
Abstract
Objectives:
This article aims to elucidate the relationship between antiretroviral (ARV) medication changes and all-cause mortality using a total of 368 patients recruited from the United States (78%), United Kingdom (11%), and Canada (11%).
Methods:
Data sources included demographic characteristics, ARV treatment history and modifications, and clinical biomarker data from the completed OPTions In Management with Antiretrovirals clinical trial. Descriptive analysis and graphical trajectory representation of ARV drug modifications and biomarker changes were undertaken. Three hypotheses aimed at assessing the impact of ARV modification parameters on clinical outcomes were tested. Kaplan-Meier survival techniques as well as Cox proportional hazard regression models were employed.
Results:
Results from the analyses suggest that (1) switching therapy strategy from an intensified ARV regimen to a less intense one or vice versa, (2) having a moderate number (up to 2) of ARV drug changes per 6 months, and (3) changes based on clinical/HIV-related reasons or nonclinical reasons compared to ARV drug regimen changes due to clinical non-HIV reasons improved survival.
Conclusion:
Modifications in the ARV regimens of HIV-infected patients with multidrug resistance are associated with improved survival.
Introduction
Highly active antiretroviral therapy (currently known as combination antiretroviral therapy) has decreased the incidence of AIDS-defining illness and burden of disease in HIV-infected patients. 1 -5 However, multidrug-resistant (MDR) HIV as well as narrowed retreatment options continue to undermine successful clinical management and remain an ongoing public health concern, especially in resource-limited settings. 6 -11 The OPTions In Management with Antiretrovirals (OPTIMA) trial, at the time it was conducted, was the largest study of treatment strategies for patients with advanced-stage AIDS and failing therapy due to MDR HIV infection having few treatment options. 8 Using a 2 × 2 factorial design, OPTIMA evaluated the effect of standard-antiretroviral therapy (standard-ART; ≤4 ARV drugs) versus intensive ART (mega-ART; ≥5 ARV drugs) 12 -14 as well as the impact of a 12-week antiretroviral drug-free period (ARDFP) versus No ARDFP, 15,16 on the onset of a new or recurrent AIDS event or death from any cause. 7
Despite unsurprisingly high overall mortality of 47%, OPTIMA did not show any statistically significant differences between treatment strategies. In the retreatment options of standard-ART versus mega-ART, 67 (34%) of 192 patients and 61 (35%) of 176 patients died, respectively (P = .96). Between immediate retreatment compared to a brief ARV interruption before retreatment, 62 (35%) of 175 patients and 61 (37%) of 164 patients died, respectively (P = .72). 7,17
What Do We Already Know about This Topic?
Optimal management of multidrug-resistant HIV for patients with advanced-stage AIDS is challenging and uncertain.
How Does Your Research Contribute to the Field?
Progression of disease in this population is associated both with failure to change treatment regimens and with having to change regimens more than once or twice.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Empiric changes in ARV regimens should be avoided whenever possible but particularly in the setting of sequential treatment failure where limited treatment options are available.
In this article, we present the results of a secondary analysis of the trial data to determine whether changes in patterns of ARV treatment were associated with differential survival within the OPTIMA study. We assessed ARV medication change patterns across patients and examined their relationship with a patient’s risk of experiencing major adverse clinical outcomes. Three ARV medication modification parameters were analyzed: (1) changes in ARV strategy, (2) rate per 6 months of ARV drug changes, and (3) reasons for ARV drug changes.
Methods
The trinational OPTIMA trial was designed as a 2 × 2 factorial comparison of standard-ART with mega-ART and a 12-week ARDFP versus No ARDFP (Clinicaltrials.gov NCT00050089). A total of 339 patients were randomized to the 2 × 2 factorial design and 29 UK participants were randomized, as allowed per study protocol, to the “UK pilot,” where participants could choose 1 of the 2 randomizations (mega-ART versus standard-ART or ARDFP versus No ARDFP) and would then be randomized to the other factorial arm. In total, the trial randomized 368 participants from the United States Department of Veterans Affairs(n = 288), the United Kingdom (n = 39), and Canada (n = 41) who were followed for a median of 4 years. Details of the study design and results are provided elsewhere. 2,8
Research Ethics and Patient Consent
The protocol was approved by independent Research Ethics Boards at each site. The trial was performed in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki. All volunteers signed written informed consent before any trial related procedure (see Appendix A for participating sites).
