
Abstract
We tested a couples HIV testing and counseling (CHTC) intervention with male couples in Atlanta by randomizing eligible couples to receive either CHTC or separate individual voluntary HIV counseling and testing (iVCT). To evaluate the acceptability and safety of CHTC, main outcomes were satisfaction with the intervention and the proportions of couples reporting intimate partner violence (IPV) and relationship dissolution after the service. The results indicated that the service was very acceptable to men (median 7-item index of satisfaction was 34 for CHTC and 35 for iVCT, P = .4). There was no difference in either incident IPV (22% versus 17% for CHTC and iVCT, respectively, P = .6) or relationship dissolution (42% versus 51% for CHTC and iVCT, respectively, P = .5). Based on the preliminary data, CHTC is safe for male couples, and it is equally acceptable to iVCT for men who have main partners.
Men who have sex with men (MSM) in the United States 1 and many other countries 2,3 are experiencing resurgent HIV epidemics. In the United States, new HIV infections are largely occurring among young MSM, 4 and they are disproportionately occurring in MSM of color. 5 Despite relatively high reported levels of annual HIV testing among MSM in large US cities, a large proportion of MSM living with HIV report being unaware of their HIV infections. 6 Thus, increasing the utilization of HIV testing and awareness of HIV serostatus among MSM in the United States must be considered a cornerstone of HIV prevention efforts and is an integral first step into linkage to care.
New, integrated approaches to HIV prevention for MSM have been called for, and HIV testing has been identified as a critical “gateway” to a comprehensive package of HIV prevention services for MSM. 7 Importantly, the recent Lancet review of HIV prevention for MSM noted that current efforts have been incongruent with men’s lives, and it called for the development of new services that reflect the lived realities and relationship contexts of MSM. 7 HIV transmissions from main partners have been reported to comprise an important—and perhaps even a predominant—source of new HIV infections among MSM in the United States. 8,9 Developing HIV prevention services for couples has to date been largely overlooked and is thus a priority area for research and program development and might be a way to provide intervention efforts that more accurately reflect both the epidemic and the lives of MSM. 10
Couples HIV testing and counseling (CHTC, also historically referred to as CVCT to emphasize the voluntary component) is a couples-based HIV testing service provided in many parts of the world outside of the United States—predominantly in low-resource countries with generalized HIV epidemics—and is considered a “high-impact” HIV prevention intervention in those settings. 11 In urban African heterosexual couples, CHTC has been associated with substantial decreases in HIV incidence within serodiscordant partnerships and with substantial behavioral shifts including increases in condom use. 12 The US President’s Emergency Plan for AIDS Relief (PEPFAR) program has recommended that a CHTC service adapted for MSM should be considered as part of comprehensive HIV prevention services, 13 and the World Health Organization has recognized the potential for high levels of serodiscordance among MSM in the context of their recently released CHTC guidelines. 14
We thus adapted a CHTC service specifically for US MSM. In general, the service comprised a 30- to 60-minute session between a male–male couple and a trained HIV tester/counselor, which included pretest discussion of HIV risks, HIV testing of both partners, skills building around sexual agreements, return of HIV test results to both partners together, and posttest discussion of how the couple wanted to approach HIV prevention going forward. The major addition to the African CHTC intervention was a component on skills building around sexual agreements. Agreements regulating whether and under what conditions sex outside the relationship is allowed are common for male couples, 15,16 but agreements are not always explicitly discussed and mutually understood within couples. 16 This article presents the results of a couple-randomized HIV prevention study to test the acceptability and safety of the adapted intervention.
Methods
Participants
Participants were recruited as couples to a randomized prevention study of CHTC versus individual voluntary HIV counseling and testing (iVCT). A multipronged recruitment strategy was employed, consisting of flyers displayed in community-based organizations and in retail locations in the Atlanta community; announcements on the website of AID Atlanta, a community-based HIV prevention and care provider; banner advertisements on Facebook targeting men who reported being in a relationship with another man; peer referral; and discussion with clients who walked into AID Atlanta seeking individual HIV testing. 17 All study visits took place at AID Atlanta regardless of recruitment method.
