
Abstract
Objectives:
Strengthening HIV testing uptake is critical to curtail the HIV epidemics among men who have sex with men in the United States. Despite the implementation of various interventions to promote HIV testing among men who have sex with men, few aggregated evidence is presented to reflect the “lessons learned” and inform future directions. The objective of this systematic review is to comprehensively summarize published studies that described, tested, and evaluated outcomes (e.g. efficacy, effectiveness, acceptability, feasibility and/or qualitative opinions) associated with an HIV testing intervention and identify gaps as well as opportunities to inform the design and implementation of future interventions to enhance HIV testing uptake among men who have sex with men in the United States.
Methods:
We followed the PRISMA guidelines and conducted a systematic review of articles (published by 23 July 2021) by searching multiple databases (PubMed, MEDLINE, Web of Science and PsycINFO).
Results:
Among the total number of 3505 articles found through multiple databases, 56 papers were included into the review. Interventional modules that demonstrated acceptability, feasibility and efficacy to improve HIV testing uptake among men who have sex with men include: HIV self-testing, interpersonal-level (e.g. peer-led, couple-based) interventions, personalized interventions and technology-based interventions (e.g. mHealth). Aggregated evidence also reflects the lack of individualized interventions that simultaneously address time-varying needs across multiple socioecological levels (e.g. individual, interpersonal, community, structural and societal).
Conclusion:
Development of interventions to improve HIV testing rates and frequency of men who have sex with men has proliferated in recent years. Our review presents important implications in sustaining and improving interventions to address HIV testing uptake among men who have sex with men in the United States.
Introduction
Men who have sex with men (MSM) bear a disproportionate burden of HIV in the United States, accounting for 69% of the 36,000 new HIV diagnoses and almost 90% of diagnoses among males in 2019. 1 Compared to their White counterparts, Black and Hispanic/Latino MSM continue to be disproportionately affected by HIV.1 –4 The challenges of HIV prevention in MSM are further compounded by their low self-perceived risk for HIV infection, suboptimal pre-exposure prophylaxis (PrEP) use and HIV testing uptake, condomless sex, multiple sex partners and social stigma about HIV and/or their sexual orientation and identity.5 –9
HIV testing is the entry point into the HIV care cascade. HIV testing is also a requirement and core component for PrEP (initiation, continuation), and test-and-treat. The expansion of HIV testing and early initiation of these biomedical HIV prevention strategies is critical to curtail the epidemic among HIV-affected populations. 10 In addition, awareness of HIV status was reported to be significantly associated with greater condom use, through which onward transmission of HIV could be prevented.11,12 In addition to conventional facility-based HIV testing, different testing modalities including rapid home self-testing (an oral fluid test with rapid provision of testing results), mail-in self-test (dried blood self-collection from a fingerstick for laboratory testing) and couples HIV testing and counseling (CHTC, a couple-based HIV testing service called Testing Together) have been designed and implemented for MSM in the United States to facilitate testing uptake among this subgroup.
Despite the proven HIV prevention benefits and increase in accessibility, HIV testing uptake remains suboptimal among MSM in general. A meta-analysis conducted among Internet-using MSM suggested that only 58% had tested for HIV in the prior year. 13 The prevalence of HIV testing among same-sex male couples was even lower, where no more than 30% of them had gotten tested for HIV every 6 months. 14 Low HIV testing rates among MSM in the United States could be attributed to a variety of factors at multiple levels, including individual (e.g. lack of knowledge on testing locations, fear of a positive result and worries about confidentiality), interpersonal (e.g. lack of support), institutional/policy (e.g. lack of financial support for HIV testing programs) and social-cultural (e.g. stigma and discrimination) levels.15 –19
The number of behavioral and structural interventions aimed at improving MSM’s engagement in HIV testing has increased since 2005. One of the early randomized controlled trials (RCTs) was “Many Men, Many Voices” with Black MSM residing in New York City. 20 This intervention aimed to improve their knowledge of and attitudes toward HIV and address structural barriers to testing such as racism and homophobia. Participants were observed to have greater odds of HIV testing compared to the waitlist comparison condition (odds ratio (OR) = 1.81, 95% confidence interval (95% CI): 1.08–3.01). 20 The limitations of the study included the cost associated with organizing an intervention retreat and diminished retention rate across study periods.
