
Abstract
Objective:
The aim of this study is to estimate the proportion of virologically suppressed People living with HIV on second-line ART and to identify factors associated with virologic suppression. With an increasing population of patients on complex second-line anti retroviral therapy (ART), understanding the factors associated with viral suppression and adherence is critical for ensured longevity of ART.
Methods:
A retrospective study was conducted of patients on second-line ART in 17 facilities supported by University of Maryland, Baltimore, in Nairobi, Kenya, covering the period beginning October 2016 up to August 2019. Viral suppression was defined as viral load <1000 copies/mL in a test conducted in the last 12 months. Adherence was assessed through self-reports and classified as optimal (good) or suboptimal (inadequate/poor). Associations were presented as adjusted risk ratios with 95% confidence intervals. Statistical significance was considered when p value ⩽0.05.
Results:
Of 1100 study participants with viral load data, 974 (88.5%) reported optimal adherence while on first-line ART and 1029 (93.5%) reported optimal adherence to second-line ART. Overall, viral load suppression on second-line ART was 90%. Optimal adherence ((adjusted risk ratio) 1.26; 95% confidence interval 1.09–1.46)) and age 35–44 versus 15–24 years ((adjusted risk ratio) 1.06; 95% confidence interval 1.01–1.13)) were associated with viral suppression . Adherence to first-line ART ((adjusted risk ratio) 1.19; 95% confidence interval 1.02–1.40)) was associated with adherence to second-line ART.
Conclusion:
Viral suppression remains high and adherence was strongly associated with viral suppression, underscoring the need to adequately address the barriers to adherence before switching regimens.
Introduction
In Kenya, antiretroviral therapy (ART) scale-up helped avert more than an estimated 635,000 AIDS-related deaths between 2004 and 2017. 1 The significantly reduced morbidity and mortality attributed to widespread use of ART highlights the importance of sustained drug adherence and retention in treatment programs, especially now that people living with HIV (PLHIV) are living longer. Clients with optimal adherence are less likely to experience non-viral suppression, 2 and those with suboptimal adherence on first-line ART are more likely to have issues with adherence on second-line ART if they switch regimens. 3
Multiple factors have contributed to clients failing second-line ART treatment in Kenya. The most impactful factor is poor adherence, which may be caused by stigma; other factors include lack of disclosure, long travel distances to clinics, and mental health disorders.4–7 The Kenya National guidelines on Anti-Retroviral (ARV) use 8 prescribe tailored interventions prior to switching to second-line treatment, including intensive adherence counseling, home visits to assess clients’ living situations, and medication storage. Other interventions include directly observed treatment (DOTs) in which the client is observed swallowing their medication each day, psychosocial support groups, and case management by peer educators who are expert clients. These interventions, along with formulation of viremia support groups and specific viremia clinic days, have shown benefits by increasing VS rates. 9
Despite a high number of individuals receiving ART in Kenya, HIV drug resistance is a growing concern. To better manage and control drug-resistant HIV, it is crucial to identify PLHIV who are not virally suppressed and quickly switch those clients to a second-line ART regimen. 10 Viral load (VL) monitoring allows healthcare workers to identify such patients, as persistent VL non-suppression is an indicator of poor treatment outcome. 10 Due to the limited availability of treatment options such as absence of third-line ART in many resource constraint setting, exploring potential factors associated with adherence remain critical.11,12
While an increasing number of PLHIV are accessing ART, limited information exists regarding non-suppression rates amongst patients on second-line ART treatment in Kenya and many resource-limited settings in general. The aim of this study is to estimate the proportion of virologically suppressed PLHIV on second-line ART and identify factors associated with virologic suppression using program data from 17 healthcare facilities in Kenya from October 2016 up to August 2019. Understanding factors associated with ART adherence and non-viral suppression will assist in devising interventions to address potential barriers for these outcomes.
