
Abstract
Objective:
The purpose of this study was to evaluate how poor retention in HIV care impacts time to viral suppression after initiating highly active antiretroviral therapy.
Methods:
A retrospective cohort study design, employing a medical chart review, was conducted at an academic infectious disease clinic at the University of Kentucky. Patients seeking care between 2003 and 2011 were included in the study. A log-normal model was employed to determine the factors associated with time to viral suppression.
Results:
Of the 532 patients in the study, 426 (80.1%) patients were virally suppressed. Controlling for insurance status, race, baseline CD4 counts, and viral loads, the expected time to viral suppression for nonoptimal retainers was longer compared to optimal retainers (100% retained in care; time ratio: 2.04; 95% confidence interval: 1.40-2.90).
Conclusion:
Researchers should continue to study the impact of retention on clinical outcomes and strategies to improve retention and reengage those lost to follow-up back into care.
Introduction
Once an individual has been diagnosed with HIV, early linkage to and retention in continuous HIV medical care are arguably the 2 most important components to the continuum of HIV health care which improve the health outcomes of individuals diagnosed and living with HIV. 1 It has been suggested that, in the United States approximately 77% of the individuals diagnosed with HIV are linked into care within 3 to 6 months after diagnosis, but only 51% of those that are linked actually remain in care. 2 Maintaining optimal retention in medical care is required among individuals living with HIV to receive full access to all the treatment benefits. Poor retention in care after initial linkage can be detrimental to an individual’s health as this can delay the initiation of antiretroviral therapy and can lead to more detrimental clinical events, such as virological failure, AIDS, or death. 3 –7
With the major advancements in HIV medical care, HIV has become a manageable chronic infectious disease. Initiating highly active antiretroviral therapy (HAART) into the clinical management of HIV has been shown to dramatically reduce the morbidity and mortality due to HIV, including suppressing viral loads (VL), which in turn reduces the risk of HIV transmission. 8 Gardner et al 1 suggested that approximately 25% of the patients who are eligible to receive HAART are not receiving HAART due to refusal or failure to initiate therapy. Of those who are receiving therapy, it is estimated that only 77% are virally suppressed. With approximately 23% of individuals estimated to be without a suppressed VL, it is believed that barriers to achieving viral suppression among individuals who have initiated HAART are poor medication adherence, nonpersistence, and resistance. 1 Although this may be true, failure to maintain optimal retention in HIV medical care may play a significant role in the failure to achieve a suppressed VL. 8
Poor retention in care represents an arduous obstacle to achieving viral suppression, as this has important individual and public health implications. Little research has been conducted on the impact retention in care has on viral suppression, especially after individuals initiate HAART. 8 –10 Understanding retention in care and how it affects health outcomes among individuals initiating HAART for the first time is very important. Individuals who have been linked to care and initiated HAART for the very first time are at a vulnerable stage in the course of their infection, as they are now expected to attend regularly scheduled clinic visits and sustain near perfect levels of medication adherence, and these individuals may not be prepared for the long-term commitment that is attached to HIV care.
The purpose of the study is to determine the impact retention in care has on viral suppression after initiating HAART. Employing parametric time to event methods, the hypothesis is that poor retention in care after initiation of HAART will delay time to viral suppression.
Methods
Study Design
A retrospective cohort study design, employing a medical chart review, was conducted at the Bluegrass Care Clinic, an academic infectious disease clinic at the University of Kentucky, to determine the impact retention in HIV medical care has on time to viral suppression. Patients who sought care between 2003 and 2011, and had initiated HAART anytime during the course of their infection, were considered eligible for this study and were followed until December 31, 2011. In this study, patients were followed from initiation of HAART until the event of interest occurred (viral suppression) or until the end of the study period (December 31, 2011), death, or movement out of the service region. The study was approved by the University of Kentucky Institutional Review Board.
Study Population and Eligibility
Data were abstracted from an electronic database. For the current study, patients who were seeking HIV medical care during the study period were ≥18 years of age at the time of the study and patients who had initiated HAART at any time during the course of their infection were considered eligible for the study. To be included in the current study, patients had to have at least 1 HIV outpatient medical clinic visit during the specified study period (not including initiation of HAART), an initial VL measurement with an actual date of result, a subsequent VL measurement with an actual date attached, and a follow-up greater than 6 months. Restricting the study to patients that have a follow-up greater than 6 months allows time for patients to obtain a subsequent VL measurement so that suppression can be observed.
