
Abstract
Objective
To compare the all-cause mortality of aged and younger patients undergoing maintenance hemodialysis (MHD) over the long or short term, and to identify independent risk factors.
Methods
We performed a retrospective cohort study using the medical records of 181 patients undergoing MHD. We compared the clinical characteristics and laboratory data of survivors and participants who died, according to their age and the duration of MHD. Binary stepwise logistic regression was used to identify independent risk factors for all-cause mortality.
Results
Cardiovascular and cerebrovascular diseases were the principal causes of mortality. The number of aged participants with hypertensive nephropathy as their primary kidney disease was significantly higher than the number of younger participants. The proportion with chronic glomerulonephritis was significantly higher for participants undergoing long-term MHD. Logistic regression analysis revealed that low body mass index, single-pool Kt/V, serum albumin, platelet count, and total iron-binding capacity; and high intact parathyroid hormone and N terminal pro B type natriuretic peptide were independent risk factors for all-cause mortality.
Conclusions
Aged patients are more susceptible to hypertensive nephropathy than younger patients. In addition, the survival of patients with chronic glomerulonephritis undergoing MHD is superior to that of those with hypertensive or diabetic nephropathy.
Keywords
Introduction
Chronic kidney disease (CKD) is a major public health problem worldwide, and is responsible for hospitalization, morbidity, and mortality when it progresses to end-stage renal disease (ESRD), as well as a huge economic burden.1,2 Cardiovascular disease (CVD) and infections are the major causes of mortality in patients with CKD, together accounting for up to 70% of all deaths.3,4 Specifically, cerebrovascular accidents (CVAs) are associated with a poorer prognosis in patients with CKD. An annual report by the United States Renal Data System (USRDS) showed that the overall prevalence of CVA in patients with CKD was 16.1% and the 2-year survival rate of patients with ESRD and CVA was just 64.1%. 5
Maintenance hemodialysis (MHD) is a form of renal replacement therapy that improves the prognosis and prolongs the survival of patients with ESRD. However, previous studies have shown a close association between long-term dialysis and mortality in patients undergoing MHD.6,7 Furthermore, a large-scale cohort study conducted in Japan showed that the duration of dialysis has differing associations with specific causes of mortality: MHD is associated with a higher risk of infection-related mortality than CVD-related mortality, especially in patients undergoing long-term MHD. 8 In addition, advanced age is associated with shorter survival in patients undergoing MHD. 9 Older patients are more likely to die of their primary disease when initiating dialysis and they are also more likely to experience various complications of dialysis. 10 Previous studies have also shown that advanced age and long-term dialysis are associated with the progression of MHD in patients.8–10 However, it has not been determined whether there is a difference in the all-cause mortality of aged and younger patients undergoing MHD or among patients who undergo dialysis for differing durations.
We aimed to perform a retrospective cohort study to identify the causes of death and the primary diseases of patients of various ages and durations of dialysis who are undergoing MHD, and to identify independent risk factors for all-cause mortality, with the aim of improving survival and improving the efficacy of hemodialysis.
Methods
Study design and participants
We conducted a retrospective cohort study of patients undergoing MHD three times weekly at the Blood Purification Center of Huashan Hospital, affiliated with Fudan University, between 1 January 2014 and 31 December 2018. The exclusion criteria were: age <18 years, renal transplantation, previous peritoneal dialysis, and previous severe surgical trauma or mental illness. We allocated the eligible participants to two groups: a survival group, comprising patients who were still alive on 31 December 2018, and a mortality group, comprising those who had died for any reason during the study period (Figure 1). All the participants gave their written informed consent, the study was performed according to the principles of the Declaration of Helsinki, and it was approved by the Ethics Committee for Human Research of Huashan Hospital (No.KY2018-368).

Flowchart of study enrollment.
Data collection
The clinical characteristics of the patients, including their age, sex, duration of dialysis, primary kidney disease, pre-dialysis blood pressure, dry body mass, and cause of death, were obtained from the database of the dialysis center. The primary kidney disease was categorized as hypertensive nephropathy (HTN), diabetic nephropathy (DN), chronic glomerulonephritis (CGN), polycystic kidney disease (PKD), or other (such as gout, pyelonephritis, and systemic lupus erythematosus). The duration of dialysis was defined as the period between the year of initiation of dialysis and the year of the last follow-up examination. Long-term dialysis was defined as a duration of ≥10 years. Blood pressure was measured three times, before each hemodialysis session, during the week preceding the end of follow-up. The causes of death were defined as cardiovascular disease (myocardial infarction, aortic dissection, or heart failure), cerebrovascular accident (cerebral hemorrhage or cerebral infarction), severe infection (severe pneumonia, severe acute pancreatitis or septic shock), malignancy, sudden death for unknown reasons, and other diseases.