Couples were eligible to participate in the study if both members were male, at least 18 years of age, reported being a couple for at least 3 months, were willing to complete a follow-up study visit in 3 months, and were able to complete study assessments in English. The definition of a “couple” was left to participants’ interpretation and did not necessarily imply sexual monogamy or that the couple was yet sexually active. Exclusionary criteria for enrollment included either partner self-reporting being previously diagnosed with HIV, either partner being unwilling to accept randomization to the couples testing arm, and either partner planning to move from the Atlanta area within 3 months of the initial study visit. Men in eligible couples were provided with informed consent documents separately. The study was reviewed and approved by Emory’s Institutional Review Board (protocol #00043714).
Study Procedures
Couples were enrolled and completed all study procedures at a community-based organization (AID Atlanta). After being consented and enrolled in the research study, each participant separately completed a computer-administered baseline survey. The survey collected information on demographic and socioeconomic characteristics, dyadic characteristics (eg, duration of relationship), history of intimate partner violence (IPV), HIV testing history, and previous 6 months’ sexual history, both within and outside of the current partnership. For couples in which either partner reported recent history of IPV (by indicating an experience of being hit, kicked, physically hurt, or forced to have oral or anal sex in the preceding 3 months) or feeling coerced to test with his partner, a text message was sent to the study counselor informing him that the couple should not be randomized. In that case, the couple was informed that they would be tested individually through iVCT, with no reason given as to why this assignment was made. If no exclusionary criterion for randomization was reported by either partner, study staff opened a sealed envelope that contained the intervention group assignment. Couples were randomly allocated to either the CHTC or iVCT groups in a one-to-one fashion and within randomized blocks of sizes 2 and 4 to ensure balance of intervention allocation while retaining blinding of the randomization sequence. The randomization scheme was prepared by Rosenberg who had no direct role in study conduct, and thus study staff and participants remained blinded to the assignment until the time of envelope opening. Each participant was provided with an incentive of US$50 for participation in the baseline survey and counseling session, regardless of nonrandom assignment to iVCT or randomization.
Couples assigned to the CHTC arm were provided with a couples counseling and testing service adapted for use with male couples and based on the standard Centers for Disease Control and Prevention (CDC) couples testing protocol. Couples assigned iVCT were provided with standard prevention counseling and HIV testing, based on the standard CDC Fundamentals of Prevention Counseling protocol. Whether HIV results were returned separately or together, those with preliminary positive rapid test results were immediately referred for collection of blood specimens for confirmatory testing. At the end of the visit, participants in both arms were asked to complete a short questionnaire regarding their satisfaction with the session. The questionnaire included 7 items assessing the perceived quality, relevance, and usefulness of the session, whether the format was appropriate, the degree to which the session met personal needs, satisfaction, and likelihood of recommending the service to a friend. Responses were recorded as Likert-type scales ranging from 1 (poor/low) to 5 (excellent/high).
All participants were scheduled to return for a 3-month follow-up visit, and reminders were sent 2 weeks and 1 week prior to the scheduled visit. In the case where 1 or both partners indicated that they were no longer a couple, each individual was invited to return for follow-up separately. During follow-up visits, each participant completed a separate computer-administered survey that addressed sex with their main partner since the intervention, sex with outside partners, and any adverse outcomes following the intervention, such as dissolution of the partnership, relationship difficulties, conflicts, or IPV. Intimate partner violence was measured using items from the Revised Conflict Tactics Scales (CTS2), 18 with items representing physical (eg, hit, kicked, and punched) and sexual (eg, forced sex) violence selected to correspond to the baseline measure of IPV. Following completion of the surveys, all participants still in partnerships were offered a couples counseling session regardless of their original randomization arm.
Analysis
We sought to evaluate the acceptability and safety of CHTC. Acceptability was evaluated by comparing reported satisfaction with CHTC to satisfaction with iVCT; we report the median and interquartile range (IQR) for satisfaction and test for differences between individuals in the 2 groups using the Wilcoxon-Mann-Whitney test to account for the nonnormal distribution of the data. To evaluate the safety of CHTC, 2 couple-level outcomes were compared between study arms: the occurrence of IPV and relationship dissolution reported at follow-up. The occurrence of IPV was measured as the proportion of couples in which 1 or both partners reported perpetration or experience of IPV in the 3 months preceding the follow-up visit. To correspond to the indicators of violence used to screen couples out at baseline, selected items from the CTS2 were used. Couples were considered to have experienced physical IPV if either partner reported having been punched, hit, or kicked by the partner he tested with, injured to the point of feeling physical pain the day after a fight, or inflicting any of these acts on his partner in the preceding 3 months.
