
Abstract
Objectives:
The fasting plasma glucose/hemoglobin A1c ratio is considered a marker associated with glucose metabolism disorders, including fasting hyperglycemia. However, it remains unclear whether this ratio can be used for the prevention of deaths in individuals with normal fasting plasma glucose levels. This study aimed to see the predictive value of the fasting plasma glucose/hemoglobin A1c ratio for all-cause mortality in a general population with normal fasting plasma glucose levels.
Methods:
The study investigated prospectively a cohort of 1087 multi-regional, community-dwelling Japanese participants (women, 69.2%) for a follow-up period of 11.3 years. We included individuals with fasting plasma glucose levels <6.11 mmol/L and excluded those meeting the diabetes criteria. All-cause mortality was the primary outcome and hazard ratios were calculated using the Cox proportional hazard model after dividing the fasting plasma glucose/hemoglobin A1c ratios into tertiles.
Results:
There were 54 deaths (25 women) during the follow-up period. The high tertile group had a significantly higher hazard ratio for all-cause mortality than the low tertile group in women (multivariate-adjusted hazard ratio = 4.45; 95% confidence interval = 1.26–15.72), but not clearly in men.
Conclusion:
The data of the population-based cohort study suggest that a high fasting plasma glucose/hemoglobin A1c ratio can predict all-cause mortality in women with normal fasting plasma glucose levels.
Keywords
Introduction
Patients with glucose metabolism disorders are at risk of all-cause mortality,1,2 and in the current clinical environment, maintaining low levels of fasting plasma glucose (FPG) is thought to be a strategy to prevent the deaths.3,4 A high-normal FPG level or impaired fasting glucose (e.g. 6.11–6.99 mmol/L by the World Health Organization criteria) can predict all-cause mortality relative to normoglycemia. 5 Further studies are required to see the impact of normal FPG levels on mortality. 6 All-cause mortality in a cohort population with normal FPG levels (i.e. <6.11 mmol/L) is of interest.
The FPG levels are typically directly proportional to the hemoglobin A1c (HbA1c) levels,7,8 while some individuals show a discrepancy between their FPG and HbA1c levels, even at the normal FPG levels.9,10 In understanding of the feature of FPG and HbA1c, the combination of FPG with HbA1c is indicated to be relevant for clinical management.9,10 The FPG/HbA1c ratio is a clinical laboratory marker reflective of the pathophysiological imbalance between FPG and HbA1c. Generally, this ratio is high in individuals with fasting hyperglycemia (predominantly associated with hepatic insulin resistance)11,12 and low in those with postprandial hyperglycemia (predominantly associated with muscle insulin resistance).12–14 Compared with FPG, thus, the measurement of the FPG/HbA1c ratio may identify individuals at risk of mortality among those with normal FPG levels. This study aimed to see whether the FPG/HbA1c ratio can predict all-cause mortality, at the normal FPG levels, in the general Japanese population.
Materials and methods
Study population
The Jichi Medical School Cohort Study is a prospective, population-based study that includes residents from 12 communities in Japan. 15 The study was approved by the Ethics Committee at Jichi Medical School and all participants provided written informed consent. Baseline data from the participants were collected through health check-up examinations (April 1992–July 1995). The end date of follow-up was 31 December 2005. 15
This study was conducted as an analysis of fractional population with normal FPG for evaluating the FPG/HbA1c ratio in particular (the aim of this study was different from that of the previous work). 16 Included in the study were 1404 participants of the original cohort who had their FPG and HbA1c levels measured. 15 The normal FPG levels were defined as <6.11 mmol/L in this study. 17 We excluded the following patients: 67 with diabetes (defined as FPG levels ⩾6.99 mmol/L, HbA1c levels ⩾6.5%),17,18 151 with FPG levels ⩾6.11 mmol/L, 17 28 with a history of diabetes, and 24 with a history of recent cardiovascular disease or cancer. We also excluded 47 who lacked a record of at least one of the following clinical parameters: body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), or self-reported smoking or drinking habits. After these exclusions, data from 1087 participants (30.8% men (n = 335), mean age of 54.7 years in men and 56.3 years in women) were analyzed.