More novel psychobehavioral interventions (e.g. couple-based, social media, behavioral economics, peer-driven) had also been designed and implemented targeting MSM to enhance their HIV testing uptake. While these interventions were successful to promote HIV testing among MSM in a defined period of time, they also have had various levels of limitations in generalizability and sustainability post the intervention period.20 –26
Despite an increasing body of literature in designing and evaluating interventions to promote HIV testing,27 –29 few in-depth, systematic summary of the contents, opportunities, strengths and limitations of these interventions is presented for MSM in the United States. The aggregated evidence from existing interventions with a goal to increase HIV testing uptake among MSM may provide prevention scientists with important information regarding which intervention components, modalities and frameworks may work best for various subgroups of MSM; equally important, what interventional aspects may need to be further strengthened to better enhance HIV testing for MSM in the United States. To this end, the objective of this systematic review is to comprehensively summarize published studies that described, tested, and evaluated outcomes (e.g. efficacy, effectiveness, acceptability, willingness, feasibility, barrier/facilitator, and/or qualitative opinions) associated with an HIV testing intervention, and identify gaps as well as opportunities to inform the design and implementation of future interventions to enhance HIV testing uptake among MSM in the United States.
Methods
Literature search strategy
This systematic review was conducted by searching published articles via multiple databases (PubMed, MEDLINE, Web of Science and PsycINFO) published by 23 July 2021, following the PRISMA guidelines (see supplemental material—PRISMA Checklist). 30 The final search terms included: (“gay” OR “men who have sex with men” OR “bisexual” OR “homosexual” OR “homosexuality” OR “same-gender-loving” OR “sexual minority”) AND (“HIV” OR “human immunodeficiency virus”) AND (“testing” OR “test” OR “diagnosis” OR “screening”) AND (“intervention” OR “trial” OR “experiment” OR “randomized” OR “pre-post”). We also conducted cross-referencing by reviewing the reference list of the included studies to identify potential papers for consideration.
Inclusion/exclusion criteria
Generally, studies were included in the systematic review if they met the following criteria: (1) published journal articles excluding abstracts or conference proceedings; (2) conducted in the United States; (3) this study and/or the parent trial was based on an experimental or quasi-experimental design (e.g. RCT, one-group pre-post) to test an HIV testing intervention; (4) reported HIV testing–related outcomes (e.g. efficacy, effectiveness, acceptance, intention and willingness) with relevant determinants (e.g. any demographic, behavioral and psychosocial factors); (5) conducted among participants identified as gay, bisexual and other MSM in the original studies; and (6) published in English.
To achieve our goal of comprehensively summarizing the content, scope and factors affecting the implementation of HIV testing interventions for MSM, we also included the following studies for potential evaluation: (1) studies conducted among mixed population groups (e.g. MSM and other sex and gender minorities) if data were reported separately for MSM; (2) studies that used an experimental design to evaluate secondary outcomes (e.g. acceptability, feasibility or cost-effectiveness) with or without reporting efficacy/effectiveness; (3) studies using non-experimental design (e.g. qualitative or cross-sectional study) to assess aforementioned secondary outcomes of an HIV testing intervention if details about the intervention design could be retrieved from their published parent trials by checking the reference lists; (4) we also included protocols that elaborated the design and conceptual frameworks to supplement our summary of the original HIV testing interventions. Any existing reviews, meta-analyses or articles that commented on an existing HIV testing intervention were not included in the current review. We also excluded studies that described the development or adaptation of eligible interventions.
Statistical analysis
All articles identified through database search were stored and managed using a reference management tool (EndNote X9). Titles and abstracts of all identified records were first screened for relevancy and duplicate removal by two independent reviewers (Y.W. and Y.L.). The full-text review and data extraction were then conducted independently by one author (Y.W.) and further cross-checked by the other author (Y.L.) for accuracy. Disagreements were iteratively discussed until agreement was reached. A standardized Excel sheet was used to extract the following information from eligible articles: study location, study/recruitment period, study design, recruitment strategy, participant characteristics, intervention content, theoretical/conceptual framework, barriers to HIV testing addressed by the intervention, control, sample size and retention, HIV testing–related outcome measures and findings (e.g. acceptability, feasibility, cost-effectiveness and efficacy).
Methodological quality assessment
The quality of each study was assessed independently by one author (Y.W.), following the guidance for study assessment. 31 The other author (Y.L.) further cross-checked the appraisal for accuracy. Conflicts in appraisal were resolved through iterative discussion until agreement was reached. The methodological quality of included studies with a control group was evaluated using National Heart, Lung, and Blood Institute (NHLBI) quality assessment tool of controlled intervention studies.31,32 This assessment tool was comprised of 14 questions, which evaluated selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and intervention providers), detection bias (blinding of outcome assessors), attrition bias (drop-out), information bias (measurement of outcomes) and other sources of bias. We rated yes, no, cannot determine, not reported or not applicable for each criterion. For example, if authors reported method of randomization, but we were unable to determine whether the randomization was adequate and would respond “cannot determine” to this criterion. If authors did not mention the method of randomization, we scored “not reported” for this criterion. The remaining pretest–posttest studies were similarly assessed using NHLBI quality assessment tool for before–after (pre–post) studies with no control group. Two assessment tools have been described in detail elsewhere. 31
Results
Search results
A total number of 3505 articles were found through multiple databases. Of 73 full-text papers assessed for eligibility, 56 papers representing 42 interventions were included into the final review. Thirty-seven papers evaluated the acceptability, feasibility, efficacy or cost-effectiveness of interventions aimed at improving MSM’s uptake of HIV testing. Seventeen articles described the protocols for the implementation of interventions. Study selection process was reported in Figure 1.