For the time to viral suppression study, patients that had a VL measurement of <50 copies/mL at the time of the study were excluded from the analysis. There were 1166 patients that had initiated HAART and were eligible for the study, with 1108 (95%) having at least 1 VL recorded. Of the 1108 patients with at least 1 VL recorded, only 973 (88%) patients had a VL with a date recorded. For time to viral suppression, patients were excluded from the analysis of the study if they had achieved a suppressed VL (<50 copies/mL) prior to start of the study. Of the 973 patients with a VL recorded during the study period, 532 (56%) had a VL that was >50 copies/mL at initiation of HAART and were included for the analysis.
Study Measures
Demographic and clinical data were abstracted from the medical records of the patients included in the study. Demographic information collected during the study included date of birth, sex, race/ethnicity (white/nonwhite), marital status, employment status, insurance status, poverty level (<100% below federal poverty level), history of tobacco and illicit drug use (yes/no), and transmission category (men who have sex with men [MSM], heterosexual contact, injection drug users, and other). The clinical characteristics obtained included CD4 counts, VLs, history of hepatitis C, date of HAART initiation, and date of death.
Retention in Care Measure
According to the current Department of Health and Human Services guidelines, newly diagnosed individuals should seek HIV medical primary care at least every 3 to 4 months until their immunological and virological response has been maintained at the appropriate levels, and then once every 6 months after that. 11 Patients living with HIV who initiate HAART should be monitored consistently, so that the patient can maintain adherence and viral suppression. Retention in care was defined as having at least 1 HIV medical outpatient clinic visit every 6 months. Patients were considered optimally retained in care if all 6-month patient care intervals had at least 1 clinic visit completed.
Outcome Measures
The primary end point of the study was viral suppression and was defined as having an HIV RNA level of <50 copies/mL. Time to viral suppression (years) was defined as the time from the initiation of HAART to the time of the first suppressed VL.
Statistical Analysis
Descriptive statistics were produced to describe the study population by employing means, medians, standard deviations, and ranges to describe all the continuous variables and frequencies and percentages to describe all the categorical variables. Independent 2 sample t tests and Wilcoxon tests were used to detect differences in continuous variables, while chi-square tests were used to determine differences in categorical variables.
For the analysis of time to event data in most epidemiologic studies, in particular HIV studies, the Cox proportional hazards model has become the model of choice, but it has been argued that parametric methods such as the accelerated failure time (AFT) model may provide a more appropriate modeling framework. 12,13 Advantages to employing parametric models are (1) ability to use full maximum likelihood to estimate parameters; (2) the estimated coefficients can provide estimates that may be clinically meaningful; (3) estimates of survival time can be provided from fitted values from the model; and (4) residuals can be computed as differences between observed and predicted values of time. 13,14 To determine the impact retention has on time to viral suppression, AFT methods were employed.
In the time to event analysis for VL suppression, time was measured from the start of HAART and analysis time ended at the earliest date of a suppressed VL or at the end of the study period, death, or movement out of the service region. Those individuals who did not achieve VL suppression or died were right censored at the end of the study. Since the authors were unaware of the exact date of viral suppression between VL dates, interval censoring was also employed between the date of viral suppression and the previous VL date. Kaplan-Meier estimates were plotted overall and stratified by retention in care. Wilcoxon tests were used to determine the differences in survival curves between the retention groups and the other covariates. 13,14
The primary objective was not to determine just the risk of VL suppression but to determine how early retention impacted time to VL suppression. Parametric survival models, in particular AFT models, were considered for the current analysis because the acceleration factor allows us to evaluate the effect of the predictor variables (retention) on the survival time as opposed to the hazard like the proportional hazard models. 13,14 Cox-Snell residual plots were produced to determine absolute goodness of fit for the parametric model. For time to VL suppression, the log-normal model was chosen. Variables with a P value ≤.15 in the univariate analysis were considered for inclusion into the final model. To determine how retention in care impacted time to viral suppression, the model controlled for insurance status, race, CD4 counts at baseline, VL at baseline (log copies), income, history of AIDS, and year of HIV diagnosis. Time ratios were the measures of association for this analysis.
All data were analyzed using SAS version 9.3 (Cary, North Carolina), and P values <.05 were regarded as statistically significant.
Results
Demographic Characteristics
For the study sample (n = 532), the mean age at the start of HAART was 39.2 ± 9.35 years. The majority of the patients were men (81.0%) and white non-Hispanic (73.3%). The majority of the patients’ reported mode of transmission was MSM (57.0%), and 49.6% of the cohort were living below the poverty level (Table 1).