Antiretroviral Accounting
Antiretroviral drug modification patterns were described using the following conventions: Each active ARV drug within a combination drug was independently counted in the sum of ARV drugs. For example, Combivir, a combination of lamivudine (3TC) and zidovudine (ZDV), counted as 2 ARV drugs. At a daily dosage below 400 mg, ritonavir (RTV) counted as a booster protease inhibitor and not as a separate ARV drug. Changes from 3TC to emtricitabine were counted for purposes of defining a switch since the difference in dosing frequency could affect adherence.
Antiretroviral Therapy Strategy Switches
During follow-up, participants were considered compliant to their randomly assigned ARV therapy strategy if their total time off the assigned strategy (standard-ART or mega-ART) did not exceed 30 days. 4,17 Compliance with treatment strategy was not affected by changes in ARV regimens used as long as the number of drugs in the regimen conformed to the assigned strategy. We defined compliance percentage to assigned ARV therapy strategy of each patient as

Actual time on assigned strategy was defined as the time a participant took the strategy-assigned ARV drugs irrespective of the ARV drug combination. Expected time on assigned strategy was defined as the duration of follow-up for each patient after ART was initiated minus the time the patient was not taking any ARV drugs due to clinical reasons. Participants with 100% compliance were classified in the “nonswitching strategy group,” while participants with compliance less than 100% were classified in “switched ARV strategy group.”
Rate of ARV Drug Changes
Antiretroviral drug changes were defined as changes in unique ARV medications used in a regimen, whether alone or co-formulated in combination with other ARV. Changes from brand name to generic drugs or between drugs otherwise judged to be biologically equivalent, that is, a change from 3TC to emtricitabine, were not counted in this analysis. The rate per 6 months of ARV drug changes was determined as the number of changes over the follow-up period for each patient divided by the total number of months of follow-up times 6 months. Rates were then categorized into 4 change levels: none, >0 to 1, >1 to 2, and more than 2.
Reasons for ARV Drug Changes
The primary reason for ARV drug change each time a patient started, stopped/interrupted, and changed dosage of a drug was recorded. The 9 reasons for ARV drug changes were categorized into 3 groups: clinical/not HIV-related (adverse events; adverse event grade 1 or 2; intercurrent illness), clinical/HIV-related (high viral load; low CD4
count; progression to HIV disease), and nonclinical (other physician/patient decision; patient unable to adhere [not because of an adverse event]; voluntary patient decision). Patients were classified into 1 of these 3 groups based on their most frequent type of reason.
Analysis
Characterization of the analysis data set includes a summary of the baseline characteristics for each subgroup of participants classified according to ARV strategy switch, ARV drug change, and reason for ARV drug change, respectively. Data from 9 participants who had neither baseline ARV drug regimen nor follow-up ARV modification information were excluded from the analysis, since their ARV drug change pattern could not be defined.
Survival rates were estimated by Kaplan-Meier and differences in survival rates were tested by the log-rank statistic. Univariate and multivariate survival analyses were also conducted using the Cox regression model for ARV strategy switch, ARV drug change, and reason for ARV drug change subgroups. Univariate analyses evaluated each of the 3 subgroups separately. The univariate analysis of reasons for drug change excluded 57 participants because they did not have a drug change and hence no reason for a drug change. Multivariate analyses jointly analyzed the 3 subgroups in 2 ways: unadjusted and adjusted for important baseline covariates: age, ethnicity, country, assigned treatment strategy, HIV drug history, baseline CD4 count, and baseline log viral load value. The unadjusted multivariate analysis excluded the 57 participants who had no drug change and adjusted multivariate analysis excluded an additional 29 participants because randomization to ARDFP or No ARDFP treatment strategy was not done in the United Kingdom, that is, no baseline value for assigned treatment strategy. The proportional hazards assumption was examined for all fitted models via Schoenfeld residuals plots and their correlation coefficients with time. P values were corrected for multiple comparisons using the Bonferroni method.