The following laboratory data were collected: serum creatinine, blood urea nitrogen (BUN), serum albumin, alkaline phosphatase (ALP), intact parathyroid hormone (iPTH), calcium, phosphorus, potassium, C-reactive protein (CRP), carbon dioxide combining power (CO2-CP), N terminal pro B type natriuretic peptide (NT-proBNP), platelet count, iron, unsaturated transferrin, total iron-binding capacity (TIBC), ferritin, and β2-microglobulin (β2-MG), and the hematocrit (HTC). These data were obtained from the hemodialysis records immediately prior to the primary study endpoint of death or the end of the study.
Statistical analysis
Continuous data are summarized using mean ± SD or median (interquartile range, IQR), and categorical data are expressed as frequency and percentage. Comparisons between continuous datasets were performed using unpaired Student’s t-test for parametric data or the Mann–Whitney Rank Sum test for non-parametric data. The chi-square test was used to compare categorical datasets. P < 0.05 was considered to represent statistical significance. Binary stepwise logistic regression was used to identify independent risk factors for all-cause mortality. Analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA) or GraphPad Prism software version 8.0 (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Comparison of the mortality associated with cardiovascular and cerebrovascular events during each year
During the years 2014 to 2018, the annual mortality rates for the participants were 7.9%, 6.4%, 7.3%, 8.7%, and 6.6%, respectively, with a mean annual mortality rate of 7.4%. Seventy-six participants died during the study, of whom 39.5% were women. Regarding the causes of mortality, 21.1% deaths were caused by cardiovascular disease, 25.0% by cerebrovascular disease, 29.0% by severe infection, and 7.9% by malignancy; 5.3% of the deaths were sudden, with no cause identified; and 11.8% of deaths were caused by other diseases. The proportions of the annual total mortality accounted for by cardiovascular events were 23.5%, 42.9%, 20.0%, 17.7%, and 0, respectively; and those accounted for by cerebrovascular events were 29.4%, 21.4%, 13.3%, 29.4%, and 30.8%, respectively (Figure 2).

Trends in the prevalences of death secondary to cardiovascular and cerebrovascular events during the years of the study.
Comparison of the causes of death in and the primary kidney diseases of aged and younger participants
Fifty-nine of the participants were ≥65 years old, and they accounted for 77.6% of the total number of deaths. The mean ages of the aged and younger participants were 77 ± 7 years and 56 ± 8 years, respectively. Cardiovascular or cerebrovascular diseases were the cause of death in 47.5% and 41.2% of the aged and younger participants, respectively. The number of patients with HTN as the primary kidney disease in the aged group was significantly higher than that in the younger group (37.3% vs. 11.8%, respectively, P = 0.046), whereas the prevalences of DN (29.4% vs. 23.7%, respectively) and CGN (47.1% vs. 23.7%, respectively) tended to be higher in the younger group, although these differences did not achieve statistical significance (Table 1).
Comparison of the causes of death and the primary kidney disease in participants who were aged or younger.

Values are expressed as mean ± SD, or number (percentage), as appropriate. Data were analyzed using the unpaired Student’s t-test, the Mann–Whitney Rank Sum test, or the chi-square test, as appropriate. Aged group: ≥65 years of age; Younger group: <65 years of age.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; spKt/V, single-pool Kt/V; nPCR, normalized protein catabolic rate; CVD, cardiovascular disease; HTN, hypertensive nephropathy; DN, diabetic nephropathy; CGN, chronic glomerulonephritis; PKD, polycystic kidney disease.