Flowchart of study selection and inclusion procedure.
Study characteristics
Table 1 presented the characteristics of 42 interventions identified from 56 included publications. Reported study locations/settings in the United States included Oregon, 33 New York,20 –22,44,55,68 –70,73 California,25,34,36,45,46,50,54,55,60 –63,74,75 Michigan,35,38,54,65,73 North Carolina,24,49,80 Washington,39,59 Georgia,25,41,53 –55,73 Illinois,25,47,54 Pennsylvania, 53 Texas,53,55 Tennessee, 54 Louisiana,23,54 Maryland, 55 Massachusetts,68 –70 Nevada, 23 Florida, 23 Minnesota 23 and D.C.54,55 Nine studies were conducted nationally.26,43,51,52,57,58,64,71,76,78,79 Most studies were implemented after 2000.20 –26,34 –37,39 –79,81
Summary of study characteristics.

MSM: men who have sex with men; HIV: human immunodeficiency virus; RCT: randomized controlled trials; MV: many voices; OR: odds ratio; CI: confidence interval; CDC: Centers for Disease Control and Prevention; HOPE: harnessing online peer education; STD: sexually transmitted diseases; PS: partner services; AIDS: acquired immunodeficiency syndrome; TMUS: testing makes us stronger; IO: information only; IP: information plus; SUP: status update project; HMP: HealthMpowerment; SSE: SMART sex ed; TW: transgender women; PEP: primary eligible participant.
Nine RCTs are still ongoing.43,53,54,65,71,74,78,79,81 Thirty-one interventions were evaluated by RCTs.20,21,23,26,35,36,38,42 –44,49 –51,53,54,57,59,64,65,67,68,71 –76,78 –81 Eleven studies were evaluated by using a quasi-experimental design;24,25,33,34,39,41,45,47,55,60,61 5 of the 11 used a pretest-posttest design.24,25,41,47,55
Regarding recruitment, offline/in-person approaches ranged from outreach (e.g. at local venues, communities, LGBT health care organizations and sexual health clinics), advertisements placed in communities, venues, and print media frequented or used by MSM, to referrals from other participants, friends of participants, and clinicians.20,21,25,34,36,38,44,45,47,49,50,57,59,61,65,66,68,72 –75,78,81 Peer recruitment within their social networks or venues-based peer outreach were also reported.35,60,80 Online recruitment included advertisements placed on gay-oriented sexual networking websites, social media sites and social magazines.21,23,26,36,38,41,43,44,45,47,49 –51,53,54,57,59,64 –66,68,71 –73,75,76,78,79,81 Participants were MSM only,20,23,24,26,35,36,38,39,43,45,47,49 –51,53 –55,57,59,60,64,66,68,71 –73,75,76,78,79,81 or a mixture of MSM with other populations (e.g. heterosexual IV drug users, women or transgender people).21,25,33,34,41,42,44,61,65,74,80 Of note, some studies targeted Black,20,25,35,44,50,55,60,75,78 Latino25,34,49,60,61,78,80 and young MSM.25,35,38,43,45,51,53,54,57,64,65,68,71,72,78,79
Methodological quality assessment
Methodological quality assessment for studies with and without a control group was summarized in Tables 2 and 3, respectively. Of 37 controlled intervention studies, one study received a score of 11 and were considered good quality, and 24 received a score of 5 to 10 and were considered fair quality. Twelve studies received a score of <5 due to the non-randomized design or lack of evaluation data (i.e. protocols). Five pretest–posttest studies had a mean score of 5.8 (standard deviation = 1.30). All five studies had clear objectives, well-defined interventions that were consistently applied to the participants, and appropriate statistical analyses.
Quality assessment of controlled intervention studies.