Results
Demographic and baseline characteristics of the OPTIMA cohort have already been reported. 8 During a median follow-up of 4 years, 359 (98%) of the 368 patients randomized in OPTIMA had information about ARV drug usage. Tables 1 to 3 present characteristics of participants classified according to ARV strategy switch, ARV drug change, and reason for ARV drug change, respectively.
Baseline Characteristics by the ARV Strategy Switch.

Abbreviations: ARV, antiretroviral; SD, standard deviation.
Baseline Characteristics by the Number of ARV Drug Changes.

Abbreviations: ARV, antiretroviral; SD, standard deviation.
a Data are not available.
Baseline Characteristics by the Reason for ARV Drug Changes.
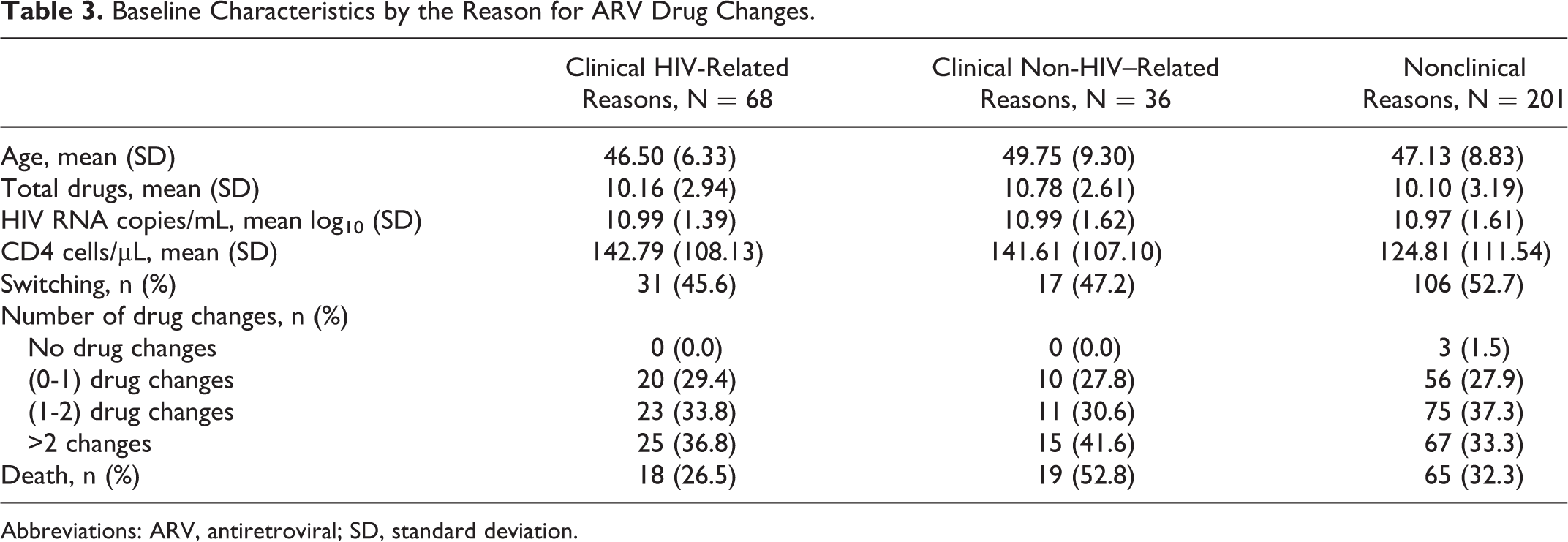
Abbreviations: ARV, antiretroviral; SD, standard deviation.
Antiretroviral Strategy Switch
Among the 359 analyzable patients, 204 (57%) were compliant with their assigned strategy throughout the follow-up period, while 155 (43%) had switched ARV strategy. Overall, participants who switched ARV drug strategy had significantly better survival compared to those who did not switch, although the curves converge after 2000 days (approximately 5.5 years; Figure 5A, P = .036).
Survival Association with ARV Drug Change
A total of 57 participants had no ARV drug changes during follow-up and 86 patients had up to 1 drug change per 6 months. Similar numbers of patients had more than 1 to 2 drug changes per 6 months (n = 109) or more than 2 drug changes per 6 months (n = 107).
