
Abstract
Introduction
The human immune deficiency virus (HIV) remains a significant public health concern. By the end of 2020, about 37.7 million people were living with HIV of which 1.5 million were newly infected. 1 More than two-thirds (67%) of the HIV burden is from Sub-Saharan Africa. 2 In Ethiopia, HIV/AIDS has created a huge burden on the healthcare system and remains a threat to the lives of inhabitants. 3 In the country, the prevalence of HIV is mixed with wide regional, geographical, and sex variation. 3
According to Joint United Nations Program on HIV/AIDS (UNAIDS) report in 2021, despite the high incidence of HIV globally, AIDS-related deaths have reduced by 47% due to the availability of decentralized antiretroviral therapy (ART).1,4 These interventions help to expand and strengthen the ART care and treatment activities at regional, zonal, woreda, districts, and unit levels through targeted social mobilization and active community participation which are expected to create an enabling environment to prevent and control spread of the epidemic. This task shifting is: an intervention that has been implemented to rational distribution of care across the healthcare workforce. The efficacy of this intervention depends on training of providers and community health agents in prevention, treatment, care, and support activities which further strengthen community linkages and ensures availability of standard minimum packages of HIV/AIDS services at primary health care level which can be instrumental in accelerating and scaling up ART uptake. 5 Out-of-catchment ART initiation (OCAI) is defined, as accessible, available, free of charge, and faster ART services that are farther away from the homes of people living with HIV (PLWHIV).
Previously, ART commenced in 2003 as a fee-based intervention program and subsequently became a free service delivery in 2005. 6 The government of Ethiopia later decentralized ART services from hospitals to health centers in 2006 7 with the intention of scaling up access to HIV care services, ART treatment and improve patient retention in care. Despite this, a significant number of HIV-infected individuals still travel out of their catchment areas to initiate ART while these services are available closer to their living areas.
As a result, some central health facilities become overburdened causing prolonged client waiting time, reduced quality of care, and increased clinic attendance. 8 On the other hand, this results in a huge financial burden due to transportation to access care and untimely treatment which in turn negatively affects regular follow-up, the quality of care, the retention in treatment, and ART treatment outcome.3,8–10 Generally, ART uptake is negatively associated with the distant proximity to health facility. 11 This is due to high transport cost is also associated with travel to access health facilities for care. As a previous study reported, farther distance from the health facilities were strong predictors for poor treatment uptake among PLWHIV. 12
All public health facilities in Ethiopia currently provide ART services for PLWHIV. Therefore, HIV-infected individuals across the country are able to access ART within their catchment area. However, a significant number of HIV-infected individuals have initiated ART out-of-catchment areas. To our knowledge, little is known about the number and factors associated with PLWHIV accessing lifelong therapy out of their catchment areas. Thus, this study aimed to assess the magnitude of OCAI among PLWHIV on ART at Nekemte Comprehensive Specialized Hospital, Western Ethiopia.
Methods
Study Design and Period
A facility-based cross-sectional study was conducted among 423 PLWHIV on lifelong therapy at ART clinic in Western Ethiopia from November 25 to December 30, 2022.
Study Setting
The study was conducted at Nekemte Comprehensive Specialized Hospital Western Ethiopia. The hospital was established in 1932 by Sweden Missionary and is located in Nekemte town which is 328Km away from the capital city Addis Ababa. 13 The hospital commenced provision of ART services in 2005 and is currently giving holistic inpatient, outpatient, and community services to population within its catchment area. The hospital also provides integrated ART services with about 4500 PLWHIV currently on lifelong therapy. The HIV testing and ART treatment cascade in the hospital was adopted from the World Health Organizations’ (WHO) model that outlines voluntary counseling and testing (VCT) and provider-initiated testing and counseling (PITC).
Eligibility Criteria
All PLWHIV within ages > 15 years, attending ART at Nekemte Comprehensive Specialized Hospital and available during data collection period were eligible to participate in the study. However, eligible participants with hearing and speaking impairment, critically ill, and unable provide informed consent were excluded from the study.
Sample Size Determination
The sample size was calculated by single population proportion formula with the assumption of 95% confidence level, 5% margin of error, 10% none response rate, and 50% proportion for the magnitude of OCHAI among PLWHIV which was not available study prior to this study. The final sample size was 423. Thus, systematic sampling technique was used to recruit study participants.
Study Variables
Dependent variable
The dependent variable for this study is out-of-catchment area ART initiation.