Baseline survey
The BMI of each participant was calculated using height in stocking feet and weight in light clothing. Measurements of SBP and DBP were performed using a fully automated sphygmomanometer (BP203RV-II, Nippon Colin Co, Ltd, Komaki, Japan). Blood samples were collected in the morning after an overnight fast. Samples for FPG were stored at 4°C in refrigerated dry ice containers for a maximum of 6 h, after which they were analyzed or quickly frozen at −80°C until use. The FPG levels as well as serum total cholesterol, high-density lipoprotein cholesterol, and triglyceride were enzymatically measured (SRL Corp, Tokyo, Japan). The HbA1c level was determined by high-performance liquid chromatography (SRL Corp) and expressed as a National Glycohemoglobin Standardization Program equivalent value using the following formula: HbA1c (%) = HbA1c (Japan Diabetes Society) (%) + 0.4%. Hypertension was defined as an SBP ⩾ 140 mmHg, DBP ⩾ 90 mmHg, and/or antihypertensive drug use. Hypercholesterolemia was defined as a total cholesterol level ⩾5.69 mmol/L and/or cholesterol-lowering medication use. Information regarding cause of deaths was collected using data from death certificates after gaining permission from the Japanese government’s General Affairs Agency.
The levels of FPG, HbA1c, and FPG/HbA1c ratio were divided into tertile groups. For the FPG/HbA1c ratios, groups were defined for men as low <0.85, middle 0.85 ⩽ FPG/HbA1c < 0.93, and high ⩾0.93, and for women as low <0.85, middle 0.85 ⩽ FPG/HbA1c < 0.91, and high ⩾0.91. For FPG levels, groups were defined for men as low <4.9 mmol/L, middle 4.9 ⩽ FPG < 5.4 mmol/L, and high ⩾5.4 mmol/L, and for women as low <4.9 mmol/L, middle 4.9 ⩽ FPG < 5.3 mmol/L, and high FPG ⩾ 5.3 mmol/L. For HbA1c levels, groups were defined for men and women as low <5.7% (38 mmol/mol), middle 5.7 ⩽ HbA1c < 6.0% (46 mmol/mol), and high ⩾6.0%. Variables are shown as mean (including standard deviation) or percentage.
Statistical analysis
In assuming 13% of the incidence rate (approximately 11 years) of all-cause deaths and 2.0 of the risk ratio (in a low-risk group versus high-risk group) in men (with a reference to a study by Kakehi et al. 16 ), the sample size was estimated to be 150 subjects in each group with the alpha-level = 0.05 (5%) and beta-level = 0.20 (power: 80%; two-tailed). Similarly, in assuming 6% of the incidence rate of all-cause deaths and 2.0 of the risk ratio (in a low-risk group versus high-risk group) in women (with a reference to a study by Kakehi et al. 16 ), the sample size was estimated to be 350 subjects in each group. The power analyses were carried out using StatMate 3.0 for Windows (ATMS Co, Ltd, Tokyo, Japan).
The data were compared by a one-way analysis of variance and the chi-square test between the groups. As for all-cause mortality (the primary endpoint), the relationships between the FPG/HbA1c ratio, FPG, HbA1c, and mortality were examined using a Cox proportional hazards model. After adjustment for age and confounding factors (BMI, SBP, total cholesterol, current smoking, and current drinking), the hazard ratio (HR) and 95% confidence interval were calculated for mortality. Statistical significance was defined as P < 0.05. These analyses were carried out using SPSS version 11 (SPSS Inc, Tokyo, Japan).
Results
The mean duration of follow-up was 11.3 ± 4.0 years. Table 1 shows the baseline characteristics of participants grouped by the FPG/HbA1c ratio and sex. The mean ages of men and women were 54.7 (±10.3) and 56.3 (±9.8) years, respectively. In men, BMI, SBP, and FPG values significantly increased as the FPG/HbA1c ratio increased, and HbA1c levels decreased as the FPG/HbA1c ratio increased. In women, SBP, DBP, and FPG values significantly increased as the FPG/HbA1c ratio increased, and HbA1c levels and prevalence of drinking decreased as the FPG/HbA1c ratio increased. The prevalence of smoking, hypertension, and hypercholesterolemia in men and women were not significantly related to the FPG/HbA1c ratio.
Baseline characteristics of participants grouped by the fasting plasma glucose to hemoglobin A1c ratio.
