
Abstract
In India and other low-and-middle-income countries, little is known about how intersectional stigma affects MSM engagement in ART. Informed by the Health Stigma and Discrimination Framework, we qualitatively examined how multiple stigmas influence ART engagement among Indian MSM. We conducted 3 focus groups (N = 22) with MSM living with HIV, aged 21–58 years, in Delhi and Hyderabad to identify potential intervention targets and solutions to improve treatment outcomes. Framework analysis and techniques were used to code and analyze translated audio-recordings. Findings revealed enacted stigma, associated with HIV and MSM identity, manifested as familial shame and healthcare discrimination, inhibiting access to support, and decreasing HIV care engagement. Anticipated stigma led to worry about disclosure and societal repercussions. Community-Based-Organizations, ART centers, and family members were primary sources of support, leading to increased ART initiation and retention. Potential solutions included using MSM peer-counselors, increasing social support, and providing HIV education to the general community.
Introduction
India has a concentrated HIV epidemic among key affected populations such as men who have sex with men (MSM). 1 The HIV prevalence among MSM population is 4.4%, which is about twenty times that in the general population (0.22%). 1 While free antiretroviral therapy (ART) is available through India's National AIDS Control Programme, there is limited data available regarding challenges MSM living with HIV (MSMLH) face in accessing and adhering to HIV care that could lead to suboptimal health outcomes.2–4 Stigma and discrimination in healthcare settings are reported as causes for low access to, and retention on ART among MSM.5–7 To effectively aid in treatment initiation and retention, it is imperative to further understand the challenges MSM face when attempting to access and maintain care.
Such challenges to receiving care may be understood through two theoretical frameworks: 1) The Health Stigma and Discrimination Framework, 8 and 2) Intersectionality Theory. 9 The Health Stigma and Discrimination Framework explains the development of stigmatization across healthcare. Intersectionality theory can be applied to better understand stigma relating to both sexual orientation and HIV status. This refers to an individual experiencing multiple marginalizations, such as MSM and HIV status, where addressing each separately does not improve their overall lived experiences. 10 Intersectional stigma refers to the combination of multiple marginalized identities within a person or group that lead to specific consequences. Intersectionality theory and intersectional stigma are terms which seek to address these effects. 11 Globally, MSMLH face stigmatization and discrimination within family units, the healthcare settings, and public spaces, leading to a lack of psychological support and employment opportunities.12–14 The same has been found true for MSMLH in India, who face intersecting stigmas based on sexual orientation (MSM stigma) and HIV status.15–17 However, further exploration is necessary to broaden awareness of how multiple stigmas faced by MSM influence HIV treatment engagement within the Indian context. Using Intersectionality Theory and the Health Stigma and Discrimination framework, we hoped to further understand and explain how multiple discrete identities may impact HIV care engagement for this population within the Indian cultural context.
Previous studies from India have shown that MSMLH experience barriers in access to ART and social support to a greater degree than the general public.16,18 The consequences of specific stigma manifestations, such as within the family, society, and hospital settings, are known to impact HIV care engagement globally,19–21 however, have not been fully discerned within this population. Additionally, the impact of disclosure and familial support has not been well studied. Family, within the Indian context, plays a unique role in the process of social acceptance and thus avoidance of stigmatization.14,22 Other studies have found that the some MSM in India may be married to women. 23 How this is related to stigma and care seeking engagement is not well understood and has been elaborated further in this study.
We conducted this qualitative study to understand how stigma attached to sexual orientation and HIV status influences HIV treatment engagement among MSM living with HIV (MSMLH) in India. Guided by the aforementioned theoretical frameworks, this study explored potential pathways between intersectional stigma and access to support and treatment, and retention in care. The findings will help to identify potentially modifiable targets and design interventions and strategies to improve health outcomes among MSMLH.
Methods
Setting and Participants
We conducted three focus group discussions (FGDs) among MSMLH in India between September and November 2019. Two FDGs took place in Delhi in North India, and one in Hyderabad, South India. The sites were chosen based on the feasibility of recruiting adequate number of MSMLH through our community partner agencies, and partly driven by our wish to include MSMLH from Northern and Southern regions in India. The number of FGDs was limited to three, primarily because of budget constraints. Participants were recruited by peer outreach workers at Vihaan Care and Support Centers 24 that are operated by local community-based organizations (CBOs) in partnership with government ART centers, and offer support services for HIV treatment engagement. All participants self-reported sex with other men. As with any other group, MSM in India come from diverse backgrounds including various degrees of sexual orientation disclosure, family support, and even being married to women. To capture diverse experiences of MSMLH, we used maximum variation sampling, a subtype of purposive sampling 25 (eg, with respect to diverse age groups, sexual orientation identities and disclosure, and being married to women). Additionally, several indigenous identities are used by Indian MSM, for instance, kothis (feminine and receptive) and panthis (masculine and insertive). To determine self-identified sexual identities, our demographic survey listed several options (kothi, panthi, double-decker, gay/homosexual/queer, heterosexual/straight, bisexual, MSM, or other).