Survival curves are shown in Figure 1B for all 4 groups of ARV drug changes. Overall, there was a significant difference in survival (P < .0001) among the 4 groups. Survival was significantly worse (P < .001) for those with more than 2 changes compared to the groups with 1 and 2 changes. It was also significantly worse for those with no changes compared to the latter 2 groups (P < .001 and P = .03, respectively). The survival differences between the groups with no changes and more than 2 changes were not significantly different (P = .86) as was the difference between the groups with 1 and 2 changes (P = .15).
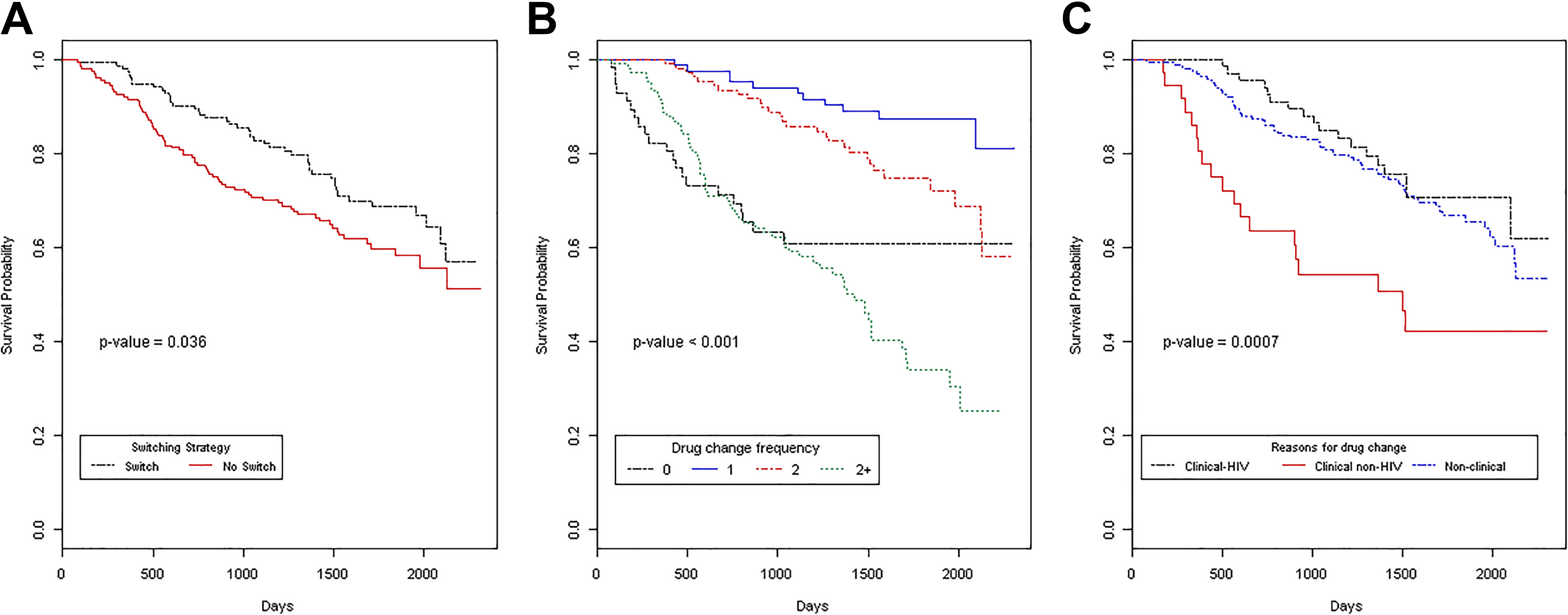
(A) Kaplan-Meier cumulative survival probabilities stratified by switching strategy status (time in days); (B) Kaplan-Meier cumulative survival probabilities stratified by rate of drug change per 6 months (time in days); (C) Kaplan-Meier cumulative survival probabilities stratified by reasons for drug change (time in days). P values are the results of the log-rank test.