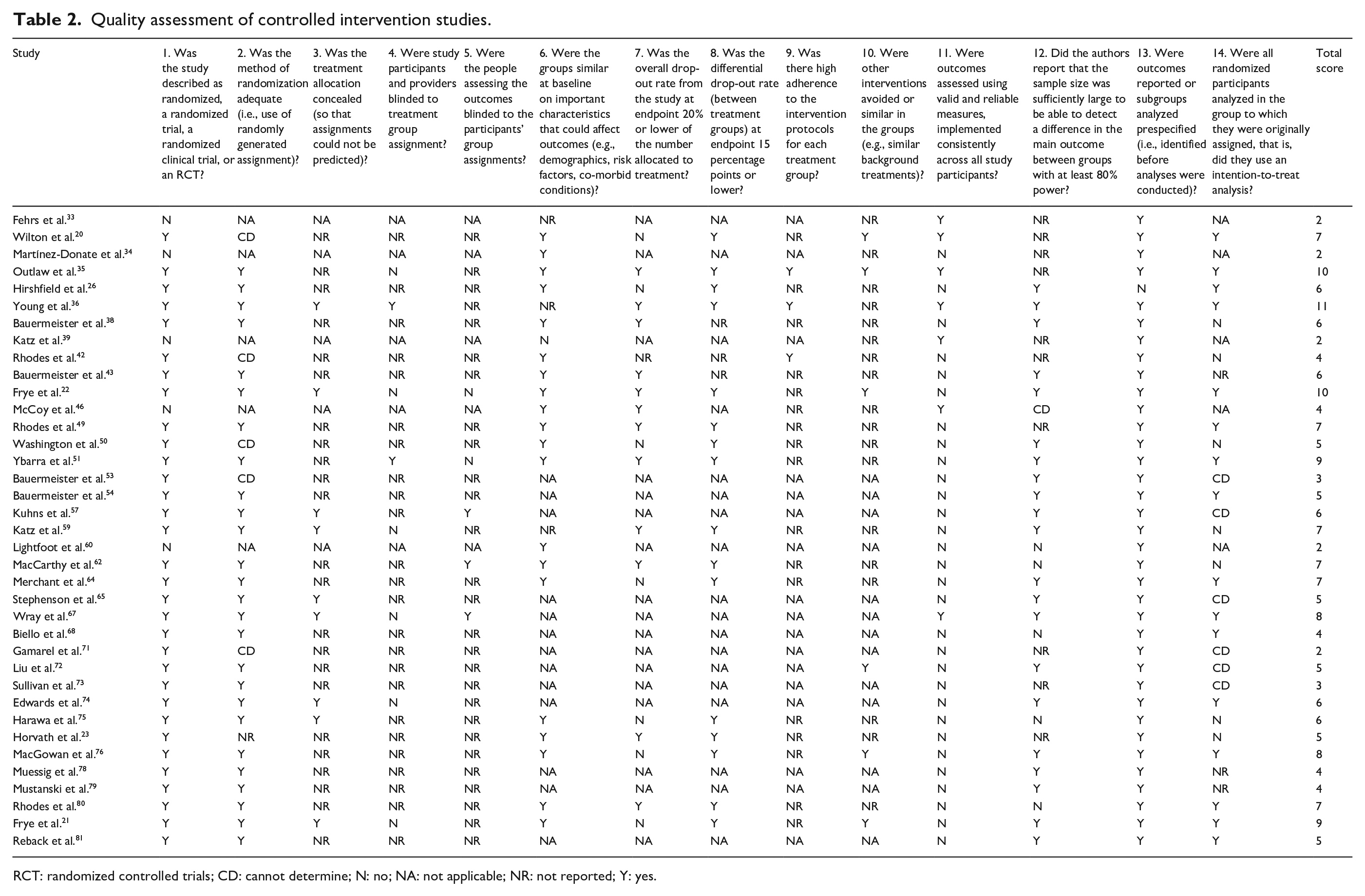
RCT: randomized controlled trials; CD: cannot determine; N: no; NA: not applicable; NR: not reported; Y: yes.
Quality assessment of pretest-posttest studies.

CD: cannot determine; N: no; NA: not applicable; NR: not reported; Y: yes.
Measurement of outcome
Knowledge of HIV testing 72 and testing locations 34 as outcome measures were reported. Attitudes toward HIV testing were measured by motivation to receive testing on a 5-point Likert-type scale 47 or willingness to refer other MSM to get tested for HIV. 64 Behavioral outcomes included self-reported HIV testing behavior (yes/no),20,21,24 –26,34,35,38,39,42 –44,49 –51,54,57,61,67,68,73 –75,78 –81 number of tests59,60,72,76 and repeat testing (two or more tests over time)23,45,53,65,71,78 during the follow-up. Other less-reported behavioral outcomes included demand for HIV testing,33,36 scheduling an appointment to test for HIV, 38 returning or following up for test results35,36 and referrals of other MSM to test for HIV. 64 Only one study evaluated the intervention by measuring the structural (e.g. transportation and distance to testing site) and psychosocial barriers (e.g. fear of testing HIV positive and HIV stigma) to HIV testing rated on a 6-point Likert-type scale. 41 For interventions focused on HIV self-testing (HST), self-efficacy toward testing (confidence in ability to test) was reported. 68
Theoretical framework
Key elements of theoretical underpinnings guided most studies to address psychosocial factors (e.g. perception, motivation, stigma, and social support), improve HIV knowledge and deliver risk reduction skills training. Commonly reported theoretical frameworks included social cognitive theory,20,24,42,44,49,65,68,73 –75,80 empowerment education,21,24,42,49,80 information motivation behavior model,23,47,51,71,72,79 motivational interviewing principles,21,35,53,65 self-determination theory,38,45,53,65 integrated behavioral model,38,43,53,78 model of behavior change,20,50,65 social-ecological model,21,34 social learning theory26,57 and social support theory.21,80
Intervention strategies and findings
Of 42 interventions reviewed in this study, most common interventions were HST interventions, interpersonal-level interventions, personalized/individualized interventions and technology-delivered interventions. The vast majority of these interventions were developed from 2016 and onward. The types of interventions in this study were not mutually exclusive (e.g. an interpersonal-level intervention might incorporate personalized elements). Hence, the types we presented here were used to provide the readers with examples of various interventions.