Data Collection
Two authors experienced in qualitative data collection and identifying as sexual minority individuals conducted the FGDs in local languages (Hindi and Telugu), co-moderated by trained MSM peer outreach workers in the two study cities. A semi-structured topic guide, which was informed by the aforementioned frameworks as well MSM community leaders, was used. The guide explored various forms of stigma and discriminatory experiences due to sexual orientation and HIV status in various settings (family, healthcare, and society), and how such stigma impacted participant's access to care and care engagement. Each FGD ranged from 60 to 90 min. Participants received an honorarium of INR 200 (∼2.50 USD) for their time. FGDs were audio-recorded, translated, and transcribed into English for data analysis.
Data Analysis
Three authors with diverse backgrounds (initials blinded for review) developed a codebook based on codes identified within the data (emergent codes) as well as based on The Health Stigma and Discrimination Framework 8 and Intersectionality Theory 5 (pre-determined or a priori codes). Code structure was produced via thorough readings of all three transcripts by three authors. Coding and categorizing techniques were adapted from framework analysis 26 and grounded theory approaches 27 to produce an agreed upon code book and Dedoose software was used to organize and code the data. Additionally, we used contiguity-based connecting strategies: a deterministic approach to understand the cause and consequence(s) of an event or phenomenon by locating the relationships among them in the participants’ narratives or among categories.27,28
The Health Stigma and Discrimination Framework guided analysis pertaining to four thematic categories: 1) stigma marking – assignment to a marginalized group (in this population, MSMLH), 2) stigma manifestations – how such marking may influence the lived experiences and outcomes of affected populations, 3) drivers – negative regulators which increase stigma marking and manifestations, and 4) outcomes – how the course of stigmatization creates barriers or facilitates access to support. Following a modified version of this framework, we categorized data by theme and content. Finally, we constructed a conceptual model based on the relationships and pathways supported by the data to visualize the key pathways between intersections stigma and access to support systems and barriers to healthcare. We conducted member checking 29 with MSM living with HIV, MSM community leaders, and staff at [name blinded for peer review] running service programs for MSM to verify findings and conclusions. 30
Author Reflexivity
To ensure the rigor of this study, the authors implemented reflexivity. The authors critically examined their own perspectives regarding key themes, study findings, and overall review results, considering their professional and life experiences. The research team, consisting of sexually and racially diverse members with expertise in conducting HIV research in the Indian context, actively participated in discussions to reflect on their own individual experiences and insights, contributing to the integrity of the work. Based on the intersectionality framework, the team conducted this study with the belief that HIV status and sexual orientation can impact stigma but took steps to conduct interviews in a neutral manner.
Ethical Approval and Informed Consent
All participants provided written informed consent. Study participation was fully voluntary and participant privacy and confidentiality were ensured. Institutional Review Boards of Albert Einstein College of Medicine (approval number 2019-9915) and Alliance India (approval number 007/2019-0009) as well as the Government of India's Health Ministry Screening Committee (HMSC), Indian Council of Medical Research (approval number 2019-7054) approved this study. All patients provided written informed consent prior to enrollment in the study.
Results
Participant Characteristics
A total of 22 MSMLH participated in three FGDs. Participants were aged between 21 and 58 years. All participants were assigned male sex at birth and identified as men, 18 participants identified as gay/MSM, 2 identified as panthi, and 2 as bisexual (Table 1). All participants were currently on ART. Of 15 participants with available demographic information (due to a procedural error, sociodemographic information was missing for seven individuals), 4 (27%) had disclosed their sexual identity to at least one person and 6 (40%) were married to women (Table 1).
Overview of the Findings
Figure 1 shows a conceptual model of the pathways between HIV-related and MSM stigma, their influence on access to social support, HIV care engagement and treatment, and the impact of various forms of support networks based on the findings from the study.

Pathways between stigma manifestations and HIV care engagement among men who have sex with men living with HIV in India. *CBO: community-based organization; ART: Anti-retroviral therapy. Intersectional stigma manifestations in this model relates to being both MSM and living with HIV.