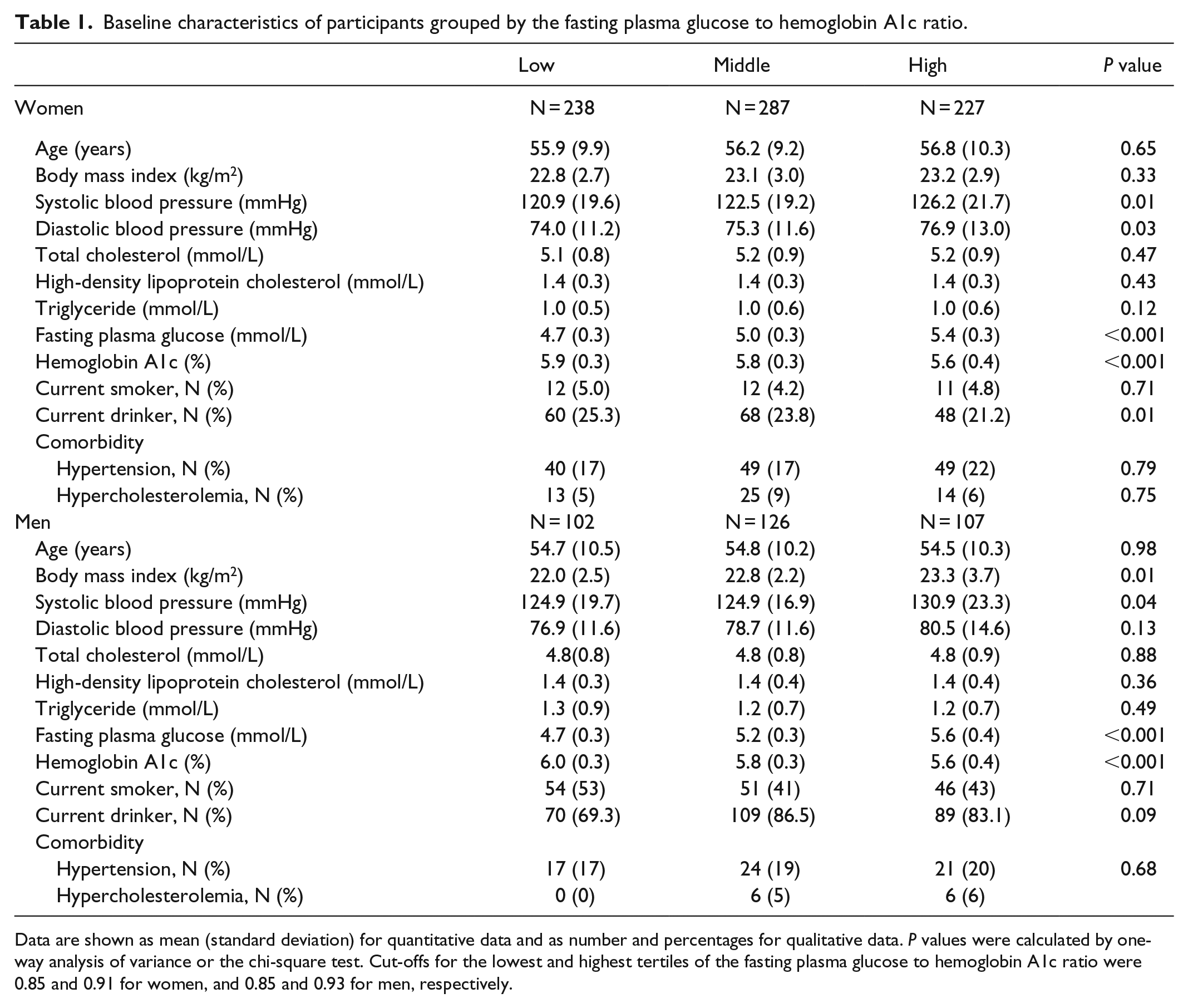
Data are shown as mean (standard deviation) for quantitative data and as number and percentages for qualitative data. P values were calculated by one-way analysis of variance or the chi-square test. Cut-offs for the lowest and highest tertiles of the fasting plasma glucose to hemoglobin A1c ratio were 0.85 and 0.91 for women, and 0.85 and 0.93 for men, respectively.
Table 2 shows the number and proportion of deaths according to cause of death. In total, 25 women and 29 men died during the study. In women, cancer death was the most common, followed by stroke and suicide. In men, cancer death was the most common, followed by heart disease, stroke, and suicide.
Incidence and proportional rate of causes of death.

Incidence expressed per 1000 person-years.
Table 3 shows the HRs for all-cause mortality by FPG, HbA1c, and the FPG/HbA1c ratio. The high FPG/HbA1c ratio tertile group showed a significantly higher HR for all-cause mortality than the low tertile group in women, but not in men. For FPG and HbA1c alone, the HRs for all-cause mortality were not significantly different among tertile groups for either sex.
All–cause mortality grouped by fasting plasma glucose (FPG), hemoglobin A1c (HbA1c), or the FPG/HbA1c ratio.

CI: confidence interval; HR: hazard ratio.
Incidence expressed per 1000 person-years.
Adjusted for age, body mass index, systolic blood pressure, total cholesterol, current smoking, and current drinking.
Cut-offs for the lowest and highest tertiles for FPG were 4.9 and 5.3 mmol/L for women and 4.9 and 5.4 mmol/L for men, respectively.