Independent variables
This includes sociodemographic (age, sex, residence, marital status, educational status, occupation, and religion), behavioral and social-related variables14,15 (expected social support, substance use, perceived stigma, role in society, sexual history, and visit traditional healer(s)), HIV-related variables (disclosure status, place of HIV test, reason for HIV test, encouragement for HIV test, how often tested for HIV, family HIV serostatus, and HIV testing approaches), and regimen-related variables (where ART initiated, ART initiation time, adherence status, know other ART user(s), functional status).
Operational Definitions
Out-of-catchment area ART initiation: This is defined as when an HIV-infected individual access ART services away from their catchment area. When PLWHIV start ART out of their own zone by passing the health facilities found within/unit/district/zones, it is referred to OCHAT. This is further categorized as either within or out-of-catchment area ART initiation and was obtained from patient medical record or by asking patients.
Functional status as defined by WHO
16
Working: Able to perform usual work inside or outside home Ambulatory: Able to perform activity of daily living (ADL) but not able to work Bedridden: Not able to perform ADL
Social support
Any help/attention obtained from family, neighbors, and social workers that is measured and graded based on Explanation of the Oslo-3 Social Support Scale. 17
Stigma
Any perceived social discrimination that is measured by providing some sort of questions. This is categorized into a 5-point Likert scale.
Traditional healing
Refers to health practices, approaches, knowledge, and beliefs incorporating plant, animal, and mineral-based medicines, spiritual therapies, manual techniques and exercises, applied singularly or in combination to treat, diagnose, and prevent illnesses or maintain well-being. 18
Baseline WHO clinical stage: Assessing the severity of the disease based on certain clinical criteria to categorize the HIV positive patients into 4 stages (stages I-IV) based on the presence and severity of symptoms and certain laboratory findings.
Baseline CD4 count: Markers that is commonly used to understand HIV disease progression and for monitoring of ART treatment response. The result of the first test before the patient started ART was obtained from patient card.
TB/HIV coinfection: When an individual gets tested for both TB and HIV and is found to be positive. This was obtained from patient card.
Data Collection Instruments and Technique
The data were collected through interviewer-administered structured questionnaires. The questionnaire was developed from national ART guideline, ART intake form, registration logbook at ART clinic follow-up, and HIV testing and counseling format. The questionnaire was developed in English then translated to Afan Oromo by experts and translated back to English to maintain its consistency. The questionnaire contains sections (sociodemographic, behavioral and social, HIV, and regimen-related factors) for assessing OCHA, and its predictors. Data were collected via face-to-face interview and patient's medical chart review. Two BSc holder nurse data collectors and 1 supervisor, fluent in speaking, writing, listening, and reading Afan Oromo participated in data collection process. The data collection process was performed in private room after the respondents finished their routine ART follow-up services.
Data Processing and Analysis
EPI data statistical software version 3.1 and STATA version 14.0 were used for data entry and data analysis respectively. Data categorizing, recategorizing, and cleaning were performed, and the descriptive statistics were presented in frequencies and percentages for categorical data, whereas mean with standard deviation was used to present the continuous data. Both bivariable and multivariable logistic regression analyses were computed to determine independent variables associated with study outcome. Thus, variables with P value <.25 in bivariable analysis were entered into the multivariable logistic regression analysis to control for potential confounding variables. Odds ratio with 95% confidence interval (CI) and P value of <.05 was used to declare statistically significance in final model.
Data Quality Control
Pretesting was done on 5% of the total sample size and on participants with similar characteristics recruited from other hospital. Based on the findings, necessary tool modifications were made. The tool validity was checked by face validity. Two days of intensive training were administered to data collectors on the study instrument and data collection procedure including the relevance of the study, objective of the study, confidentiality, informed consent, and interview technique. The data collection process was performed under close supervision of the study supervisor and principal investigators. The collected data completeness was checked on daily basis. Collected data were carefully entered and cleaned before the analysis.
Ethical Considerations
Ethical clearance was obtained from the University ethical review committee of Institute of Health Sciences, Wollega University with reference number of IHSRPAD015/2022, and permission letter was secured from the Nekemte Comprehensive Specialized Hospital's administrative body. Written informed consent was obtained from each respondent before the data collection process. The respondents were well informed of their voluntarily participation and the right to terminate at any time they wanted. Confidentiality of the information was maintained by omitting personal identifier data of study participants.