Experiences of Enacted Stigma and its Effect on Social Isolation
Participants recounted numerous events in which they were subjected to enacted stigma due to their HIV status and MSM identity. Instances of enacted stigma can be separated by perpetrator identities: the medical community, general population, or family members and friends. Such stigma often presented as discrimination and social exclusion: “After knowing about the HIV positive status, family and friends starts making distances and they will also talk about our sexual orientation as well as our HIV status to other friends,” (Delhi, FGD 2). Such enacted stigma gave rise and shed light on other forms stigma manifestations, including internalized stigma and familial shame: “If suppose, I am moving within my circle of friends, when they come to know that I am like this [MSM], they isolate me. They are all men. There is a difference between their behavior and my behavior. Once they come to know about my identity, they isolate me immediately,” (Hyderabad, FGD 3).
Familial Shame and the Subsequent Lack of Social Support
Discrimination by family members materialized as shame within the family and the outside community. Familial shame was discussed in all focus groups: the notion that MSMLH shed stigma not only on oneself, but also on family members. Thus, stigma on an individual led to discriminatory actions upon their parents, partners, and children: “Even my son faced a lot of stigma in the society because of my HIV status. People assumed that he got infected from me. So, nobody used to play with him. To prove that my son is not HIV positive, I had to go with him for the testing…the report of my son was negative. And proved in the neighborhood after his negative report,” (Delhi, FGD 1). Participants illustrated how stigma circulated and radiated to family members. Marriage prospects for the siblings changed, family name was dishonored, and family resources decreased due to HIV stigma and MSM stigma: “This is the worst kind of life, we always have to act in life, we have to act when we are with family or friends or with relatives, everybody. Normally people stay individually but in our community our name will be connected with parents, friends, relatives also,” (Hyderabad, FGD 3). An unexpected finding was marriage as a means to mitigate enacted stigma. Whether this was MSM stigma or HIV stigma remained unclear. Various members in all three focus groups were married to women while identifying as MSM. The reasons for these unions included familial pressure, lessening the likelihood of disclosure, and decreasing stigma related to HIV or MSM identities: “I got married in 2015 with a HIV negative woman under family pressure,” (Delhi, FGD 1). The cultural significance of marriage was used to counterbalance the stigmatization and shame MSM or PLHIV brought to their families: “So from that day I was living my life happily and I married to HIV positive woman in 2008. My family and relatives accepted me,” (Delhi, FGD 1). In two of three focus groups, participants noted marriage to specifically HIV-positive women, many of whom were aware of their partner's sexual orientation: “After 1 year I married a HIV-positive woman, and she knows that I am an MSM. She doesn’t have any problem on my sexuality (Delhi, FGD 2). In these women, participants gained family acceptance and a support system who also had lived experiences with HIV. In turn, many women received monetary and social support: “She told me that she has no problem and she just want me to take care of her daily needs and raise the child,” (Delhi, FGD 2). However, many participants were aware that marriage did not truly relieve stigma. Family members and friends living without HIV or who are of a sexual majority often proposed marriage as a solution; nevertheless, participants communicated that actions to reduce stigmatization are what were truly lacking.
Discrimination Within the Healthcare System
HIV-positive status and sexual minority identities led to enacted stigma by healthcare personnel. Participants in all three focus groups reported being or knowing someone turned away from the hospital due to their HIV status. This illustrated the limited and low-quality care received by MSMLH: “In the Government hospitals, if we are sick, they do not give us the proper and correct treatment, as they cannot tell us to go away nor do they want us to stay. They do not tell us to go away directly. Hence, we feel troubled after staying there,” (Hyderabad, FGD 3). When admitted, they were subjected to discrimination and often their HIV status was outed: “If we are admitted in the government hospital, then they don’t allot us bed. If they allot us the bed, then we have to face a lot of stigma. They don’t even change our bed sheet and never take care of us. They treat us as we are alien. The nurses and the ward person reveal our HIV status to the room partners and humiliate us,” (Delhi, FGD 1). Such pathways can be seen in Figure 1.
Due to their illness, participants noted the frequency of necessary hospital visits. However, when faced with repeated acts of discrimination, these men felt neither safe nor comfortable receiving care due to enacted and anticipated stigma. Belief that their healthcare team feared PLHIV and blamed MSMLH as the sole carriers and propagators of the disease created fear among participants to access care: “I was admitted in [a government] hospital, the nurse came to me and told me that from now in your body the blood would get infected by HIV virus. She asked me how you can live now. And after saying these lines she moved on ahead,” (Delhi, FGD 1). This was also seen to lead to internalized stigma. “We feel very bad, and we feel it is better to die than face this situation, whenever we are reminded of these words, we feel really bad,” (Hyderabad, FGD 3).
Treatment was further limited when individuals disclosed their sexual orientation. To receive care, participants in Delhi mentioned the recurrent need to call leaders of their community. When care was received, it was frequently worse or suboptimal as illustrated by this individual: “Once I went with my MSM friend to admit him in the ward. They were not allowing him to admit. Then we called our RWA [Resident Welfare Association] member. When he came, they allow my friend to get admit in the ward. But next day in the morning only, the staff discharged him after giving glucose drip even they knew that he was not feeling well. In Government hospital, TGs and MSM has to face a lot of stigma and discrimination,” (Delhi, FGD 1).
