiate CAB/RPV, the need for additional resources, or a reconfiguration of what already exists, may also increase. This need for adaptability further falls against a changing innovation backdrop, as clinics ready themselves for newer innovations in HIV treatment in the years ahead.
Limitations
While our results provide insight into CAB/RPV implementation, several factors should be considered when interpreting our findings. First, to maximize the efficiency of the research and relevance of the observations, our sampling approach sought to identify individuals who were readily available and most proximal to CAB/RPV integration. 20 However, the resulting sample is small and largely comprised of medical doctors at UNC ID; as a result, our findings are primarily unique to this stakeholder group and may not reflect the full breadth and depth of the implementation process. 20 In addition, this study conducted interviews with health workers both prior to and following the first non-trial patient receiving CAB/RPV at UNC ID. While these observations provide some understanding of how the implementation process evolved over time, including clinic-level planning and real-time problem solving, participants were only interviewed once, meaning that their insights could only be considered cross-sectionally. Finally, our findings are specific to UNC ID, which is a Ryan White-funded clinic affiliated with a large academic center in the southeastern US. Additional research that examines the implementation of CAB/RPV in other types of clinic settings would be valuable, as the challenges and opportunities faced are likely unique from our setting.
Conclusions
This study highlights the resource demands of implementing CAB/RPV and interrelated complexities at patient, health worker, and health system levels. Our results offer insight into opportunities and potential challenges when integrating CAB/RPV into practice. This includes considerations pertaining to clinic operations and logistics, health worker knowledge of and confidence in the implementation process, access to care among a given population of people living with HIV, and sustainability. For clinical innovations like CAB/RPV to reach all that may benefit, health systems must be responsive to these intricacies.
Footnotes
Author Note
This study is part of a multi-component grant to evaluate CAB/RPV integration at UNC ID. All authors are currently or have previously been affiliated with the broader university. Three authors have a direct affiliation with UNC ID, two as practicing medical doctors. The paper was developed by a diverse group of authors in terms of topical expertise and seniority. The team includes both public health and medical professionals with expertise in the areas of qualitative research, mixed methods research, HIV treatment and prevention, and implementation science. Half of the authors are early career researchers, and seniority within team ranges from graduate to post-graduate education levels.
Acknowledgments
The authors are deeply grateful for the support of the University of North Carolina Infectious Disease clinic (UNC ID) and to the health workers who shared their insights and experiences as part of this research.
Ethical Approval
This study was approved by the UNC Chapel Hill Institutional Review Board (21-2517).
Participant Informed Consent
All participants completed an informed consent process and provided written consent prior to participating in the research. Participants were offered $50 for their participation.
Author Contributions
HEH led coding and analysis and drafted the manuscript. CL coded interview data and critically reviewed the manuscript. HA collected interview data and critically reviewed the manuscript. OAM critically reviewed the manuscript. VG, CF, and SN provided technical feedback and critically reviewed the manuscript. SER conceptualized the study, provided oversight, and drafted the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by pilot funds provided by North Carolina Translational and Clinical Sciences Institute (Grant #UM1TR004406) and the University of North Carolina at Chapel Hill Center for AIDS Research (Grant #P30AI050410). SER received additional support from Doris Duke Charitable Foundation (Grant #2020143).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The qualitative interview data that support the findings of this study are not publicly available to protect participant confidentiality. De-identified excerpts may be made available from the corresponding author upon reasonable request and subject to approval by the relevant ethics committee.