Methods
Study design and population
We implemented a retrospective cohort study to evaluate factors associated with second-line ART viral suppression from October 2016 to August 2019. The study population consisted of PLHIV who are ⩾15 years old and on second-line ART for at least 6 months from 17 University of Maryland, Baltimore-supported healthcare facilities in Nairobi, Kenya. Specifically, those PLHIV who are 15 years or older, on second-line ART, had 12 months viral load data were included in our primary analysis. Those who were younger than 15 years and/or had no viral load data were excluded. We chose to include patients who are 15 years or older because these patients are considered to have taken ownership of their treatment, and among adolescents, full disclosure of their HIV status has been completed. Healthcare facilities offer treatment according to the Kenya Ministry of Health guidelines. 8 The drugs used for second-line ART depended on the first-line ART regimen of each patient. For patients on Zidovudine (AZT) in first-line ART, the default second-line option was tenofovir disoproxil fumarate (TDF) combined with lamivudine (3TC) and lopinavir and ritonavir (LPV/r) or atazanavir and ritonavir (ATV/r). For those who had received TDF in first-line ART, the second-line option was an AZT-based regimen combined with 3TC and LPV/r or ATV/r. An alternative second-line option for those unable to tolerate TDF was abacavir (ABC) combined with 3TC and LPV/r or ATV/r.
Data collection
As part of routine HIV clinical care, all patient data, including demographics and medication use, ART regimen, ART initiation date, ART switch dates, duration on ART, and self-reported adherence, were collected from patient registers, patient charts, and electronic medical records (EMRs). The data capturing sheet was used to collect patient information, such as demographics, self-reported adherence, ART medications, viral load, and body mass index. It was used to extract patient data from patient charts and viremia registers. For facilities with EMRs, data were queried to retrieve patient information. De-identified patient data from EMRs and data extracted from patient charts and viremia registers were combined into a single dataset that was used for analysis.
Definition of variables
The primary end-point was second-line ART viral suppression, defined as VL <1000 copies/mL, recorded from a VL test conducted and with results documented in the client medical records in the last 12 (11.5–12.5) months. There was no baseline viral load data. Adherence was assessed through self-reports that were routinely collected in patient medical records and documented as poor, inadequate, or good based on missed doses per month whereby 1 to 3 missed doses is rated as good, missing 4 to 8 doses is rated inadequate, and missing over 9 doses is rated as poor. Adherence assessment conducted on the patient’s last visit was used in this study. For the purposes of this analysis, self-reported adherence was classified as optimal adherence for those with good adherence or suboptimal for those reporting a poor/inadequate level of adherence. Other variables evaluated included age, gender, BMI, regimen type, timing of switching to second-line ART, and duration on ART.
Sample size and power
The sample size was calculated using a single population proportion formula with the assumption of a 95% confidence interval, 5% margin of error, 80% power, and 90% of patients achieving viral load suppression while on second line as previously described. 13 Based on these assumptions, the sample size needed was 138 patients. By using all routinely collected patients with viral load data while on second-line ART (n = 1100), we had >80% power to verify a proportion of patients who achieved viral suppression.
Statistical analyses
Frequencies of categorical variables were calculated as the proportions of patients sampled. Adjusted binomial regression models were used to assess the association of different factors with VS on second-line ART. Multivariate models included variables that were statistically significant on bivariate and pre-specified, biologically plausible factors of interest. A binomial regression model was also used to assess the association between adherence to first-line ART and adherence to second-line ART using patients with adherence data on second line. For primary analysis, a complete case analysis was performed. Then, multiple imputation for the missing data was done as sensitivity analysis. All associations were presented as adjusted risk ratios (aRRs) with 95% confidence intervals (CIs). Statistical significance was considered when p value ⩽0.05. SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.
Results
Of 1486 participants on second-line ART, 1380 (92.9%) were 15 years or older. Of these, 1100 (79.7%) had VL data while on second-line ART 810 (73.6%) were 25 years or older, and 802 (72.9%) were female and 427 (38.8%) switched to second line >90 days from when non-viral suppression was documented (Table 1). The median age (interquartile range) was 31 (26–38) years. The majority, 1029 (93.5%), reported optimal adherence to second-line ART, and 974 (88.5%) reported optimal adherence while on first-line ART. Overall, VL suppression on second line was achieved by 990 (90.0%) patients.
Characteristics of people living with HIV attending 17 healthcare facilities in Nairobi, Kenya, 2016-2019.