Anticipated and Perceived/Community Stigma and the Result on Adherence
Anticipated Stigma and the Fear of Disclosure
Anticipated stigma also resulted from MSM and HIV stigma. In all focus groups, participants recounted their fear of discrimination and the perceptions of community members, whether based on behaviors, disclosure, or through medication adherence: “They come to know that we are MSM based on our walk, talk and our behavior. Once they understand that, they start discriminating,” (Hyderabad, FGD 3). The relationship between fear/anxiety and ART initiation and adherence was also emphasized in the focus groups. Figure 1 illustrates the indirect pathway of how stigma manifestations led to a lack ART care engagement. Fear of HIV in consort with anticipated stigma led to a lack of ART initiation: “It is so frightening. The fears that an MSM has…the way we boil in our hearts…but… we cannot say anything” (Hyderabad, FGD 3) and “Some people think that they will die now, then what is the benefit of taking medicines?” (Delhi, FGD 2). Some participants were unable to see the advantages medications could offer and instead anticipated the condemning medications could cause if found. Thoughts of treatment futility were also discussed. Additionally, fear of disclosure or being outed (disclosure done by someone other than the respondent, without the respondent's permission) was a large driver of anticipated stigma: “If someone leaks my status, then everyone will stare at me and will give me a dirty look. And will be wondering about how I got this infection,” (Delhi, FGD 2). The worry of being seen as an outcast coerced individuals to hide their identities resulting in decreased treatment engagement.
Perceived/Community Stigma and Medication non-Adherence
Perceived/community stigma in combination with anticipated stigma surfaced as another cause for non-disclosure of HIV status and/or sexual orientation. This is mainly because of past experiences of stigma that either the person had faced or witnessed happening to others. The need to hide one's identity due to mistrust led to a lack of treatment initiation and retention: “Some people do not even take medicines because they are tortured by the family members” (Delhi, FGD 2). Even when treatment was started, fear and anxiety hindered the overall adherence to medication. For instance, individuals worried about disclosure through medication and its impact on community-life: “I change the container of the medicine and then take my medicine at time. I don’t want to tell anyone about my medicines. Even I throw the empty bottle of medicine far away from my home,” (Delhi, FGD 2) and “No, one day my father has seen my medicine. And he took my medicine to a doctor and investigated about it. On the next day, he came to me and asked me about the medicine,” (Delhi, FGD 1). Adherence to these medications at a specific time each day revealed respondent's necessity for medication, and possibly, the reason for it. This led to stigmatization within the workplace as well job-acquisition discrimination. If these medications were found by friends and family, disclosure of HIV status, and possibly sexual orientation, became possible: “I go to village I have to quit ART drugs because nobody knows about my HIV positive status in my relatives,” (Delhi, FGD 2). Therefore, medication was often seen as a pathway to forced disclosure and stigmatization: “Because of this stigma we had to quit medicines. There is a fixed time to take ART medicine. If we are at home, we can easily take our medicine but if go to somewhere or at friends’ home and we have to take our medicine then our friends start asking question ‘Why are you taking this medicine daily’ and “What kind of medicine is this which you have to take at a fix time daily?” (Delhi, FGD 1).
Potential Solutions to Reduce the Impact of Stigma
Access to support emerged as the leading facilitator of both adherence and treatment initiation. The ability to access support systems was seen lessen feelings of fear, worry, and depression. This decreased the strength of stigma drivers. Disclosure and access to a CBO or ART center emerged as factors that increased an individual's access to support.
Disclosure of HIV or Sexual Identity to Improve Access to Support
Findings reveal that, when rooted in trust, HIV or sexual identity disclosure facilitated access to support networks for HIV treatment engagement. Such support networks included family, friends, healthcare workers, and other MSMLH: “I was diagnosed with HIV in 2005, I started to panic and thought what would happen if someone would know my status at home. But I never hide my status from my family. I told to my cousins and mother that I got this infection. After knowing, they supported me and said nothing to worry. We all are with you,” (Delhi, FGD 2). Following disclosure, sources of support were aware of the individual's illness. This enabled increased aid with access to treatment, emotional support, and adherence. As seen in all three focus groups, with support systems came confidence and ease in treatment protected from stigma. When families were aware of PLHIV, participants no longer needed to worry about unwanted disclosure, medication finding, or exclusion from family. In fact, their family often enabled treatment initiation by accompanying them to ART centers or provided reminders to take medications daily: “Because at the time I have to take medicine, I am busy on call at that time. So, my mother always reminds me to take medicine,” (Delhi, FGD 2). Additionally, when participants disclosed their HIV status and received support from family, friends or counselors, the fear associated with HIV was mitigated. These support systems provided reassurance and confidence so that worry or depression relating to, or caused by, the disease was appeased: “I discussed my HIV status to my two general close friends. That was the turning point of my life, they helped me a lot and also told me that HIV is not a non-curable disease and you should go to doctor for your medication. From then I start working in NGO and helped others to overcome this kind of depression,” (Delhi, FGD 1).