Results
Sociodemographic Characteristics of the Study Participants
A total of 423 PLWHIV on ART participated in the study yielding response rate of 100%. The mean age of study participants was 33.43 ± 9.79 years. Majority of the participants were male (54.61%), married (49.65%), and housewives (32.15%). More than half (54.37%) of respondents attended formal education to primary school and majority of respondents (69.27%) were urban dwellers (Table 1).
Sociodemographic Characteristics of PLHIV Attending ART Follow-up at Nekemte Comprehensive Specialized Hospital From November 25 to December 30, 2022 (n = 423).

Clinical Characteristics
Majority (37.35%) of the study participants were diagnosed with the stage I baseline WHO clinical staging, and 43.97% had a baseline CD4 count of ≥500 cells/mL. Only 10.17% of the participants were coinfected of TB and HIV, and 82.74% attained working functional status; 57.92% of the participants reported PICT as the major HIV testing approach used (Table 2).
Clinical Characteristics of PLHIV Attending ART Follow-Up at Nekemte Comprehensive Specialized Hospital From November 25 to December 30, 2022 (n = 423).

Abbreviations: VCT, voluntary counseling and test; PITC, provider-initiating testing and counseling; WHO, World Health Organization; TB, tuberculosis; HIV, human immunodeficiency virus.
Behavioral and Social Characteristics
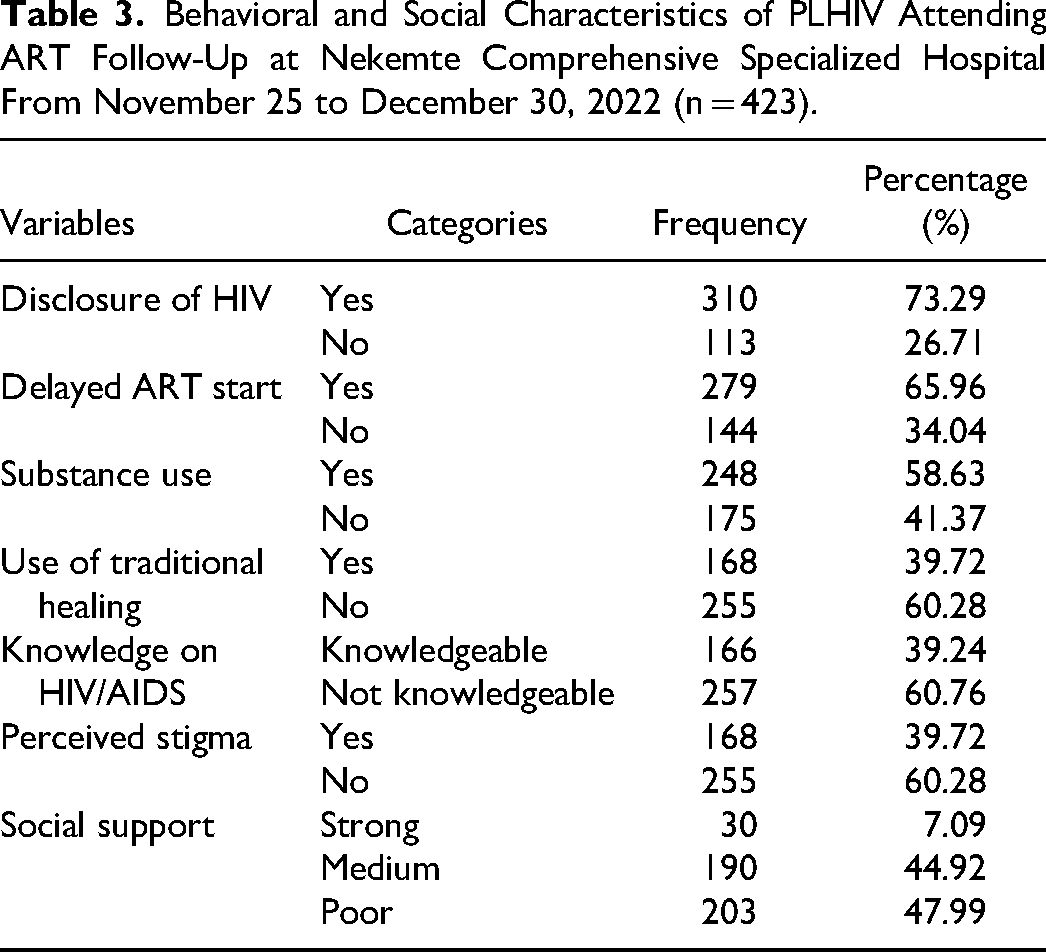
Majority (73.29%) of the respondents had disclosed HIV serostatus, did not use traditional healing (60.28%), and delayed ART initiation (65.96%). More than half respondents (58.63%) had substance using history, poor perceived social support (47.99%), and not perceived stigma (60.28%) (Table 3).