Relationship dissolution was reported as the proportion of couples in which either or both partners reported that the relationship had ended after their participation in the study. The reasons provided for relationship dissolution were also reviewed to identify cases in which relationship dissolution was possibly linked to the intervention. For both IPV and relationship dissolution, the proportions for the 2 intervention groups were compared using chi-square tests; P values <.05 were considered to be statistically significant.
Although evaluation of efficacy in reducing risk behaviors or HIV incidence was not a primary goal of this analysis and the study was not powered to measure efficacy, we conducted an exploratory analysis to compare the occurrence of couple-level recent (past 3 months) unprotected anal intercourse (UAI) at follow-up among couples that were determined to be HIV serodiscordant in their study testing. This is because UAI with the testing partner is particularly risky in serodiscordant partnerships. 19 For men who tested concordant negative, the principal risk behavior is sex with outside partners. Although unprotected sex with outside partners is a more telling indicator of risk, we did not have comparable indicators across study visits to assess changes in this specific behavior. As such, we examined the proportion of seroconcordant negative couples in which at least 1 man reported sex partners other than the testing partner at follow-up. Chi-square tests were again conducted to compare proportions across study arms. We did not include HIV-concordant-positive couples in the analysis of these behavioral efficacy outcomes because there were only 2 such couples, and we did not have power to detect behavioral changes among these couples.
Results
Enrollment and Randomization
As shown in Figure 1, 213 couples were screened for eligibility from September 2010 through December 2011. Of these, 113 (53%) couples were eligible, and all 113 enrolled in the study. Of the enrolled couples, 31 (27%) were ineligible for randomization due to reports of sexual or physical IPV (15, 13%), coercion (10, 9%), or both (6, 5%). In all, 18 (16%) couples were later excluded from analysis because they had been enrolled based on incomplete or inaccurate information: 4 (4%) had a previous diagnosis of HIV not reported to study staff at enrollment, 13 (12%) were judged not to be authentic couples based on contradictory responses to the questionnaire, and 1 (1%) had a previous HIV diagnosis and was judged not to be an authentic couple. Of these excluded couples, 4 had been randomized to CHTC, 6 to voluntary HIV counseling and testing, and 8 had been deemed ineligible for randomization due to reported IPV or coercion.
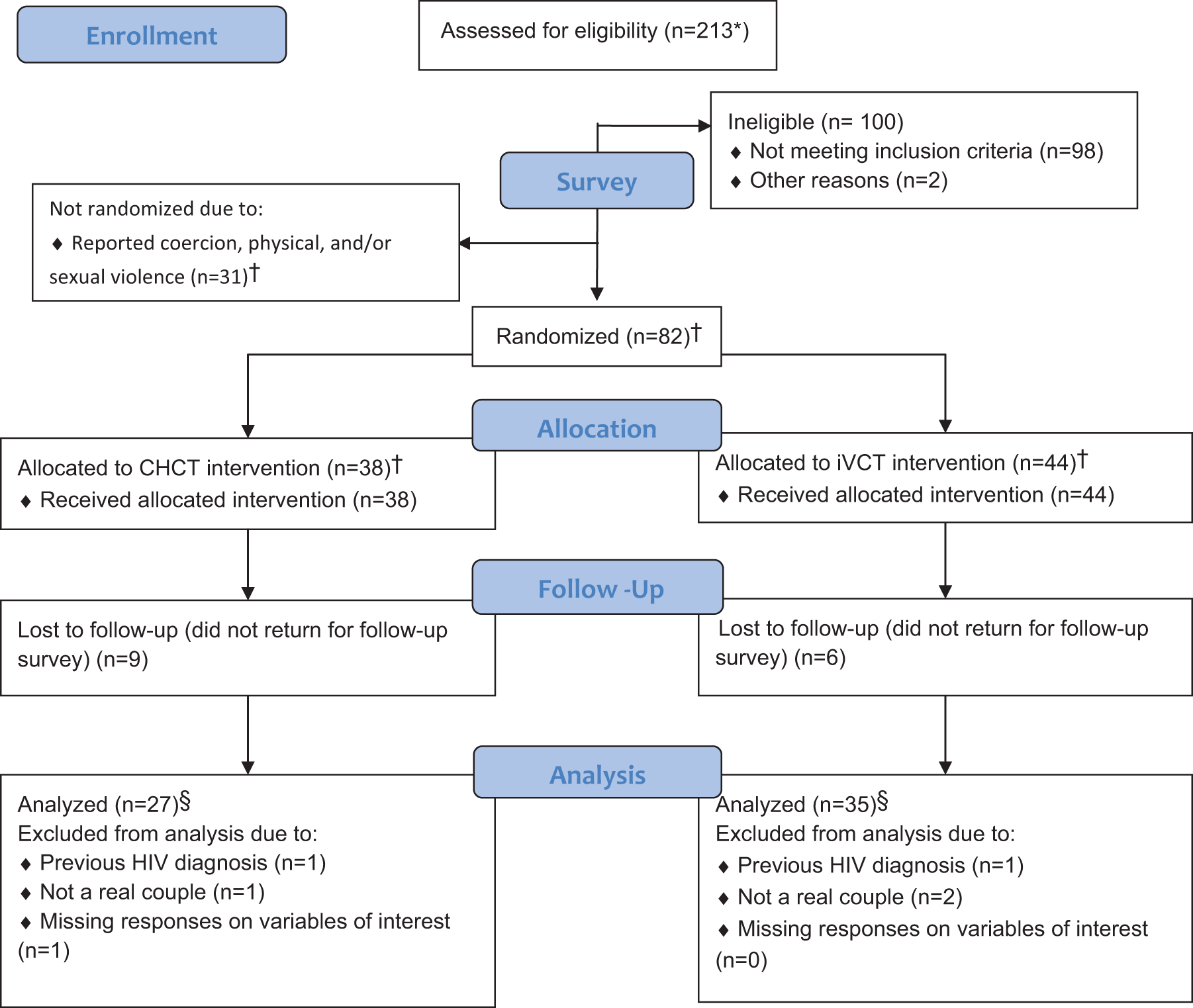