Contrastingly, in all three focus groups, some participants recounted disclosing their HIV status but not sexual orientation. Fear of MSM stigma prevented individuals from disclosing both identities. As a strategy to conceal their sexual orientation, some participants changed their behaviors and emphasized their family life. The participants illustrated how MSM stigma, separate from HIV stigma, was undoubtedly an impedance to disclosure and hindered access to care and support, “Because if we tell someone in the family that we are gay or we had relationship with men, they will not accept us and start hating us,” (Delhi, FGD 2). While trust in another person often facilitated disclosure to that individual, mistrust appeared to result in non-disclosure. When unsupportive or disparaging individuals uncovered the identities of MSMLH, access to support became onerous as passages to supporting groups and healthcare were blocked. In some instances, this was due to further shame placed on individuals. Conversely, when sexual orientation or HIV status was disclosed to trusted individuals, access to a support system and its positive benefits became attainable.
Community-Based Organizations (CBOs) and ART Centers as Supportive Communities
CBOs and ART centers were often associated with access to support due to their inherent role in provision of support. When visiting CBOs and ART centers, some participants felt that they could easily access counseling, treatment, and emotional support: “In the ART centers, ICTC [Integrated Counseling and Testing Centers], skin treatment centers, our reception is very good. It is better than what the general population gets. They sometimes give more preference and importance to us [MSM]. They take proper care of us. They explain what medicine to take, how long to take each one of them, whether it is the doctor or somebody else. They tell us what to do and what not to do, to take certain medicines…They ask us to come on time. They take good care of us in this respect,” (Hyderabad, FGD 3). The healthcare workers in these ART centers served multiple purposes including as educators and care and support providers, which made PLHIV feel comfortable in these centers and decreased pressures to conceal their MSM identity. Such positive experiences appeared to support ongoing engagement and retention (see Figure 1).
Community was seen as an essential part of support. Peer groups were able to provide comfort, education, and a sense of solidarity. Participants visited CBOs or ART centers, witnessed other MSMLH living with productive, happy, healthy lives, and envisioned their potential future: “They told me that this all network is positive. How we are, you will be like that. Don’t be tensed. You will get tested and given medicines. We are healthy and we have this disease since many years. Don’t be scared you will be fine. Then I thought for that whole night. Yes, that sister and sir are good. I will also use medicine. I am also positive right. I will also use. I thought so after thinking for all night. I went to ART center and gave a [lab] sample,” (Hyderabad, FGD 3). Access to these centers and peer groups provided positive thoughts about care while helping diminish anxiety. With support systems in place, individuals were better able to initiate their ART plan and promote adherence, as illustrated in Figure 1 . Participants conveyed the power their community had to ensure proper treatment and respect: “…the presence of the network of MSM, NGOs have helped us a lot. We have got some confidence. We feel that they are our people. If we go there…we will get justice,” (Hyderabad, FGD 3).
Education and Inclusion
The need for change was brought up by participants in all three FGDs who believed that an increase in education and knowledge, thus inclusivity, could result in change. Two specific target groups for interventions were mentioned: the community (including family, friends, and the general population) and healthcare personnel. When participants spoke about education, they emphasized knowledge on HIV, with only a slight focus on same-sex sexuality.
Education for the Non-MSM, Non-PLHIV Communities
Focus group data illuminated the need for and importance of spreading information about the science of HIV transmission on the community level. Strategies included counseling and educational sessions at schools and colleges, awareness programs, and accessible information on testing. Additionally, participants noted a need for proper counseling for parents and other family members of PLHIV: “Yes, if proper counselling is given to parents, then they will understand us,” (Delhi, FGD 1). Family interventions emerged as necessary mitigators of HIV and MSM stigma, and promoters of treatment engagement and adherence: “We want people to have more awareness of MSMs and trans-genders. How they should talk, how they should behave, the problems that occur due to such bad behavior [mistreatment] (Hyderabad, FGD 3).