Comparison of the causes of death in and the primary kidney disease of participants who had undergone dialysis over the long or short term
Twenty-nine participants had undergone long-term MHD (≥10 years), and this group accounted for 38.2% of the total number of deaths. In comparison, 47 had undergone short-term dialysis (<10 years), and this group accounted for 61.8% of the total number of deaths. The mean durations of dialysis were 15.9 ± 3.2 years and 5.4 ± 2.8 years in the long- and short-term groups, respectively. The proportions of deaths caused by cardiovascular or cerebrovascular events were 44.8% and 46.8% in the long- and short-term groups, respectively. The proportions of deaths caused by other diseases were 24.1% and 4.3% in the long- and short-term groups, respectively (P = 0.025) (Table 2). The proportion of the participants with DN as their primary kidney disease was significantly higher in the short-term dialysis group than in the long-term dialysis group (36.2% vs. 6.9%, respectively; P = 0.04), whereas the proportion of the participants who had CGN was significantly higher in the long-term dialysis group (48.3% vs. 17.0%, respectively; P = 0.04) (Table 2).
Comparison of the cause of death and primary kidney disease in participants who had undergone long- or short-term dialysis.

Values are expressed as mean ± SD, or number (percentage), as appropriate. Data were analyzed using the unpaired Student’s t-test, the Mann–Whitney Rank Sum test, or the chi-square test, as appropriate.
SBP, systolic blood pressure; DBP, diastolic blood pressure; spKt/V, single-pool Kt/V; nPCR, normalized protein catabolic rate; CVD, cardiovascular disease; HTN, hypertensive nephropathy; DN, diabetic nephropathy; CGN, chronic glomerulonephritis; PKD, polycystic kidney disease.
Comparison and binary stepwise logistic regression analysis of the clinical characteristics of participants who survived or died
Of the 181 participants, 105 survived and 76 died during the study period. At baseline, the mean ages of the two groups were 63 ± 12 and 72 ± 11 years, and their mean durations of MHD were 8.9 ± 6.7 and 9.4 ± 5.9 years, respectively. There were significant differences in the following parameters between the groups: age; proportion who were ≥65 years old; body mass index (BMI); pre-dialysis systolic blood pressure; pre-dialysis diastolic blood pressure; single-pool (sp)Kt/V; normalized protein catabolic rate (nPCR); the proportion with diabetes; and pre-dialysis blood creatinine, urea nitrogen, albumin, ALP, iPTH, serum potassium, CRP, NT-proBNP, platelet count, hemoglobin, serum iron, HCT, TIBC, and β2-MG (all P < 0.05) (Table 3). Binary stepwise logistic regression analysis showed that low BMI (odds ratio [OR] 5.878, P = 0.015), spKt/V (OR 7.224, P = 0.007), albumin (OR 9.741, P = 0.002), platelet count (OR 7.630, P = 0.006), and TIBC (OR 6.080, P = 0.014); and high iPTH (OR 4.355, P = 0.037) and NT-proBNP (OR 6.499, P = 0.011) were independent risk factors for all-cause mortality (Table 4).
Comparison of the clinical characteristics of participants who survived or died during the study period.

Values are expressed as mean ± SD, median (IQR), or number (percentage), as appropriate. Data were analyzed using the unpaired Student’s t-test, the Mann–Whitney Rank Sum test, or the chi-square test, as appropriate.
BMI, body mass index; spKt/V, single-pool Kt/V; nPCR, normalized protein catabolic rate; CVD, cardiovascular disease; BUN, blood urea nitrogen; ALP, alkaline phosphatase; iPTH, intact parathyroid hormone; CRP, C-reactive protein; CO2-CP, carbon dioxide combining power; NT-proBNP, N terminal pro B type natriuretic peptide; HCT, hematocrit; TIBC, total iron-binding capacity; β2-MG, β2-microglobulin.
Independent risk factors for all-cause mortality in the participants, assessed using binary stepwise logistic regression analysis.