Interventions for HIV self-testing
Generally, for interventions aimed at promoting HST, participants received information on HST and self-administration of the testing via social media groups, video chat, mobile app, online videos or peer educators. Then they received or requested the test kits from the research teams or ordered the kits online.21,36,41,59,68,76 As an emergent tool for HIV screening, HST was proved to be highly acceptable, feasible, efficacious and cost-effective.21,36,41,59,70,76,77 In the “HOPE” study, participants who were delivered information on HIV testing had high acceptance across assessment periods and were more likely to request an HIV testing kit compared to those who received general health information (43.9% vs 20.0%). 36
There were two studies evaluating the effect of testing kits distribution strategies on the uptake of testing, which were social network distribution 60 and online purchase by participants. 64 We additionally identified an intervention providing counseling and referral of needed services after participants performed self-testing.66,67 All of these interventions exhibited efficacy in promoting HST among MSM.60,64,66
Interpersonal-level interventions
There were two couples-based interventions for MSM, “2GETHER” and ongoing “We Prevent.” Both interventions delivered sessions about communication skills and CHTC.47,71 “2GETHER” additionally discussed minority stress, relationship stress and utilization of social and community support. 47 This study demonstrates feasibility, acceptability and preliminary efficacy among young male couples. 47
Most interpersonal-level interventions were peer-mentored or peer-led. Peers, who shared sociodemographic characteristics with participants, delivered information on HIV testing, provided support or directly distributed HST kits to MSM.35,36,41,54,60,74,75,80 Peer-mentored interventions were efficacious in reducing barriers to HIV testing, promoting uptake of testing and returning for testing results.35,36,41,60,75,80 The “HOLA” intervention targeted Latino MSM, and participants who received help from peer leaders had more than eight times the odds of getting the test at 12 months compare to those assigned to the general health education comparison group (OR = 8.3, 95% CI: 3.0–23.0). 80
We identified two interventions that friends participated in together, “HealthMpowerment 2.0” and “TRUST.”21,78 In the “HealthMpowerment 2.0,” participants invited their friends to join the study via the mobile app, but they had no access to detailed information of enrolled friends. 78 In the “TRUST” study, however, friend pairs engaged in HIV testing and intervention sessions together. Evidence suggested that friend pairs were more likely to receive HST during the study period. 21
Social campaigns
We observed two campaigns, “Hombres Sanos” [Healthy Men] and “Testing Makes Us Stronger” (TMUS). The elements of “Hombres Sanos” campaign included print materials, radio advertisements and community-based outreach. Favorable changes in HIV testing among Latino MSM were not observed for “Hombres Sanos.” 34 The TMUS incorporated more Internet-based components such as online advertisements, a dedicated website and social media outreach. The number of HIV testing among Black MSM in the implementation cities of TMUS was found to increase at a rate of 6.22 tests per month (95% CI: 2.31–10.12). 55
Structural interventions
In 1986, Oregon began offering anonymous HIV counseling and testing services in which numbers were used to identify clients. It is reported that the availability of anonymity increased HIV testing among gay men by 125%. 33 Another structural intervention was the integration of HIV testing into sexually transmitted diseases (STD) partner services (PS) program in Washington State. 39 This program was highly effective in promoting HIV testing (63% pre-intervention to 91% during) among MSM with an STD and was also cost-effective.39,40
Personalized/individualized interventions
Personalized interventions were developed by customizing the content based on participants’ self-reported information (e.g. demographic characteristics, sexual behaviors, psychosocial factors and prior HIV testing experiences). Most personalized interventions were aimed to improve individual-level information (e.g. HIV prevention information and HIV risk assessment), motivation (e.g. HIV testing reminder, risk reduction and wellness plan, guidance from mentors) and behavioral skills (e.g. safer sex skills).38,41,43,53,54,65,68,72 –75 Individualized interventions were found to be acceptable, feasible and efficacious in enhancing HIV testing among MSM.38,41,70,75
At the structural level, two interventions, “Get Connected” and “Get Connected 2.0,” employed tailoring to link participants to the HIV testing sites that were most appropriate to their needs (e.g. privacy, confidentiality and clinic environment).38,53 The “All About Me” intervention provided a personalized recommendation of an optimal HIV testing approach (HST, facility-based testing or CHTC) for participants.22,44 “All About Me” improved HIV testing among Black MSM during follow-up compared to the non-tailored control (75.9% vs 70.9%), although the difference was non-significant. 22
Technology-delivered interventions
Development and evaluation of technology-delivered interventions exploded from 2010 and onward. Different from venue-based interventions, participants received intervention content including HIV prevention, HIV testing and sexual risk reduction information through online videos, text messages, websites, web apps or social media.26,38,50,51,53,76 We additionally identified interventions providing online consultation to participants. In these studies, well-trained counselors provided social support and information on HIV testing or assisted participants in setting health goals via chat room, video chat or social media.24,36,41,42,54,71,79 Technology-delivered interventions for HIV testing were shown to be acceptable, feasible, efficacious, and cost-effective among MSM.24,36,38,41,42,50 –52,76,77