Transforming Interactions Within the Healthcare Setting
Enacted stigma by the medical community emerged as a repressive barrier to care. Participants noted a need for health personnel-specific interventions such as education and bias reviews. In all three transcripts, several examples of reported breaches of confidentiality were seen: “The nurses and the ward person expose our HIV status among the room partners and humiliate us,” (Delhi, FGD 1). Participants noted that their HIV status had been disclosed to other patients or unnecessary personnel by nurses and doctors: “Doctor has written a plus symbol on my sheet, then the duty nurse what she did is that she told about this to all the other nurses that the person in that bed is a positive case so you have to be careful when you go to him or talk to him, you have to wear gloves, she was telling this in front of everyone,” (Hyderabad, FGD 3). Participants asserted that confidentiality must be maintained throughout the stay of care for all individuals. To further maintain confidentiality, some participants suggested using scientific words as secret codes to identify HIV status, such as CD4 count, and refraining from using the terms AIDS and HIV interchangeably.
Within ART centers and CBOs, participants portrayed a need for knowledgeable counselors. Specifically, counselors who identified within the MSM and PLHIV community were desired. Participants believed this to allow greater understanding, lack of stigmatization, and open communication,” We have faced many troubles until now. We want that the future MSM, transgenders or other people of our community…do not face these troubles. We want our community people to be as happy as the general population is. If the CBOs or NGOs help in developing all skills among the people of our community in the future, it would definitely benefit them. This is what we wish,” (Hyderabad, FGD 3).
The benefit of decentralized HIV care and ART provision was also reported in all FGDs. On multiple occasions, participants noted that medication administration and dispensation should be done at CBOs for MSM. Participants noted that these centers should act as testing and counseling centers as well. The need for a more holistic, customizable approach to counseling was clear and may play a role in resolving misconceptions about ART and increase adherence.
Discussion
This qualitative study reports on how multiple types of stigma may impact HIV care engagement for MSMLH in India. Analysis of focus group data shed light on the numerous factors that facilitated and hampered HIV care engagement. Study findings convey the importance of access to support as social support emerged as the key facilitator to increase treatment engagement and ART adherence. Research on how stigma influences HIV care engagement for MSMLH within the Indian context is novel and confirm similar findings from studies in other settings. 31 Participants reported that stigma marking was caused by the interplay of drivers, culture, and perceived normative behavior. Ascription to a minority identity, either as MSM and/or person living with HIV (PLHIV), contributed to enacted, anticipated, and perceived/community stigma. Ultimately, enacted stigma presented as familial rejection and discrimination within healthcare settings. Drivers increasing stigmatization included fear of disease, fear of disclosure, familial shame, and medical community mistrust. Results also highlight potential solutions to increase access to support which may include expanding educational and inclusivity-based programs within the greater community 32 and to strengthen the services provided by CBOs and ART centers, such as through the provision of HIV treatment, care services, and prevention methods, to provide safe healthcare and improve health outcomes. 33
The study findings highlighted the role of disclosure of marginalized identities and how this may impact the experience of stigma as well as influence social support access. As alluded to in the findings, the type of disclosure (ie, self vs involuntary) impacts the level of stigmatization. 34 Several participants reported disclosing their HIV status, but not sexual orientation. Many of the solutions to reduce stigmatization and access to healthcare posited by the participants focused on HIV stigma, treatment engagement, and societal inclusion of PLHIV, suggesting perhaps a greater acceptance for PLHIV than MSM identity in India. This may be due to a relatively long history of national efforts targeting HIV attitudes and awareness and the lack of those regarding sexual orientation. Adult consensual same-sex relationships in India were decriminalized in September 2018, only a year before this study initiation. Therefore, participants might have perceived addressing HIV stigma as a more socially acceptable way towards addressing MSM stigma. Nevertheless, as seen within the results of this study and those of previous studies, the intersectional stigma formed by HIV stigma and MSM stigma demand both be addressed together for treatment improvement.7,16,35,36 Thus, in addition to educational programs on HIV, there is a need to initiate programs and education on sexual diversity.
While disclosure of HIV status can prompt access to support and care, it can also lead to pressure within family networks. 14 Marriage holds significance in Indian society37,38 and disclosure of HIV status may play a role in increasing familial pressure to marry. 34 Thus, marriage played a role in alleviating stigma manifestations and familial pressure, assuaging HIV stigma, and relieving the risk of undesired disclosure of sexual orientation. While some participants indicated marriage as a possible immediate solution, this is likely rooted in the emphasis and prioritization of heterosexual marriage organization. The data suggest that, given the pervasive patriarchy and heteronormativity in the Indian society, portraying oneself as a heterosexual, signified by getting married to a woman, may be one option to maintain societal status and avoid discrimination. However, such an action is not a long-term solution as it has the potential to lead to great amounts of distress in the future to oneself and female spouse. 39 What is needed is family and society-based interventions to encourage and motivate acceptance.