Association of Sociodemographic and Clinical Characteristics and Viral Suppression among the Patients Seeking HIV Medical Care and Initiating HAART at the Bluegrass Care Clinic, 2003 to 2011.

Abbreviations: HAART, highly active antiretroviral therapy; IDU, injection drug user; MSM, men who have sex with men; SD, standard deviation.
At the start of the study, approximately 39.2% of the patients did not have any form of insurance, with 34.3% having some form of public assistance (Medicaid or Medicare). The median CD4 count at initiation was 357.2 (1, 1690) cells/mm3, and the mean log VL was 7.3 ± 3.2 copies. At the end of the study period, approximately 53% of the patients were optimally retained in care (Table 1).
A total of 426 (80.1%) patients achieved a viral suppression at least once during the study period. Those with a suppressed VL were more likely to be white non-Hispanic (76.5% versus 60.4%, P = .001) and those with private insurance (28.7% versus 17.9%, P = .001). The patients with a suppressed VL were less likely to be those living below the federal poverty level (47.7% versus 57.6% P < .0001) and those on Medicaid (13.7% versus 27.4%) and no insurance (38.4% versus 42.5%, P = .001; Table 1).
Clinically, those with a suppressed VL were more likely to have a higher median CD4 count (385.6 versus 242.0 cells/mm3, P < .0001) and more likely to have a lower mean log VL at initiation (6.8 versus 9.1 log copies, P < .0001). Viral suppression was also found to be less likely in those patients that were not optimally retained in care throughout the study period (41.1% versus 68.9%, P < .0001; Table 1).
Time to Viral Suppression
Figure 1 presents the Kaplan-Meier curve for the 426 patients that achieved a viral suppression, with those patients who did not being right censored (n = 106). The curve suggests a faster progression within the first year of initiation to HAART, followed by a much slower progression as the time increases. The median time to viral suppression for the patients was approximately 1.03 years. Figure 2 presents a Kaplan-Meier curve of time to viral suppression stratified by retention in care. The curve suggests that the patients who were optimally retained in HIV medical care after the initiation of HAART had a shorter time to viral suppression compared to those who were not optimally retained in care. The median time to viral suppression for optimal and nonoptimal retainers was 0.87 and 1.79 years, respectively (Wilcoxon test, P = .002). The estimated cumulative survival distribution for the log-normal distribution was produced for optimal and nonoptimal retainers. The curves show results similar to the Kaplan-Meier curves that optimal retainers have a higher chance of viral suppression compared to the nonoptimal retainers (Figure 3).