Survival Association with Reason for ARV Drug Change
For patients who had at least 1 ARV drug change (n = 305), the most frequent reasons for ARV drug changes were grouped into 3 categories: (1) clinical/not-HIV–related reasons (grades 1/2 adverse events; intercurrent illness; n = 36; 12%); (2) clinical/HIV-related reasons (high viral load, low CD4 count, disease progression; n = 68; 22%); and (3) nonclinical (other physician/patient decision, patient unable to adhere [no adverse events], voluntary patient decision; n = 198; 66%).
Figure 1C displays the survival curves by reason for drug change group. Overall, the survival curves were significantly different (P value = .0007). Survival for the group with clinical non-HIV reasons was significantly worse (P < .001) than the groups with clinical HIV-related reasons and nonclinical reasons, respectively. Survival was not statistically different between the latter 2 groups (P = 1.0).
Cox Regression Analysis
Table 4 gives the results of univariate and multivariate Cox regression analyses of the ARV strategy switch, ARV drug change, and reason for ARV drug change subgroups. As expected, the univariate analyses are consistent with those of the log-rank statistic presented earlier because the model is the same. The independent effects of switching ARV drug strategy, rate of ARV drug changes, and reasons for ARV drug changes were consistent with the univariate findings, even after adjustment for important baseline covariates. However, the effect of switching strategy appears to have bigger impact on survival in the multivariate analyses (hazard ratios = 0.36 unadjusted and 0.32 adjusted) compared to the univariate analysis (hazard ratio = 0.68), but these results must interpreted cautiously because they are conditional on having at least 1 drug change.
Unadjusted and Adjusted Cox Analysis of Switching, Rate of Drug Changes and Reasons for Drug Changes.
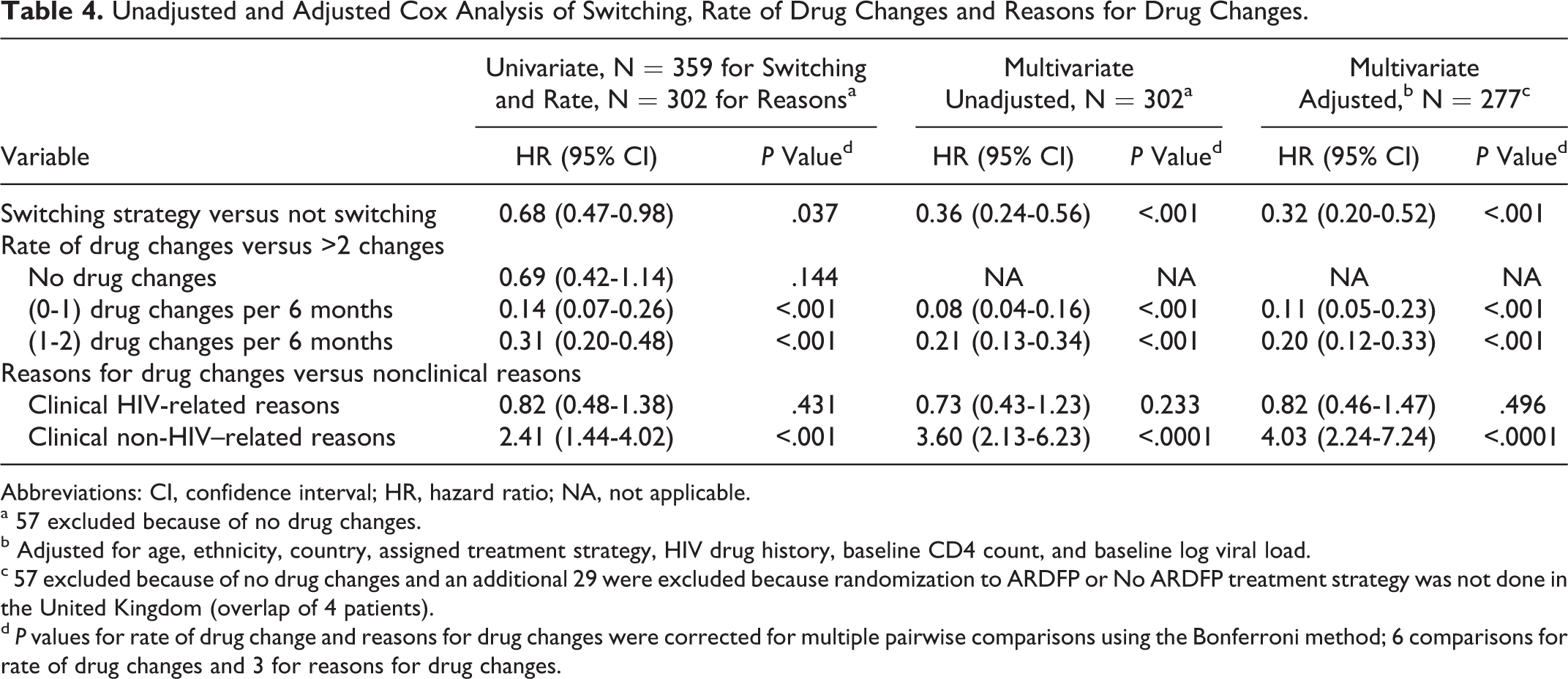
Abbreviations: CI, confidence interval; HR, hazard ratio; NA, not applicable.