As suggested in the narratives and reported in previous studies, 40 there is a clear connection between perceived positive familial support and increased treatment adherence as well as reduced psychological distress. Previous studies have shown the numerous benefits and ways in which PLHIV may gain support and aid from others.21,41 This support included material resources, encouragement, reminders to take medication, counseling, and awareness of the fact that others living with HIV were prospering on ART. 41 Meanwhile, negative family interactions often led to higher rates of depression, feelings of rejection, and internalized stigma.21,40,42 As such, support programs for MSMLH in India and elsewhere should consider developing strategies to help foster and reinforce family support. 43 Interventions focused on changing perceptions, attitudes, and understanding of HIV and MSM are needed as family perceptions of HIV and MSM are usually based on community and societal conventions.44,45 Previous studies have suggested that establishment of community support when starting HIV prevention programs could lead to higher community acceptance and engagement. 46 Community-based preventative health education in HIV risk reduction and counseling have also been seen to improve knowledge and attitudes towards HIV. 46 Based on such previous findings, educational programs, regarding both HIV and MSM, should be amplified within key populations as well for communities with frequent interactions with MSM living with HIV. These may include gender sensitization classes or talks at schools, within families, and other community meetings. 32
Cycles of enacted stigma by the medical community were strongly linked to lack of or delay in ART initiation and care disengagement. Education of staff members and the use of peer counselors (other MSM living with HIV) have been shown to decrease stigmatization and increase care engagement.47–49 Previous studies have shown that enacted stigma by healthcare providers stems from transmission-related fears and misconceptions as well as limited experience working with PLHIV. 50 Interventions for healthcare providers should include thorough training of universal precautions as well as formation of educational programs on the health ramifications of HIV. MSMLH should be involved in all stages of intervention and implementation to ensure meaningful interactions between healthcare providers and PLHIV. 50 This is even more significant in a post-pandemic world, as the challenges faced by PLHIV, including MSMLH, highlight the COVID-related economic and psychological stress influencing health behaviors and outcomes. 51 The findings also indicated the need for community leaders who act as healthcare personnel, beginning with hiring intra-community members: MSMLH. Involving PLHIV in the provision and development of healthcare has been seen to improve healthcare outcomes. 52 Findings suggest that CBOs and ART centers should augment the provision and access of counseling services and provide personalized care. For instance, while many participants identified as MSM, the breadth of gender and identity terminology was expansive. Therefore, interventions may be interested in focusing on individual behaviors, rather than identity ascription. Developing Community-Based Organizations (CBOs) could increase access to treatment by reducing outward exposure, such as disclosing one's status by visiting HIV treatment sites. NGOs should be strengthened to provide HIV medication administration, dispensation, and testing. 33 Such decentralization of healthcare promotes trust and safety which contributes to an increase in engagement and adherence. Future studies should investigate how trust rooted in peer support, built-in social networks, and access to personalized care can lead to confidence and a rise in voluntary disclosure with greater access to ART.
Limitations
This study had several limitations. Participants were clients accessing care and support services from CBOs or networks for PLHIV, and who felt comfortable disclosing their HIV status and sexual orientation to peer recruiters and interviewers. Thus, the findings may not be reflective of MSMLH not accessing such services or not publicly disclosing sexual identity or HIV status. Because qualitative data collection was limited to two large metro cities and three FGDs, findings are not generalizable to other MSM or MSMLH and may limit exploration of themes. While generalizability is not the focus of this study, findings may be conceptually generalizable and therefore transferable to similar settings. As these were not individual interviews, we were unable to examinate how individual characteristics impact stigma which future studies may want to explore. Additionally, future qualitative and mixed methods studies are warranted to better understand pathways between structural and individual stigma for Indian MSMLH as well as placing focus on mental health and structural stigma.
Conclusions
Overall, our study shed light on pathways between intersectional stigma and access to support and HIV care as well as identify short-term modifiable targets for CBOs to address stigma affecting MSMLH. Discrimination in healthcare, familial rejection, and mistrust stemmed from stigma associated with being both a PLHIV and MSM, with a perception that HIV stigma may be more addressable compared to acceptance of MSM identity. Participants laid out pieces to a process which they believe will benefit themselves and future MSM living with HIV which includes building intra-community and familial trust, facilitating safe disclosure, ensuring confidentiality, and strengthening support systems. Finally, findings suggest that strategies to decrease the impact of intersectional stigma on MSMLH should consider increasing diverse types of support and development of outreach interventions for families, healthcare providers, community members, and other MSMLH – areas that warrant further research to develop evidence-based strategies.
Participant Characteristics.