Cut-offs for the lowest and highest tertiles for HbA1c were 5.7% (38 mmol/mol) and 6.0% (46 mmol/mol) for women and men.
Cut-offs for the lowest and highest tertiles for the FPG/HbA1c ratio were 0.85 and 0.91 for women and 0.85 and 0.93 for men, respectively.
Discussion
This study of a general Japanese population showed that a high FPG/HbA1c ratio predicted all-cause mortality in women, even though the FPG was at the normal levels. The FPG or HbA1c levels alone did not clearly predict all-cause mortality in this population. Thus, women at high risk of all-cause mortality might be identified by the FPG/HbA1c ratio, which could be used as a simple screening laboratory marker in this population.
While the precise mechanisms of a prediction of FPG/HbA1c on all-cause mortality remain unknown, we consider several possibilities. An increase in the FPG/HbA1c ratio can occur with fasting hyperglycemia, which is due to impaired insulin secretion with hepatic insulin resistance and increased hepatic glucose production in the fasting state.11,12,19,20 Thus, individuals with a high FPG/HbA1c ratio might have early impairment in fasting glucose metabolism, leading to an increased all-cause mortality rate.
In this study, all-cause mortality did not significantly but tended to increase with FPG levels alone in a general population of women. Although there is the general knowledge of an increase of mortality with FPG levels, it might not be obviously exhibited by the population restricted to the normal FPG levels in this study. In addition, all-cause mortality did not significantly but tended to decrease with HbA1c levels alone in this study. Several studies report that all-cause mortality increases with very low levels of FPG (<3.89 mmol/L)21,22 and HbA1c (<5.0%). 23 Although the levels can be in some pathological conditions, the mortality–HbA1c relationship might not be obviously presented by few participants with such low FPG and HbA1c levels in the general (healthy) population of this study. 15
An anemic state characterized by low hemoglobin levels is reported to be associated with an increased all-cause mortality rate. 24 Patients with hemoglobinopathies and clinically overt anemia have decreased HbA1c levels compared with FPG levels.25,26 Although we did not assess erythrocyte indices in this study, anemia (such as sickle cell anemia) is rarely observed during routine check-ups for residents in Japan. However, the possible inclusion of individuals with anemia might have influenced our data to a small degree, as in general, women can have slightly more anemia. 27 Anyway, this study showed that HbA1c alone was not a significant predictor of mortality in this population of women.
The Diabetes Epidemiology Collaborative Analysis of Diagnostic Criteria in Asia (DECODA) study reported that postprandial hyperglycemia was a better predictor of all-cause mortality than the FPG. 28 This appears to contradict our current results, as the FPG/HbA1c ratio is possibly low in patients with postprandial hyperglycemia. However, the DECODA study included individuals with FPG levels ⩾6.1 mmol/L, while this study included only those with FPG levels <6.11 mmol/L. The difference in the studied subjects may, thus, have contributed to the findings.
We must consider the sex difference in the ability of the FPG/HbA1c ratio to predict all-cause mortality. For instance, a trend of a decrease of postprandial plasma glucose elevation and/or night-time plasma glucose level in women who often eat less than in men may be mechanistically a contributor (although this is a simple hypothesis). Women with impaired fasting glucose are reported to have increased endothelial dysfunction compared with men,29,30 and this has been linked to various fatal diseases including cardiovascular and cancerous pathologies. 31 Research to explain the sex difference will be further required for screening/clinical use of the FPG/HbA1c ratio as a marker for all-cause mortality.
The study had some limitations. First, as the participants in the study were recruited from the general residents, they were likely to be healthy and less likely to die. 15 Second, the larger sample size was necessary to conclude the gender difference in the finding (especially, men should be more recruited) and discuss the specific cause of mortality. Third, an oral glucose tolerance test (OGTT) was not performed to exclude completely the individuals with pre-diabetes. The studies with a large-scaled sample and inclusion of various measurements (e.g. anemia and OGTT) will be called for in the future.
In conclusion, this community-based cohort study suggests that a high FPG/HbA1c ratio can predict all-cause mortality in women with normal FPG levels in a general check-up setting. To confirm the findings, further studies are warranted.
Footnotes
Author contributions
E.K. and K.Ko. analyzed the data and wrote the manuscript. S.I., T.G., and K.Ka. designed and supervised the study. All authors approved the final version of the paper. E.K. and K.Ko. contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by each municipal government and the Ethics Committee for Epidemiological Research at Jichi Medical School. The institutional Review Board of Jichi Medical School approved the study (epidemiology no. 03-01).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly supported by a Grant-in-Aid from the Foundation for the Development of the Community, Tochigi, Japan.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable because of a simple observational study.