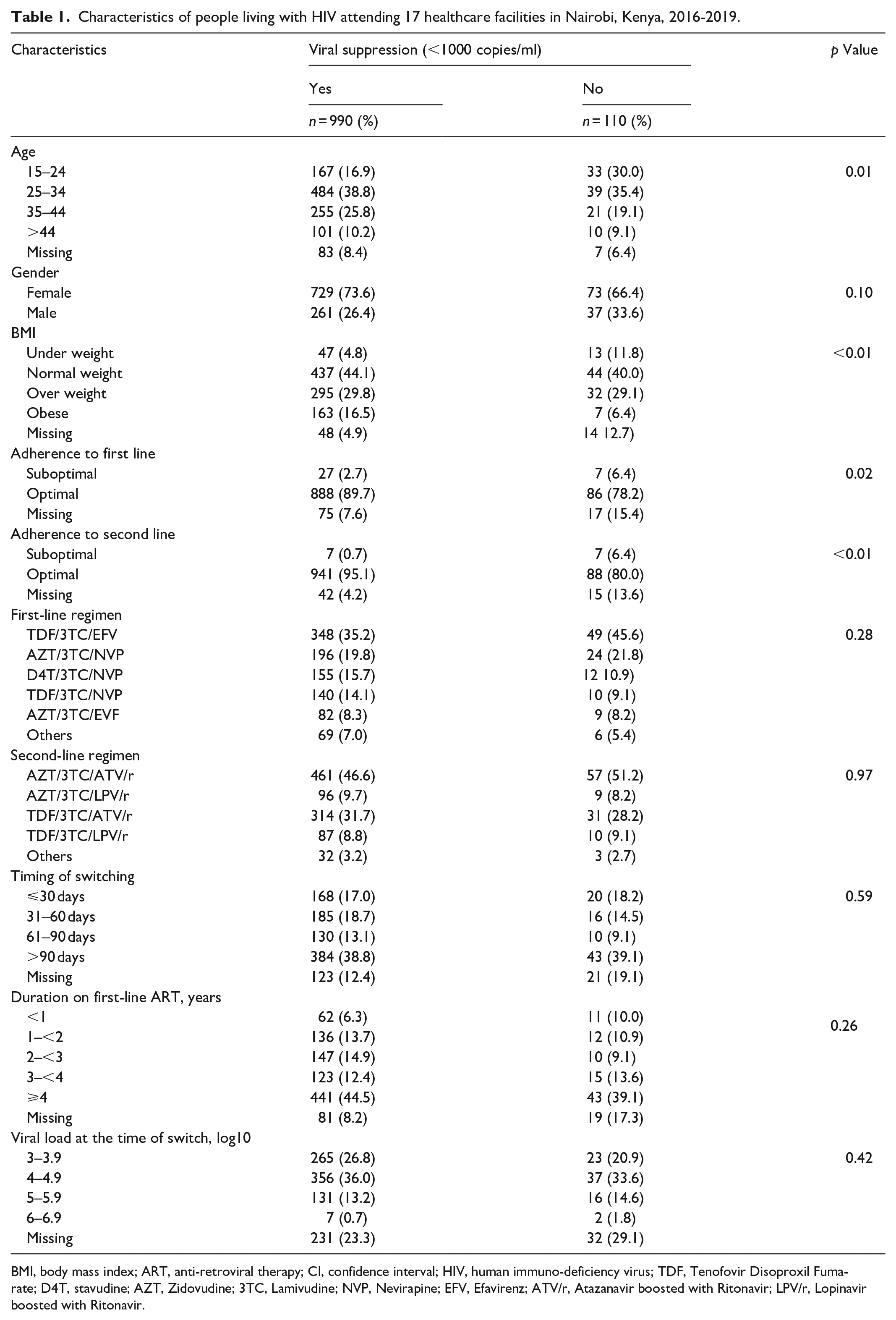
BMI, body mass index; ART, anti-retroviral therapy; CI, confidence interval; HIV, human immuno-deficiency virus; TDF, Tenofovir Disoproxil Fumarate; D4T, stavudine; AZT, Zidovudine; 3TC, Lamivudine; NVP, Nevirapine; EFV, Efavirenz; ATV/r, Atazanavir boosted with Ritonavir; LPV/r, Lopinavir boosted with Ritonavir.