Kaplan-Meier curve of time to viral suppression among the patients initiating highly active antiretroviral therapy (HAART).
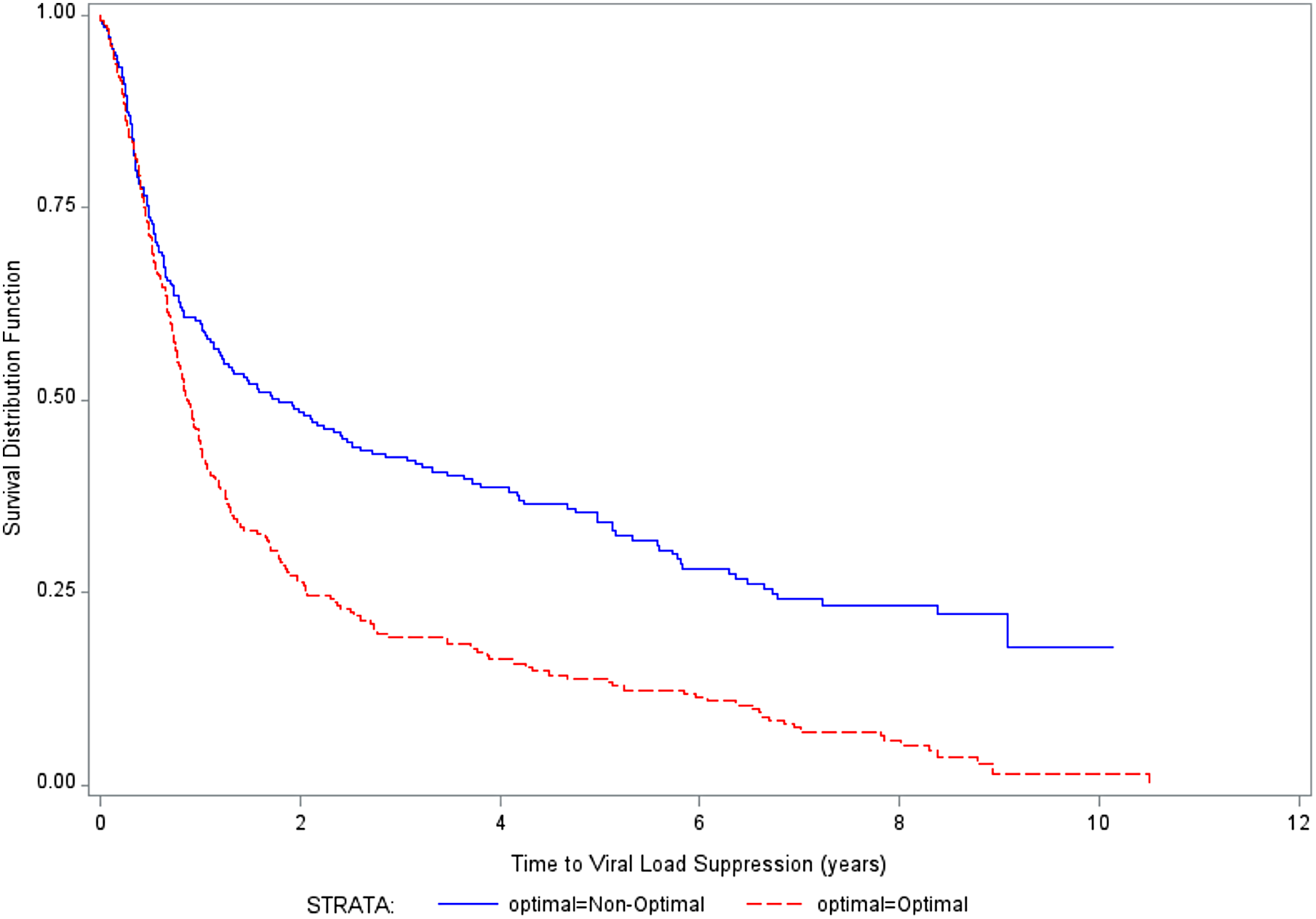
Kaplan-Meier curves of the time to viral suppression stratified by optimal retention.

Estimate cumulative incidence curves of time to viral suppression for the log-normal distribution.
In the log-normal models, the association with viral suppression was tested for all the variables in the univariate models, and those with a P value <.15 in the unadjusted model were included in the adjusted model. In the unadjusted log-normal model, nonoptimal retainers, those on Medicaid, and those with an AIDS diagnosis had longer times to viral suppression compared to their counterparts (Table 2). Controlling for insurance status, race, baseline CD4 counts, and baseline VLs, the expected time to viral suppression for nonoptimal retainers was 2.04 (95% confidence interval [CI]: 1.40-2.90) times greater than those who were optimally retained in care. The expected time to viral suppression for those Medicaid was 2.06 (95% CI: 1.08-3.95) times greater compared to those with private insurance, and those without an AIDS diagnosis had a shorter time to viral suppression compared to those with an AIDS diagnosis (time ratio =0.59; 95% CI: 0.37-0.94; Table 2).
Log-Normal Regression Determining the Association between Retention in HIV Medical Care and Time to Viral Suppression among the Patients Seeking Care at the Bluegrass Care Clinic: 2003 to 2011.a

Abbreviations: TR, time ratio; CI, confidence interval. aBold numbers signify P values < .05.
Discussion
The purpose of this study was to understand the effect retention in care had on viral suppression among individuals receiving HAART. There is a paucity of research on the examination of the effect of retention in HIV medical care on time to viral suppression. For time to viral suppression, the authors selected a small cohort of patients who were initiating HAART for the first time and followed them from the time of HAART initiation to the time of their first suppressed VL. Retention in care was shown to be associated with time to viral suppression. Patients that had optimal (100%) retention after initiating HAART were more successful in achieving a suppressed VL, and the time it took for suppression was much shorter than the patients who were poorly retained in care. The results from this study are consistent with those of Mugavero et al, 8 which observed the impact early retention (number of missed visits in the first year of care) had on viral suppression, and they were able to show that patients with perfect visit adherence were more likely to have a viral suppression, and that each “no show” clinic visit conveyed a 17% increased risk of delayed viral suppression.