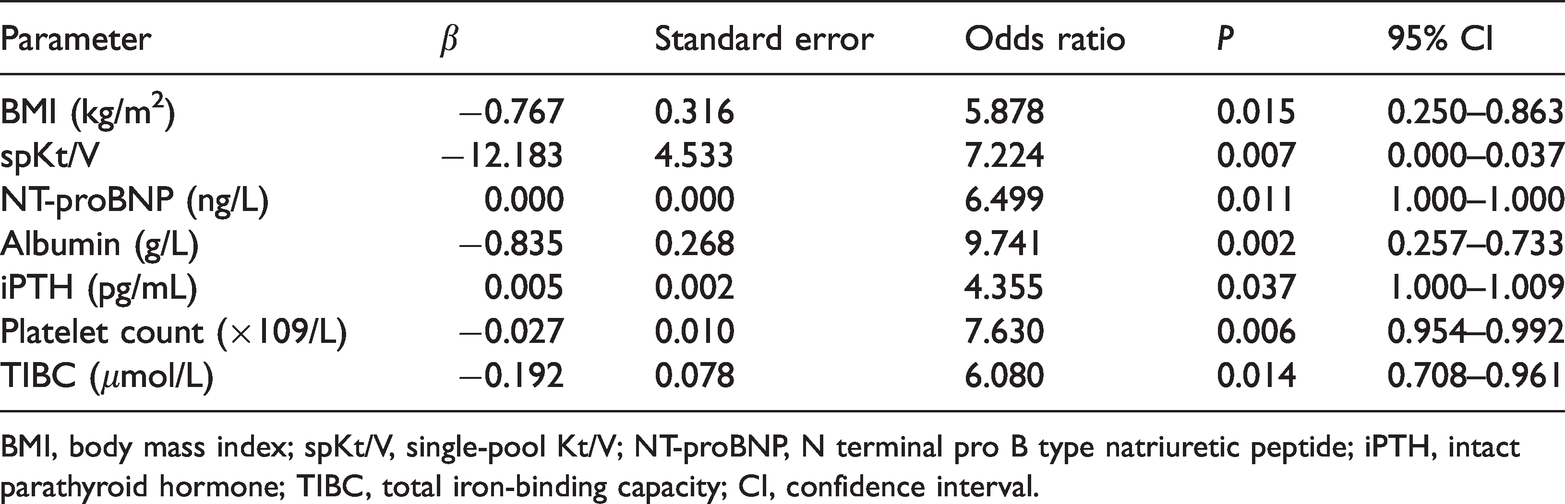
BMI, body mass index; spKt/V, single-pool Kt/V; NT-proBNP, N terminal pro B type natriuretic peptide; iPTH, intact parathyroid hormone; TIBC, total iron-binding capacity; CI, confidence interval.
Discussion
According to an annual report by the USRDS, cardiovascular events and infection are the most common causes of death among patients undergoing MHD. 11 In addition, Ali and colleagues showed that cardiovascular events, infection, and malignancy are the leading causes of the mortality in patients commencing MHD. 12 However, a recent multi-center study conducted in China showed that the most common cause of death is a cardiovascular event (37.9%), followed by a cerebrovascular event (20.3%). 13 Consistent with this, we found that cardiovascular and cerebrovascular diseases were the commonest causes of death in participants undergoing hemodialysis. A prospective cohort study comprising phases 4 and 5 of the Dialysis Outcomes and Practice Patterns Study (DOPPS) found that although cardiovascular events were common among patients undergoing hemodialysis, their incidence varied geographically. 14 During recent years, with advances in the prevention of cardiovascular events, including the regular use of echocardiography and coronary computed tomography to assess calcification, the incidence of cardiovascular events at our center has decreased substantially, whereas that of CVA has increased. A previous cohort study conducted in the UK showed that the incidence of cerebrovascular events in patients undergoing MHD was more than 10 times higher than in the general population, and the mortality rate was approximately three times higher. 15 Thus, CVA poses a significant threat to the survival of patients undergoing MHD. Given that the institution of preventive measures and timely medical interventions should reduce these risks, regular screening for cerebrovascular events and close monitoring should be instituted, especially for patients with a previous history of stroke.