a 57 excluded because of no drug changes.
b Adjusted for age, ethnicity, country, assigned treatment strategy, HIV drug history, baseline CD4 count, and baseline log viral load.
c 57 excluded because of no drug changes and an additional 29 were excluded because randomization to ARDFP or No ARDFP treatment strategy was not done in the United Kingdom (overlap of 4 patients).
d P values for rate of drug change and reasons for drug changes were corrected for multiple pairwise comparisons using the Bonferroni method; 6 comparisons for rate of drug changes and 3 for reasons for drug changes.
Discussion
HIV MDR creates challenges for the management of ARV therapy in patients with advanced-stage HIV/AIDS; modification of ARV drug regimen could potentially help address this challenge. Although the primary results of the OPTIMA study did not show any statistically significant differences between standard-ART and mega-ART strategies or between the ARDFP group and No ARDFP group, differences in patterns of ARV treatment during follow-up were associated with survival outcomes.
Switching ARV therapy strategy (mega-ART to standard-ART or vice versa), having a moderate number (up to 2) ARV drug changes per 6 months, and changing the ARV drug regimen based on clinical/HIV-related reasons or nonclinical reasons are treatment strategies in this complex clinical setting that may improve survival. In multivariate analysis, these strategies were independently predictive of survival conditional on having at least 1 drug change.
There was a 33% overall mortality rate in OPTIMA, 68% of which occurred in those with either no or greater than 2 drug changes. The most likely reason for the improved survival seen in patients having 1 to 2 changes in ARV regimens is that regimens arrived at were reasonably successful in achieving more sustained suppression of HIV progression whether the change resulted from HIV progression, other non-HIV–related adverse events, or another patient or provider decision. Failure associated with frequent changes is likely to reflect sequentially futile efforts to establish effective treatment. Poorer outcomes in those with no drug change may reflect death or illness as a competing factor or recognition of clinical futility for further treatment change.
Populations with advanced-stage AIDS having MDR virus for which no fully effective treatment options are available, the principle eligibility criteria for entry into OPTIMA, remain a significant clinical challenge globally. It has been difficult to replicate the success of antiviral therapy achieved by developed countries in low-middle-income countries. 18 Delays in diagnosis, inadequate health-care infrastructure, limited ARV treatment options, and economic and social barriers to adherence contribute to suboptimal treatment, which results in significant rates of ARV resistance, progression of disease, and mortality. 19,20 Insights from this analysis have implications for clinical decisions in analogous populations. They reinforce the importance of strategies to preserve treatment options until effective regimens are available. 21 Empiric changes in ARV regimens should be avoided whenever possible but particularly in the setting of sequential treatment failure where limited treatment options are available.
There are several limitations in this analytical project: (1) The study cohort included a very small number of women and thus the impact of gender could not be adequately assessed; (2) time-varying effects of the possible ARV modification patterns (switching ARV strategy, frequency of ARV drug changes, and reasons for ARV drug change) were not applied in the survival analysis methods; and (3) reasons for ARV drug changes were not always known and thus, the comparison of survival experience among different reason groups might not be reflective of the true clinical presentation.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Cooperative Studies Program of the Department of Veterans Affairs Office of Research and Development.