Behavioral and Social Characteristics of PLHIV Attending ART Follow-Up at Nekemte Comprehensive Specialized Hospital From November 25 to December 30, 2022 (n = 423).
Proportion of Out-of-Catchment Area ART Initiation
About 1 in 4, 93 (21.98%) of the study participants-initiated ART out-of-catchment area (95% CI: 18.28-26.20). Of all who initiated ART out-of-catchment area 52(55.93%) did not disclose their HIV serostatus, 53 (56.98%) of them had perceived stigma and about 55(59.1%) of them had used traditional healing before they initiated ART (Figure 1).

HIV seropositive disclosure status among PLHIV from out-of-catchment area and attending ART follow-up at Nekemte comprehensive specialized Hospital from November 25 to December 30, 2022 G.C.
Factors Associated With Out-of-Catchment Area ART Initiation
Both bivariable and multivariable logistic regression analysis was performed. Nine variables from bivariable analysis were entered into multivariable logistic regression analysis at P value of .25 significance. From multivariable logistic regression analysis, 6 independent variables remained significantly associated with the dependent variable at P value of .05. Female respondents (AOR = 2.42, 95% CI = 1.36-4.32; P = .003), respondents with perceived stigma (AOR = 3.413, 95% CI = 1.883-6.187; P = .000), and those that did not disclose HIV serostatus (AOR = 3.995, 95% CI = 2.454-7.872; P = .000) were more likely to practice OCHAI.
Additionally, participants using traditional healings (AOR = 1.91, 95% CI = 1.03-3.55; P = .039), got tested for HIV via VCT (AOR = 3.995, 95% CI = 2.21-7.19; P = .000), had HIV-related knowledge (AOR = 2.159, 95% CI = 1.184-3.938; P = .012) and with delayed ART initiation (AOR = 2.562, 95% CI = 1.32-4.96; P = .005) were more likely to practice OCHAI (Table 4).
Bivariable and Multivariable Factor Analysis for Out-of-Catchment Area ART Initiation among PLHIV Attending ART Follow-Up at Nekemte Comprehensive Specialized Hospital, Western Ethiopia, November 25 to December 30, 2022 (n = 423).a

Abbreviations: OCHAI, out-of-catchment ART initiation; ARTI, antiretroviral therapy initiation; COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; HIV, human immunodeficiency virus; VCT, voluntary counseling and testing; PITC, provider-initiating testing and counseling.
Bold are significant variables with P < .05.
P < .0001.
Discussion
Out-of-catchment area ART initiation is an overlooked concern in HIV care and ART program. ART can financially affect PLWHIV and health facilities either directly or indirectly. Surprisingly, current study reveals the prevalence of OCHAI to be 21.98%. Decentralized HIV care and management demands access to ART that is closer to community (within catchment area) and integrated delivery of the services within existing primary health care system. Despite this, current study indicates that a significant proportion of PLWHIV had initiated ART out of their catchment area.
Long distance to care is associated with lost to follow-up, poor appointment adherence to treatment, time taken off from work, and transport costs.18,19,21 Similar findings were reported from study conducted in different parts of Ethiopia22–24 and other African countries.25,26 In turn, poor adherence and retention in care can increase the risk of HIV-related illness, morbidity, mortality, and continued community HIV transmission.
Appointment adherence is thought to be indicative of PLWHIVs’ engagement in HIV care which in turn paves viral suppression. 20 In contrast, distance patients travel and time taken to access ART facility may compromise the service uptake.
The odds of OCHAI were 2-fold higher in female participants as compared to male. This may be due to the fact that females PLWHIV are more socially discriminated and blamed for trading sex than males. As a result, they may hesitant to initiating ART treatment within their catchment area. Female sex workers (FSW) are among key population and risk group for HIV infection and further transmit the infection within community. Upon awareness of HIV-positive status within this group, they are less likely to initiate ART within their catchment due to the fear of discrimination, stigma, and social life impacts that are linked with PLWHIV in this gender.27,28
The odds of OCHAI were also 2-fold higher among participants who previously used traditional healing when compared to their counterparts. We suggest that those who previously used traditional healing resulted to this form of care due to the fear of discrimination and their social concerns. This may have affected their likelihood to seek medical care in health facilities far away from their catchment.