It was previously shown that long-term dialysis was associated with high all-cause mortality in a large cohort of patients undergoing hemodialysis in Japan. 8 A recent cohort study also showed that physical quality of life deteriorates as the duration of dialysis increases in older patients undergoing MHD. 16 To our knowledge, few studies have investigated the relationships of the duration of dialysis and the survival or prognosis of patients with specific primary kidney diseases. Notably, we found that the duration of dialysis was associated with the identity of the primary kidney disease, and specifically that the survival and prognosis of participants with CGN were significantly better than those of participants with HTN or DN. CGN was the most common cause of glomerulosclerosis and ESRD, and involved proteinuria and hematuria, 17 CGN exists in a variety of complex pathological types, including IgA nephropathy, membranoproliferative glomerulonephritis (MPGN), focal segmental glomerulosclerosis (FSGS), and idiopathic membranous nephropathy (IMN); and therefore the therapy and prognosis of CGN varies from person to person. Furthermore, Litovkina et al. found that genes involved in the regulation of vascular homeostasis have a significant effect on the renal survival rate of patients with CGN. 18
In contrast, the USRDS showed that DN was the principal cause of ESRD, followed by HTN. 5 Furthermore, a multi-center prospective cohort study conducted in Japan showed that the all-cause mortality associated with HTN patients was as high as that for patients with DN, and that the prognosis of patients with ESRD secondary to HTN was as poor was that of patients with DN. 19 When blood pressure and blood glucose concentration were not well controlled, patients with HTN or DN showed further deterioration of renal function and the development of complications, including hyperkalemia, infection, and congestive heart failure. Similarly, a 9-year cohort study conducted in Japan showed that the presence of diabetes mellitus predisposes toward all-cause mortality in patients undergoing hemodialysis. 20 Consistent with this, reductions in systolic blood pressure and glycosylated hemoglobin A1c prolong the survival of patients with DN. 21 Thus, the management of blood pressure and blood glucose is essential for patients undergoing MHD.
BMI and serum albumin are important indicators of nutritional status, and are closely associated with malnutrition, inflammation, chronic protein-energy wasting, and even all-cause mortality.22,23 Consistent with the findings of the DOPPS, 24 we found that low baseline BMI and serum albumin concentration are independently associated with a higher risk of mortality. Moreover, because of insufficient erythropoietin or the accumulation of toxins in the circulation, patients undergoing MHD tend to develop renal anemia to varying extents, involving a lower hemoglobin concentration, a lower platelet count, and less hematopoiesis. A recent clinical study showed that low transferrin saturation and a high ferritin concentration are predictors of cerebrovascular and cardiovascular disease and mortality in patients undergoing MHD. 25 Notably, we have shown that low TIBC and platelet count are associated with a higher risk of all-cause mortality. Iron use disorders would aggravate any anemia, and thrombocytopenia would increase the risks of bleeding and infection. In addition, we have shown that high iPTH and NT-pro BNP concentrations are associated with a high mortality rate in patients undergoing MHD. As the duration of dialysis and the age of the participants increased, there was progressive deterioration of calcium and phosphorus metabolism in patients undergoing hemodialysis, but hyperphosphatemia and hypocalcemia would stimulate the secretion and release of PTH, leading to secondary hyperparathyroidism, osteoporosis, and even cardiovascular events.26,27 NT-proBNP concentration is widely used to assess cardiac function, and high concentrations are associated not only with CVD-related, but also non-CVD-related mortality. 28 Consistent with the findings of Kara et al., 29 we found that a low spKt/V is associated with a higher risk of death in patients undergoing MHD. The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) Clinical Practice Guideline for Hemodialysis has recommended a target spKt/V of 1.4 per hemodialysis session for patients being treated three times weekly, and a minimum spKt/V of 1.2. 30 Sahutoglu et al. also found that a high spKt/V (>1.4) was associated with lower 1-year mortality in a small cohort of patients undergoing MHD. 31 Further studies are required to assess the association between the effectiveness of hemodialysis and mortality.
The findings of the present study should be viewed in light of its limitations. Because it was a single-center retrospective cohort study, a number of potentially confounding factors could not be accounted for. In addition, it had a small sample size, there was a lack of information regarding other causes of death, and the effects of various dialysis modes were not investigated. Therefore, further multi-center, large-scale, prospective studies should be conducted to identify further risk factors for mortality in patients undergoing MHD.
In conclusion, the mean annual mortality rate of patients undergoing MHD at our center was 7.4%. In these patients, the prevalence of cardiovascular events as a cause of death decreased between 2015 and 2018. In contrast, death from cerebrovascular events increased in prevalence between 2016 to 2018, which implies that more attention should be paid to screening and preventative measures for cerebrovascular diseases. Long-term dialysis was closely associated with specific primary kidney diseases, and specifically the survival time and prognosis of patients with CGN were significantly better than those of patients with HTN or DN. Low BMI, spKt/V, albumin, platelet count, and TIBC; and high iPTH and NT-proBNP concentration were found to be independent risk factors for all-cause mortality in patients undergoing MHD.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded by the Natural Science Foundation of China (No. 81870501) and the Shanghai Science and Technology Commission Fund (No. 19411967800).