The results of the current study convey important implications for individual patient outcomes as well as future public health prevention efforts. Failure to achieve viral suppression in a timely manner and maintain a suppressed VL can be damaging to the individual’s health; the longer it takes for an individual living with HIV to suppress their VL, the risk of detrimental clinical events increases. Researchers have suggested that failure to suppress one’s VL can be an indicator of poor medication adherence as well as medication resistance. 1,5,15
From a public health standpoint, failure to achieve viral suppression can be damaging to prevention efforts, as patients with high VLs may increase the risk of HIV transmission. In 2008, Metsch et al 16 conducted a study to show how recently diagnosed patients with optimal early retention in care had reductions in sexual risk behaviors compared to those who were poorly retained. The authors were able to show that poor retention in HIV care, among individuals who had initiated HAART, was a barrier for timely viral suppression, which in turn impedes the potential reduction in transmission of HIV to others. This shows the importance of retention in care among individuals living with HIV and strategies should be developed to help reengage those individuals who have fallen out of care as this can improve their chances of viral suppression.
The patients in the study with Medicaid had challenges in achieving timely viral suppression. Even when controlling for the other variables in the parametric model, patients with Medicaid had delays in viral suppression. The Medicaid population has been consistently shown by researchers to be poor retainers in care, poor viral suppressers, and viral rebounders. 17 –19 Studies should be conducted on this population to get a better sense of why retention is poor, which can then lead to poor HIV outcomes. Understanding the factors that prevent this population from retaining in care and suppressing VLs can help guide future prevention efforts to reengage this population back into care.
This study was an observational, retrospective cohort study and subject to potential uncontrolled confounders for which the authors had no information, such as alcohol use and presence of social and familial support networks. A medical chart review was employed to capture patient’s data, and not all the patients had complete information in their medical records. This was the case for selecting patients for inclusion into the study who had a VL and a follow-up measurement; 193 patients were excluded from the analysis partly because they had missing information regarding their HIV laboratory test results (eg, VL recorded but no date or a VL date but no VL result). There were no significant differences between those that were excluded from the analysis in regard to demographic information, but exclusion of patients reduces the power of the study and potentially introduces bias. Although the study clinic provides care for a large proportion of individuals diagnosed with HIV who reside in central and eastern Kentucky, the results may not be generalizable to all Kentuckians living with HIV nor all individuals living with HIV in the United States. A future research study conducted using similar methods should involve a multicenter study across all Ryan White funded clinics in Kentucky.
Another limitation to this study was the definition for retention. In the retention in care literature, it is debated as to what constitutes a clinic visit. For this study, retention was defined as having at least 1 HIV medical primary care visit every 6 months. This limitation could lead to a misclassification bias, as individuals who seek medical care from non-HIV providers may be classified as poor retainers, therefore, overestimating non-retainers in the study. There is a potential for selection and misclassification bias, as individuals were removed from the study when they did not have at least 6 months of follow-up. Removing these individuals from the analysis may underestimate the number of poor retainers seeking medical care at the Bluegrass Care Clinic. It was not feasible to find out whether these individuals were seeking HIV medical care at other clinics. The authors do not believe patients would seek care at other clinics, often because most of the patients relied on funding from the clinic for medication and patient care, and other options for HIV/AIDS care in their region may be limited.
Finally, medication adherence was not observed or evaluated for this study. Studies have observed the impact medication adherence has on viral suppression and have suggested that patients that are not at least 95% adherent to their medications are more likely to have virological failures. Medication adherence is on the causal pathway between retention in care and VL suppression, but the purpose of this study was to establish the relationship between retention and VL suppression. 20 It may be concluded that medication adherence is the driving force behind viral suppression, but Giordano et al 5 were able to show that poor retention in care and poor medication adherence were highly correlated; therefore, it seemed appropriate to use retention in care as a surrogate measure. Also with this study, obtaining medication adherence was difficult as the patient population at the clinic obtain their medications from multiple pharmacies, which makes it difficult to track medication pick up once the prescription has been written.
Conclusion
In conclusion, the authors were able to identify significant associations between retention in care and viral suppression among patients initiating HAART. Patients who were poorly retained in care after initiating HAART prolonged their opportunity to achieve viral suppression compared to optimal retainers in care. The results of this study stress the importance of maintaining optimal retention among individuals living with HIV in order to increase the number of individuals with suppressed VLs. Researchers and clinicians should continue to study the impact of retention in HIV medical care on clinical outcomes and strategies to improve retention and reengage those lost to follow-up back into care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.