Traditional healers and users are popular in local community, have acceptance within the population, and the practice is their source of income. Not to lose their popularity, acceptance, reputability of their healing practice, and income attributed to that practice, they may prefer to go far distance to initiate ART out of their catchment.28–30
Participants who had HIV/AIDS-related knowledge were 2.2-fold more likely to practice OCHAI as compared to their counterparts. Patients who had plenty of information about HIV/AIDS may also have knowledge on availability, and accessibility of ART which may influence their preference for a higher level of care. In order to get quality services, and as a result, may seek ART from hospitals that are located farther away from their location of residence.31–33
Participants with delayed therapy compared to those that initiated therapy early were 3 times more likely to practice OCHAI. Newly diagnosed PLWHIV are I most situations psychologically affected and due to fear of stigma, serostatus disclosure issues, family and social desirability condition. As a result, they may result to locations that are farther away from where they could be recognized to initiate ART. This may negatively affect their willingness to initiate timely ART, thus, limiting their opportunity to benefit from starting the lifelong therapy.32,33
Furthermore, participants who had perceived HIV/AIDS-related stigma were 3-fold more likely to practice the OCHAI. HIV/AIDS-related stigma is a critical issue that negatively affect HIV care and the cascade as a whole. 34 Due to stigma, PLWHIV may change their living address, jobs, and treatment site or health facility. 33 They may also not want to be seen by their relatives, coworkers, and friends at the ART clinic within their catchment area due to fear of loss of social support, job, and social interaction.34,35
The odds of OCHAI were 4-fold more likely identified in participants who did not disclose HIV serostatus as compared to those who did. HIV-positive serostatus disclosure is a challenge that impedes optimum HIV care, ART treatment adherence, and the prevention of new infection. Most of the time PLWHIV refuse to disclose their status for fear of divorce, family disharmony, blame as index case, missing social support, and loss of income.34,36–39As a result, they like to conceal their serostatus and prefer to start ART out of their catchment area away from their families, friends, and relatives.
In addition, participants who had tested for HIV via VCT were 4-fold more likely initiated ART out-of-catchment area as compared to those who were tested via PITC. Those who get tested for HIV through VCT probably have high knowledge about HIV/AIDS and they may know their risk levels. Along with their voluntariness to get tested for HIV they may also consider central health facilities for quality care than that of prefer health facilities. Majority of PLWHIV who get tested for HIV via VCT are priority and key population including FSW and their partners, merchants, and highly paid employers. These parts of the community are most of the time popular; so, they may fear to be known as a PLWHIV around their living home. As a result, they may decide to start ART at out of their catchment area.
Limitation of the Study
Data were cross-sectional and prevented inferring causality on the study population. Also, some data from the participants’ medical record were incomplete in which may have resulted to underestimation of factors associated with OCAI and introduce bias to the study.
Conclusion
In the current study, a substantial number of PLWHIV initiate ART outside their designated catchment areas. Females, traditional healing users, delayed ART users, those who perceived stigma, undisclosed HIV status, and who tested via VCT are study participants who were more likely practiced the OCHAI. Thus, enhancing further HIV serostatus disclosure, combating discrimination associated with HIV/AIDS, and promoting decentralized HIV care and ART services are highly recommended to be strengthened and reinforced for newly diagnosed HIV-positive people and become a concern in HIV continuum of care
Footnotes
Acknowledgements
The authors are grateful to the funding institution, data collectors, supervisor, and study participants.
Author Contributions
All authors made extensive contribution to the conception, design, acquisition of data, or analysis and interpretation of data, took part in drafting the manuscript or revising it critically for important intellectual content; agreed to summit the manuscript to the current journal, gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Availability of Data and Material
All data generated and analyzed are included in this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent Statement
Ethical clearance was obtained from ethical review committee of the Institute of Health Sciences, Wollega University with reference number of IHSRPAD015/2022. Permission letter was secured from Nekemte Comprehensive Specialized Hospital administrative body, and written informed consent was obtained from each respondent before the data collection process. All respondents have informed regarding confidentiality of their response, voluntarily participation, and a right to terminate at any time. Participants were given the chance to ask any questions about the study and were made free to refuse or stop the interview at any moment they wanted. All collected data were treated confidentially.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Wollega University. The funding institution had no role in the designing of the study, data collection, data analysis, and data interpretation, and writing of this manuscript.