Factors associated with viral suppression
Compared to patients on second-line ART with suboptimal adherence, those with optimal adherence were more likely to be virally suppressed (adjusted risk ratio, (aRR) 1.26; 95% CI 1.09–1.46)) (Table 2). Compared to patients who were 15–24 years, patients who were 35–44 years were more likely to be virally suppressed (aRR 1.06; 95% CI 1.01–1.13). Second-line regimen type, timing of the switch after non-viral suppression was documented, and VL at the time of switch were not significantly associated with VS.
Risk factors of viral suppression among HIV-infected patients on ART at healthcare facilities in Nairobi, Kenya.

ART, antiretroviral therapy; CI, confidence interval; HIV, human immunodeficiency virus; RR, risk ratio; TDF, Tenofovir Disoproxil Fumarate; AZT, Zidovudine; 3TC, Lamivudine; ATV/r, Atazanavir boosted with Ritonavir; LPV/r, Lopinavir boosted with Ritonavir. Bolded; statistically significant.
Sensitivity analysis on factors associated with viral suppression
When missing data for predictor variables were imputed and data re-analyzed, association between adherence to second line and viral suppression persisted. Those with optimal adherence continued to be virally suppressed compared to those with suboptimal adherence (aRR 1.47; 95% CI 1.01–2.15) (Table 3).
Sensitivity analysis on risk factors of viral suppression among HIV-infected patients on ART at healthcare facilities in Nairobi, Kenya.

ART, antiretroviral therapy; CI, confidence interval; HIV, human immunodeficiency virus; RR, risk ratio; TDF, tenofovir disoproxil fumarate; AZT, zidovudine; 3TC, lamivudine; ATV/r, atazanavir boosted with ritonavir; LPV/r, lopinavir boosted with ritonavir. Bolded; statistically significant.
Factors associated with adherence to second-line ART
Participants who had optimal adherence to first-line ART continued to have optimal adherence to second-line ART (aRR 1.19; 95% CI 1.02–1.40) (Table 4). Other factors, including age, gender, and regimen type, were not significantly associated with adherence to second-line ART.
Factors associated with Adherence to second-line ART among HIV-infected patients at infectious disease clinics in Nairobi, Kenya.
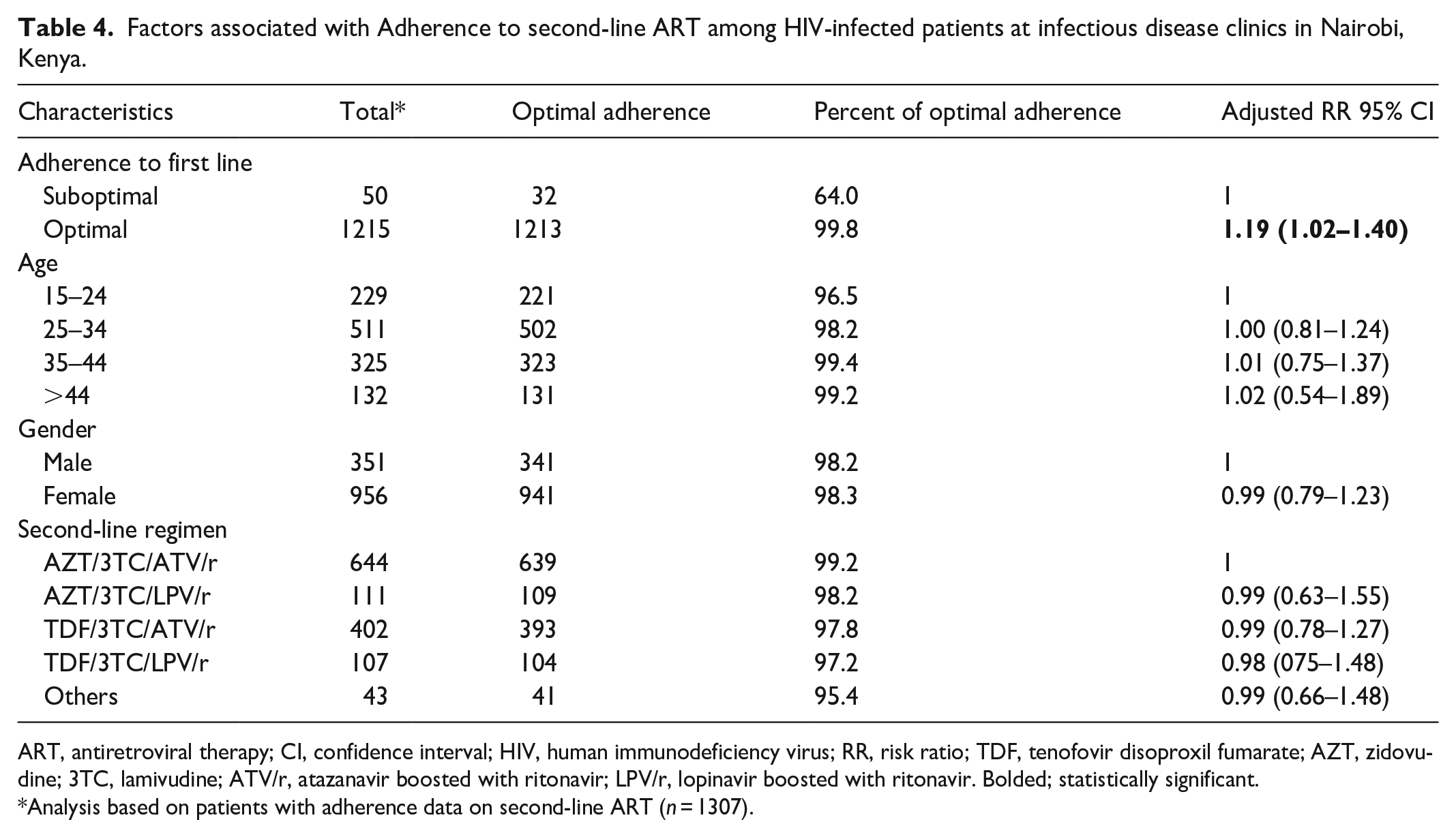
ART, antiretroviral therapy; CI, confidence interval; HIV, human immunodeficiency virus; RR, risk ratio; TDF, tenofovir disoproxil fumarate; AZT, zidovudine; 3TC, lamivudine; ATV/r, atazanavir boosted with ritonavir; LPV/r, lopinavir boosted with ritonavir. Bolded; statistically significant.