Recruitment, randomization, and inclusion of men who have sex with men (MSM) in a study of couples-based versus individual HIV testing and counseling, Atlanta, 2010 to 2011. *Sample sizes reported at the couple level. †These sample sizes include couples later determined to be ineligible because of a previous HIV diagnosis or inauthentic couple status—8 from the nonrandomized group, 4 from the CHTC arm, and 6 from the individual voluntary HIV counseling and testing (iVCT) arm. See text for details. §This analysis sample corresponds to the outcome of intimate partner violence (IPV). Samples for other outcomes varied depending on the number of missing responses on variables of interest and the subsample of analysis (ie, serodiscordant couples). These sample sizes are noted in the tables.
Demographic data of participants are presented in Table 1, and baseline characteristics of the dyads are presented in Table 2. There was no failure of randomization across any individual or dyadic characteristic. The modal age of the sample was in the 18 to 29 years age group, most participants were African American, and about half of the men had some education above the high school level. These demographics are largely reflective of the client base at AID Atlanta. Over a third of the men were nongay identified, and most were referred to the study by a community-based organization. The median duration of relationships among enrolled couples was 14 months. One or both partners in all but 6% of couples reported having had anal sex and over 60% reported engaging in unprotected anal sex with their main partner in the past year. In nearly half of the couples, at least 1 partner reported having 1 or more male sex partners outside the relationship, and in one-third of couples at least 1 partner reported UAI with a concurrent partner outside the relationship. Partners in 46% of couples reported differing agreements regarding sex outside of the relationship. As reported previously, 17 81% of the couples were found to be concordant negative, 17% were found to be serodiscordant, and 2% were found to be concordant positive.
Individual Demographics by Study Arm.a

Abbreviations: CHTC, couples HIV testing and counseling; iVCT, individual voluntary HIV counseling and testing; NA, not asked.
a We report data on the participants included in the final analysis data set, which comprised a total of 72 couples in the randomized arms and 23 in the nonrandomized cohort.
b Due to missing values, frequencies and percentages may not add up to the total.
c Chi-square test used to detect differences between the 2 randomization arms (CHTC and iVCT). Fisher exact test used where expected cell counts <5.
d Information on the method of recruitment not obtained from the nonrandomized group.