Most interventions delivered via text message, web app or mobile app provided not only information on HIV and local resources (e.g. HIV testing sites, PrEP clinics and community events), but online interactive activities to boost participants’ engagement. Commonly reported activities were individual risk assessments, setting health goals, using sexual diaries, and engaging in forums, polls, games, and/or quizzes.23,43,54,57,61,68,72 –74,78,81 In addition, participants could directly order prevention commodities (e.g. HST kits, mail-in self-tests or condom variety packages) and follow-up on unreported HIV test results through the apps.68,72,73,78 For participants who tested positive during the study, information on referral and linkage to HIV services in the local communities were provided.72,78 Efficacy of technology-delivered interventions was unclear because most studies were ongoing.43,54,73,74,78,81
Of note, we observed one intervention, “Stick to it,” incorporating both online and offline activities. Participants were encouraged to earn points through online activities, such as taking the quizzes and monitoring their plans for HIV screening. Offline activities occurred at health clinics where participants could receive HIV screening and redeem their points for prizes. 45 The pilot test reported that participants in the intervention group were more likely to repeat an HIV test over the 6 months of follow-up (OR = 2.15, 95% CI: 1.03 - 4.47). 46
Comparison of evaluation of interventions
Evaluation of acceptability and feasibility was mostly conducted in technology-delivered interventions.23,36,38,41,46,47,51,63,70 Participants generally had positive attitudes toward the interventions delivered by website, video or text messages, for example, “I liked the whole goal of the program (Guy2Guy intervention),” and expressed high satisfaction with the program.38,41,46,51 Mobile app interventions were also shown to be acceptable based on the high System Usability Scale score. 70 In terms of feasibility, these programs were able to recruit and retain diverse participants in their interventions.38,41,46
All types of interventions demonstrated efficacy to improve HIV testing uptake among MSM, including increased HIV counseling and testing, repeat HIV testing, and less barriers to HIV testing.20,21,24,25,35,36,38,41,46,49,51,55,58,66,76,80 Of note, two peer-delivered interventions, “HOLA” and “HOLA en Grupos,” reported more than eight-fold increase in HIV testing among Hispanic/Latino MSM.49,80 Few interventions reported non-significant improvement in primary outcomes compared to control groups, including knowledge of testing locations, self-reported HIV testing, motivation to receive testing, and repeat testing.22,23,34,47
Discussion
There have been an increasing number of RCTs of HST implemented in the United States since 2010.21,36,59,64,66,69,70,76 High acceptability of HST and its potential to improve HIV testing uptake among MSM is not surprising given the positive attributes associated with the test (e.g. availability at pharmacies, oral fluid collection and rapid provision of results). In addition, HST may have the ability to decrease the stigma and discrimination associated with HIV, both of which are established barriers to HIV testing among MSM, 16 by providing a confidential and private testing environment.82,83 HST interventions also proved to be successful in increasing HIV testing among MSM in China84,85 and Australia. 86
The limitations of HST should be noted. First, a rapid self-test is unable to detect early infection due to lower sensitivity of oral fluid HST than whole blood-based test, long window period of the rapid test and poor test performance caused by lack of training or psychological factors.59,64,87,88 For example, almost 10% of participants were found to wait for less than specified amount of time before opening the test kit and interpreting the results. 59 The findings highlight the importance of provision of training in the performance of HST and technical assistance to help MSM properly conduct the test. With regard to low sensitivity and long window period, a possible solution could be the mail-in self-test. Given the limited evidence and limitations of the mail-in self-test (inability to offer quick results and unavailability at pharmacies), further research is needed to evaluate its efficacy in promoting HIV testing among MSM. Second, linkage to a confirmatory test and HIV primary care after a reactive rapid test remains a challenge due to multi-level barriers.89 –91 Epidemiological studies have demonstrated that delayed initiation of HIV treatment leads to increased incidence of AIDS or non-AIDS events, decrease in life expectancy and significant number of onward infections.92 –94 Hence, it is important for future trials to offer follow-up counseling and referral services to participants if needed. 66 Last, efficacy of HST interventions may be overestimated under experimental conditions where test kits were provided free of charge. A study conducted in urban Philadelphia found that although 90% of participants expressed willingness to use HST kits, whereas only 23% were willing to pay for it. 95 Further research regarding public funding of HST programs to maximize HST uptake among MSM is warranted. 96
At the interpersonal level, we identified two interventions trying to promote HIV testing among male couples, “2GETHER” and “We Prevent.”47,71 Couple-based interventions were designed to promote knowledge of HIV risk in couples, peer norms about prevention in relationships and sexual health communication, which were all facilitators of uptake of HIV prevention services.97,98 CHTC also facilitates the disclosure of HIV status among couples, based on which they could make sexual risk reduction plan, which is especially important for serodiscordant couples. Secondary analyses of “2GETHER” intervention further revealed the increased motivation to test for HIV with one’s partner for MSM with high internalized stigma. 48 However, given the low coverage of CHTC and multi-level barriers to the implementation but high willingness to use this service among MSM,22,99,100,101 there remains a need for more research on the development, implementation and promotion of male couple-based interventions.