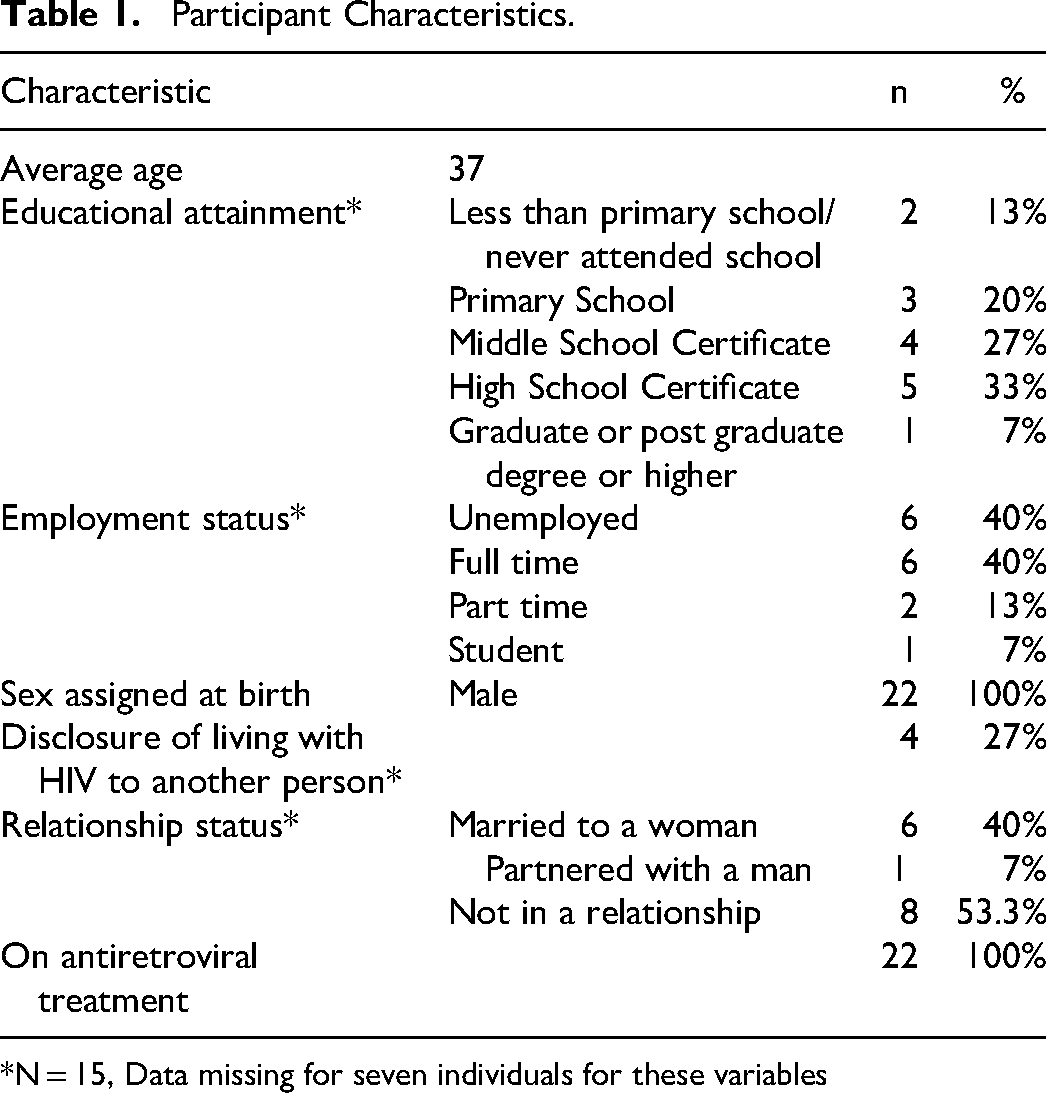
*N = 15, Data missing for seven individuals for these variables
Supplemental Material
sj-docx-1-jia-10.1177_23259582231199398 - Supplemental material for Pathways Between Intersectional Stigma and HIV Treatment Engagement Among Men Who Have Sex with Men (MSM) in India
Supplemental material, sj-docx-1-jia-10.1177_23259582231199398 for Pathways Between Intersectional Stigma and HIV Treatment Engagement Among Men Who Have Sex with Men (MSM) in India by Kiran Bhutada, Venkatesan Chakrapani, Fazlur R. Gulfam, Jonathan Ross and Sarit A. Golub, Steven A. Safren, Rita Prasad, Viraj V. Patel in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgements
The authors would like to thank the participants who generously gave their time and effort to participate in this study. We also extend our gratitude to the Community Advisory Board at India HIV/AIDS Alliance for their valuable insights and feedback. In addition, we thank Sonal Mehta and Viswanathan Arumugam for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institutes of Health, (grant number P30AI124414, R21MH118102).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.