Couple Demographics by Study Arm.

Abbreviations: CHTC, couples HIV testing and counseling; iVCT, individual voluntary HIV counseling and testing; UAI, unprotected anal intercourse.
a Due to missing values, frequencies and percentages may not add up to the total.
b Chi-square test used to detect differences between the 2 randomization arms (CHTC and iVCT). Fisher exact test used where expected cell counts <5.
Participants in both arms had high levels of satisfaction with the counseling service they received (Table 3). No significant difference was found between the median satisfaction scores reported by men who received CHTC and men who received iVCT for any of the items or for the index.
Individual Satisfaction with the Baseline HIV Counseling and Testing Session, by Study Arm.

Abbreviations: CHTC, couples HIV testing and counseling; iVCT, individual voluntary HIV counseling and testing; IQR, interquartile range.
a Data reported by individuals, not by couples (4 respondents missing from each study arm).
b Wilcoxon-Mann-Whitney test used to compare mean scores across the 2 study arms.
c Higher scores indicate more positive opinions/perceptions. Possible scores range from 1 to 5 for all items except the index of opinions about the session (possible scores 5-35).
Prospective Assessment of Outcomes
Of the 144 individuals who completed the baseline procedures, 115 (80%) returned for follow-up. At least 1 partner from 62 (86%) of the initial 72 couples completed follow-up: 27 (79%) of the 34 couples in the CHTC arm and 35 (92%) of the 38 in the iVCT arm (P = .2 by Fisher exact test). The median time between baseline and follow-up visits was 4.1 months (IQR: 3.2, 5.8). Among participants assigned to CHTC, the median was 3.9 months (IQR: 3.4, 5.1), compared to 4.3 months (IQR: 3.0, 6.1) for the iVCT arm (Wilcoxon-Mann-Whitney P = .8).
Safety
Data on the perpetration or experience of IPV were provided by 1 or both partners in all 62 couples that returned for follow-up: 27 (79%) CHTC couples and 35 (92%) iVCT couples (Table 4). Of these, a total of 6 (22%) couples in the CHTC arm and 6 (17%) in the iVCT arm reported IPV in the 3 months preceding the follow-up visit (P = .6).
Proportion of Couples Reporting IPV and Relationship Dissolution at Follow-up, by Study Arm.

Abbreviations: CHTC, couples HIV testing and counseling; iVCT, individual voluntary HIV counseling and testing; IPV, intimate partner violence.
a Data reported at the couple level.
b Of the 62 couples from which 1 or both partners provided follow-up data, 1 did not provide answers to the questions on relationship dissolution.
Of the 61 (85%) couples from which at least 1 partner provided data on the status of the relationship at follow-up, 11 (42%) couples randomized to CHTC were reported to have ended the relationship compared to 18 (51%) couples assigned to receive iVCT (P = .5; Table 4). Participants who indicated that their relationship had ended were asked whether they thought that the study had anything to do with the breakup. Two participants responded “yes” to this question, both of whom were in the iVCT group. These participants elaborated that the study helped them identify preexisting issues with their relationships: “The study caused me to ask additional probing questions…” and “It opened the conversation between me and him up to see that we were both on two different pathways in life and what we wanted.”
Exploratory Analysis of Efficacy
From among the 11 randomized couples that were identified by study testing as serodiscordant, data on UAI with the main partner during the 3 months before the follow-up visit were obtained from 1 or both partners in 9 (82%) couples—4 in the CHTC arm and 5 in the iVCT arm. No member of a couple in either study arm reported UAI with the serodiscordant partner they tested within the past 3 months.
Focusing on outside sex partners among seroconcordant negative couples, at least 1 partner from 51 (86%) of the 59 couples who were found to be seroconcordant negative at baseline provided data on sex with outside partners during the 3 months before the follow-up visit (Table 5). Among couples in the CHTC arm, 39% reported outside partners at follow-up; 46% of couples in the iVCT arm reported outside partners (P = .6).
Presence of Outside Sex Partners in the Preceding 3 Months among Seroconcordant Negative Couples Reported at Follow-up, by Study Arm.

Abbreviations: CHTC, couples HIV testing and counseling; iVCT, individual voluntary HIV counseling and testing.
a Data reported at the couple level.