Analysis based on patients with adherence data on second-line ART (n = 1307).
Discussion
As the HIV program matures, the number of patients requiring second-line treatment and subsequent third-line treatment is steadily increasing. In this cohort of PLHIV on second-line ART from various HIV care facilities in Nairobi, Kenya, 90% had achieved VS, with 93.5% achieving optimal drug adherence on second-line treatment. This level of VS is similar to the national percentage of 92% in 2019 14 but lower than the UNAIDS 95-95-95 goal of 95% of PLHIV on treatment having VS by 2030. 15
ART adherence is an important factor in VL suppression. Overall, adherence to ART for this cohort improved from 88.5% on first-line ART to 93.5% on second-line ART, and patients with optimal adherence to first-line ART were more likely to have optimal adherence to second-line ART. An improvement of VL suppression during second-line could be due to three successive enhanced adherence counseling implemented among patients with non-viral suppression on first-line ART as recommended by Kenya ART guidelines. 8 Of the 50 patients who reported suboptimal adherence to first-line ART, 18 (36%), continued to have suboptimal adherence to second-line ART. A similar association between first-line ART and second-line ART has been shown in Tanzania, in which approximately 36.3% of patients who had suboptimal adherence to first-line ART had suboptimal adherence to second-line ART. 3
Emphasis on optimal adherence to ART remains critical. Prior work in Kenya has shown that, among patients who had non-viral suppression on second-line treatment, 27% were in need of switching to a third-line treatment regimen and 25% have exhausted all first- and second-line treatment regimens due to HIV drug resistance. 16 Failing second-line ART will necessitate switching to third-line ART. Third-line ART, or salvage regimens, are often unavailable or unaffordable, 17 which becomes especially problematic in low- and middle-income countries. Unavailability of third-line treatment options for those in need in these settings has negative implications to both patients and the population in general. First, patients continuing therapy on failed regimens are at high risk of developing opportunistic infections and increased risk of death. Secondly, high VL among these patients increases risk of HIV transmission to uninfected individuals.