Another type of interpersonal-level interventions was based on peer mentoring. The strengths of peer-mentored or peer-led interventions lie in efficient peer-based chain recruitment, high acceptance and engagement due to demographic similarity among peers, and provision of peer support.21,36,41,60 Peer-based intervention would be more useful when they are applied to minority groups, for example, Black and Latino MSM.35,60,75,80 These groups, who are disproportionately affected by HIV, lack trust in healthcare providers/system and do not have information on access to HIV prevention services.80,102,103 For example, fears related to immigration enforcement was reported to be one of the greatest barriers to HIV testing among Latino MSM. 80 Peer-based interventions bridge these gaps by providing support and creating an opportunity for minority groups to receive culturally congruent information on HIV from credible sources.35,60,75,80 Of note, for peer-led interventions, researchers should take caution with selection of peer leaders. Individuals who are both helpful and trusted within their social networks are necessary for the successful implementation of interventions. 80 It is also critical to deliver training programs to peer leaders to ensure that they could deliver high-quality interventions.
We observed one peer-based intervention, “The Passport to Wellness,” that made an effort to improve social determinants of health among Black MSM by using incentives and peer support. 75 This intervention is worth noting because it addressed negative social determinants of health including poverty, access to healthy food, stigma and discrimination, all of which were thought to be the root cause of health and barriers to seeking HIV prevention services.104,105 There remains a need for more research to integrate and address social determinants of health into HIV prevention and testing programs.
At the structural level, the only intervention implemented in recent years was the STD PS program in Washington State which ensured HIV testing for MSM with an STD and their partners. We observed a pronounced increase in HIV testing among MSM who received the diagnosis of STD from healthcare providers that were not specializing in HIV or STD care. 39 This finding highlights the great potential of the healthcare system, especially non-specialty providers, in promoting HIV testing and the importance of collaboration across health departments. However, the generalizability of a similar program in other states are uncertain given the disparity in public health infrastructure across the United States. 39
We found an increasing number of interventions incorporating personalized elements in recent years.38,41,43,44,53,54,65,72 –75 Three novel interventions seeking to connect participants with the most appropriate HIV testing approach were identified.22,38,53 Compared to common interventions to promote community- or facility-based testing, these interventions not only addressed institutional barriers to HIV testing (e.g. healthcare providers’ stigmatizing behaviors toward patients) by filtering testing sites based on participants’ past experiences and expectations, they also took into account local testing resources (e.g. geographic coverage of testing sites).22,38,53,106 However, it is important to note that the development of tailored intervention remains challenging. For instance, in the “All About Me” study, development of an algorithm to match individuals to an optimal testing method involved the identification of barriers to testing and consideration of institutional conditions. 22 Formative studies to fully understand participants’ needs and exploration of local HIV testing resources are warranted for the successful implementation of personalized interventions.
With the increasing use of the Internet and mobile technology by MSM to find HIV-related information, connect to the gay communities and seek sexual partners,107 –109 technology has become an effective tool for researchers to conduct HIV prevention interventions among MSM. The technology-delivered interventions are no doubt time-saving and convenient and thereby are cost-effective. With online recruitment, researchers could reach MSM who may be hard to reach through traditional outreach in a cost-efficient means.42,110 Flexibility in delivery enables this type of intervention to hold more promise in promoting HIV testing in the context of COVID-19 where reduction of interpersonal contact is required. Nascent technologies (e.g. virtual reality, crowdsourcing and chatbot) were reported to be used in HIV prevention in recent years.111 –115 More studies to determine their effect on MSM are required since the application of technology to HIV interventions is still at its infancy.