Discussion
We report results from a randomized prevention trial about the acceptability and safety of CHTC for male couples in Atlanta. Based on these results, we conclude that CHTC is a highly acceptable prevention service for MSM and that there is no evidence of important potential harms—new IPV or relationship dissolution. This suggests that further expansion of CHTC for male couples is safe, warranted, and acceptable to men. Formative work has also demonstrated high levels of willingness to use CHTC among US MSM, 20,21 especially among couples with higher levels of relationship satisfaction and commitment to sexual agreements. 22 However, the current study was not powered to demonstrate efficacy of the intervention for behavioral outcomes or reduction in HIV or STI incidence, and ongoing evaluation of key outcomes will be important as scale-up of the service in the United States occurs.
Intimate partner violence is at least as common among North American MSM as among heterosexual women, 23 –26 and in our discussions with prevention providers and stakeholders leading up to the adaptation of the intervention for US MSM, we heard frequent concerns that couples testing services might incite IPV. Counselors who deliver the CHTC service are trained to use specific approaches to defuse tension and ease blame during CHTC sessions, and as a part of this study we made arrangements for couples in the study to access a family therapist if conflict arose within the session that the counselor did not feel comfortable handling. Only 1 referral to the family therapist was made for study participants. Our finding of no increased incidence of IPV among couples tested together is consistent with reports from male–female couples in Africa, where the great majority of men and women testing together did not report IPV. 27
However, there are some important caveats to our findings about IPV. First, we restricted enrollment in our study to couples where neither partner reported a recent (3 months) history of physical or sexual IPV as defined by our screening questions. Therefore, our findings can only be applied to couples without recent physical or sexual IPV in their relationship. It is possible that, for couples with a history of recent IPV, CHTC could be associated with a higher occurrence of further IPV, compared to iVCT. It is notable that, even among our IPV-free couples, there was a measurable amount of new IPV among all couples, regardless of whether or not they were tested for HIV as a couple. The observed incidence of IPV points to the importance of sensitizing counselors to the issue of IPV among male–male couples and highlights the need for further research to understand the factors and experiences that trigger violence among male–male couples. A recent study by Were et al 27 observed that HIV-positive people in East and Southern Africa were more likely to report experience of IPV than their HIV-negative counterparts; in our study, there were not enough HIV-positive participants to calculate stable status-stratified rates. Future evaluations of CHTC should include couples with a history of IPV for evaluation of whether CHTC potentiates recurrent IPV, and as experience with larger numbers of HIV-positive men accrues, HIV-status stratified estimates should be developed.
Satisfaction with HIV testing and counseling was high in both arms. In this study, the same study counselor (J.B.) provided counseling to most men regardless of their randomization, and it is likely that this measure is a reflection of the quality of his counseling as well as the format (ie, couples or individual) in which the service was provided. Our high levels of satisfaction are consistent with those recently reported in another randomized study of an enhanced counseling intervention for MSM. 28 The high satisfaction with the service is also consistent with our preliminary qualitative studies, which suggested high levels of enthusiasm for testing together with a male partner among MSM with main partners, 21 and with preliminary survey work, which suggested high levels of interest in testing with partners. 20
Rates of relationship dissolution were not different by study arm but were high overall: nearly half of the couples who participated in the study reported having ended their relationship at follow-up. However, only 2 of the 29 couples reporting dissolution attributed their relationship ending to having tested together, and both of those men received iVCT. Despite the relatively long duration of relationship at baseline (median 14 months), this may simply reflect lability of main partnerships, especially among younger men (our modal age was in the 18-29 years group).
Although our study was not powered to detect efficacy for self-reported behavioral outcomes, exploratory analyses provided some interesting findings. We note that among the 9 couples that were found to be HIV serodiscordant during baseline testing and who provided follow-up data, none reported UAI in the 3 months between having learned about their discordant status and returning for the follow-up visit. Although the lack of UAI was the same in couples tested together or separately, we believe that the fact that couples came to the study and submitted to the possibility of randomization to testing together, and the fact that the couples who were randomized to be tested separately were tested on the same day and in the same location, made it likely that post-iVCT discussion of test results occurred. Regardless, the finding of reported universal uptake of condoms for anal sex after diagnosis of serodiscordance suggests that informing a couple of serodiscordance may provide HIV prevention benefits, at least in the short term. Among men in couples who received concordant negative results, there was no difference in reported anal intercourse partners outside the relationship by study arm. Because of a technical survey error in which follow-up questions about UAI with outside partners did not unambiguously identify which partner was being asked about, we were concerned that there might be serious misclassification in the UAI data with outside partners and chose not to report those data as part of the exploratory analyses.