We identified three limitations associated with the technology-delivered interventions. First, given the ethnic/racial disparities in the use of technology for health-related purposes, Black and Latino MSM may be less likely to participate in online HIV prevention interventions and use Internet for HIV information.116 –119 The second is the moderate level of engagement probably due to the lack of direct contact with research team. 46 For example, a mobile app-based study found that almost 20% of participants never downloaded/opened the app. 23 Potential strategies to improve participants’ engagement may include adoption of existing popular platforms, incorporation of individualized and interactive activities, and reminders sent from research team via text message or email. Last, development of the website or app remains a barrier. Commonly reported issues included insufficient guidance, technical problems (e.g. app crashing or slow responsiveness) and problems with user control and freedom.23,46,56,63 When pilot testing the Status Update Project mobile app, some participants appreciated its simplicity and reminders while others thought that it was too simple and repetitive. 23 Formative studies and pilot tests are required to learn participants’ preference and test the usability of the online interventions.
There are several common limitations to current HIV testing interventions regardless of their intervention modalities. First, there might be a mismatch between the complexity of HIV information content and participants’ health literacy. For example, participants with high health literacy thought that the health information was “simplistic” and they “did not fully get the opportunity to learn anything new.”47,63 Possible solution could be the development of intervention content tailored to participants’ educational level and health literacy. Second, we observed diminished effect of the intervention across study periods.21 –23 Attention should be paid to participants who did not have established HIV testing patterns before joining the study, given the evidence that these people were less likely to follow the intervention. 23 Furthermore, incorporation of personalized elements and booster sessions might be effective in extending the effect of intervention.21,64 Third, some people did not return or follow-up for test results35,36 while knowledge of HIV status is the first step in the initiation of treatment for HIV. Reminder to follow-up on and provision of testing results via text message, email or mobile app could be useful in promoting knowledge and acceptance of HIV status among MSM. Last, condomless sex may be concomitant with increased HIV testing due to mutual knowledge of HIV-negative serostatus among couples.20,59 Therefore, integration of sexual health education into interventions for HIV testing are necessary to reinforce the importance of sexual health while promoting HIV testing among MSM.
Compared to previous reviews of HIV testing interventions among MSM,27 –29 our study extends the literature by aggregating up-to-date intervention strategies (e.g. gamification, personalization and couple-based intervention), comprehensively evaluating existing interventions in terms of acceptability, feasibility, efficacy and cost-effectiveness, and summarizing gaps/limitations in those interventions. Some limitations are also worth noting. First, the search terms used in this systematic review may not be comprehensive and therefore we were unable to include all relevant studies. Second, in addition to poor or fair methodological quality, some studies reported small sample size and short follow-up period, which might lead to low statistical power.23,36,38,41,75,80 High-quality RCTs with a large sample size and a long follow-up period are warranted to replicate their results. Finally, most studies evaluated the efficacy of the interventions by measuring self-reported binary HIV testing, which was prone to recall bias and social desirability bias.20,21,24 –26,34,35,38,39,42 –44,49 –51,54,57,61,67,68,73 –75,78 –81 Objective measures of HIV testing behavior are further required. In addition, future studies should take into account more aspects of HIV testing such as knowledge, attitudes, barriers and repeat HIV testing when evaluating their interventions.
Conclusion
MSM continue to be disproportionately affected by HIV in the United States. Low uptake of HIV testing in general, and of repeat testing among MSM is concerning. Not testing and infrequently testing may exasperate negative health outcomes, late initiation of HIV treatment, further engagement in condomless sex, and potential onward transmission of HIV. Development of interventions to improve MSM’s HIV testing rates and frequency has proliferated in recent years. Most common interventions were those focused on HST, interpersonal level, personalized, and technology delivered. These interventions hold promise in expanding the coverage of HIV testing among MSM in the United States given their acceptability, feasibility and efficacy. Researchers are presented with opportunities to overcome the limitations we identified in this review and provide more evidence to demonstrate the effect of interventions to improve HIV testing uptake and frequency among MSM in the United States.
Supplemental Material
sj-doc-1-smo-10.1177_20503121221107126 – Supplemental material for Evidence and implication of interventions across various socioecological levels to address HIV testing uptake among men who have sex with men in the United States: A systematic review
Supplemental material, sj-doc-1-smo-10.1177_20503121221107126 for Evidence and implication of interventions across various socioecological levels to address HIV testing uptake among men who have sex with men in the United States: A systematic review by Ying Wang, Jason Mitchell and Yu Liu in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all the participants in the primary studies and the teams who conducted the studies.
Author contributions
Y.L. designed the research study. Y.W. led the systematic review and drafted the first version of this manuscript. Y.W. and Y.L. conducted title and abstract screening. Y.W. conducted full-text review and extracted data which were cross-checked by Y.L. J.M. reviewed and revised the manuscript. All authors critically interpreted the results and revised the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because the present paper was a systematic review of published literatures and did not involve human subject research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study because the present paper was a systematic review of published literatures and did not involve human subject research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.