Our study has important limitations. First, our study was conducted only in Atlanta, and our results might not apply to male couples in other parts of the United States or the world. However, our recent evidence suggests high levels of willingness to use CHTC among MSM worldwide. 20,29,30 Compared with a recent, larger sample of male couples, 16 the couples in our study reported a higher extent of not agreeing on the terms of their sexual agreements; this might be because couples in Atlanta are different than the national sample of Mitchell, or because we or he had other biases that led to misclassification. Second, although our randomization was successful with respect to individual and couple characteristics, we had some (nonsignificant) degree of lower follow-up reporting from couples randomized to CHTC versus iVCT. This might have introduced differential selection bias to our follow-up data. If couples who were tested together were systematically more likely not to complete follow-up surveys that might indicate lower satisfaction with the original service or more (unreported) negative outcomes after the service. However, we assessed satisfaction with the original service during the baseline visit, so we do not believe that lower follow-up rates were the result of lower initial satisfaction. We are also aware that social desirability bias might impact our reporting of satisfaction (presumably favoring higher satisfaction) or of IPV (presumably favoring lower reporting of perpetration, and perhaps experience, of IPV). Our study was not designed or powered to measure efficacy for self-reported behavioral outcomes.
Despite these limitations, our study provides important information as part of a systematic and progressive evaluation of the adapted CHTC service for male couples in the United States. Formally assessing acceptability and safety are key steps in deciding whether an intervention should move forward for further programmatic scale-up or further research. There is currently great attention to HIV testing as the gateway to clinical evaluation and viral suppression. 31 At the same time, CDC recommends that MSM at high risk for HIV should test for HIV more often than annually. 32 Centers for Disease Control and Prevention also recognizes CHTC as a high-priority HIV prevention strategy for the United States and is supporting training, implementation, and technical assistance for all types of couples (personal communication, Kristina Grabbe, CDC, May 29, 2013). The CHTC service is also consistent with National HIV/AIDS Strategy goals 33 and has been supported for dissemination through CDC’s MSM Testing Initiative and the Enhanced Comprehensive HIV Prevention Planning (ECHPP) Project.
After testing separately for HIV, in about one-third of sexual partnerships, including those with regular partners, men do not discuss their HIV status with their partner before first sex. 34 In this context, we believe that developing a diverse set of HIV testing options that are congruent with men’s life situations is critical. Couples HIV testing and counseling represents a highly acceptable means of promoting testing for MSM, of addressing disclosure of HIV status, and of supporting male couples to plan together to manage critical issues in their lives, including the risks or realities of HIV, expectations about sex and sexual risks, and expectations about broader relationship issues.
At this time, CHTC is supported as part of routine HIV prevention services in PEPFAR countries, and PEPFAR recommends considering CHTC for male couples in PEPFAR countries. 13 Currently, a number of public health agencies and community-based organizations are scaling up CHTC for male couples in the United States, based on the decades of experience with CHTC in Africa, the urgency of addressing HIV testing needs in male couples, and the preliminary evidence of acceptability and safety. We recommend that, to the extent possible, further evaluations of key elements of CHTC (eg, safety, acceptability, prevalence of serodiscordance in different service settings, and surveillance of adverse outcomes) be conducted. Such evaluations would be facilitated by the addition of a data element to document provision of a couples testing service in routine reporting systems for publicly funded HIV-testing programs, and we call on CDC to develop such a reporting element. It is also possible that additional data from randomized studies of CHTC in male couples could come from other types of research studies, such as implementation science studies of how testing couples together impacts subsequent access to care and treatment for HIV, adherence, and other prevention-relevant outcomes.
Footnotes
Acknowledgments
We thank AID Atlanta for providing space for the research activities, and Adam Carpenter for editorial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (grant number R34-MH086331), the Emory Center for AIDS Research (grant number P30-AI050409), and the MAC AIDS Fund.