Adherence to ART was also associated with VS, as those who were optimally adherent to treatment were statistically significantly more likely to be virally suppressed. This corresponds with previous research. In a meta-analysis, Bezabhe et al. 2 found that patients with optimal adherence had a lower risk of non-viral suppression. Another study on non-suppression in Uganda also found that those with suboptimal adherence were more likely to face virologic non-suppression. 18 In addition, it has been found that those who switch to a second-line regimen due to non-compliance reasons are less likely to reach VS. 19 These findings highlight the importance of adherence interventions, especially with patients being switched to second-line treatment who may have unresolved barriers to treatment. The role of continued counseling on the importance of regular and consistent use of medication is, therefore, critical.
Of note, younger individuals were less likely to be virally suppressed—hence the need for a more comprehensive approach to care designed to assess and improve adherence and VS among these patients. Other studies have found similar results. A study from western Kenya found that younger age was associated with viral load levels >1000 copies/mL, 20 and a study from Uganda found that children and adolescents had the highest odds of viral non-suppression. 18 As adherence and VS are closely linked, it is important to understand why young people may be having difficulty reaching VS, especially if there are any barriers related to adherence. Some barriers of optimal adherence in young people include a lack of awareness regarding the importance of ART and its benefits, depression, stigma from family and friends, and forgetting to take medication.21–23 In addition, youth attending boarding schools may feel an increased sense of stigma while living amongst their peers and trying to hide their medication or opting to take their medication in secret. 24 Thus, many physical, psychological, and social issues may interfere with optimal adherence to complicated ART regimens among adolescents and young adults. Patient and healthcare level interventions to improve adherence and treatment outcome among young individuals have been tested and a few such as intensive home-based case management, peer support, special adolescent’s clinic hold promise in young individuals.25,26
In 2015, the World Health Organization (WHO) recommended dolutegravir (DTG) as an alternative first-line regimen for adults and adolescents. DTG has been the drug of choice for people living with HIV because it has few side effects, it is easier to take, and patients are less likely to develop resistance. 27 Kenya approved the use of DTG since 2018. 8 Despite the benefits of this new regimen, efforts to emphasize the need to be consistently adherent to treatment should not be underscored. Reports showed that reasons for non-viral suppression among DTG users are similar to those of previous drug formulations. These include low CD4 count and high baseline viral load. 28 Moreover, non-viral suppression has been reported as high as 9.2% among PLHIV-initiated DTG-based regimen. 29 These data highlight the need to support adherence to ART among PLHIV.
Several other factors such as HIV-associated stigma, pill burden, and insufficient support have been documented as barriers to ART adherence.30,31 Although not assessed in this study, it is worth emphasizing the need to increase social support, continued counseling, and status disclosure. These measures have proven benefit in improving patient adherence and viral suppression.32,33
Our study has several limitations. We used self-reported adherence documented in the patient charts by the clinicians, which is subject to overestimation of adherence assessments. 34 This may be confounded by social desirability bias, as patients may feel the need to exaggerate true adherence. 2 In addition, there could be other potential risk factors for not achieving VS which this paper was not able to address because analysis was done on routinely collected facility data. These factors include insufficient support structure, pill fatigue, and stigma that could be further studied. Duration on treatment is a potential variable to explore as patients who have been on treatment at different duration may differ; however, this variable was not collected. Although duration on treatment was not available, we explored viral load data at the time of switch which showed that patients with higher viral load were less likely to be virally suppressed although the association was not statistically significant. Furthermore, we did not have data to explore VS among adolescents and young individuals by comparing those who were perinatally infected from those who are vertically infected.
Future research
While this study demonstrates factors associated with VS among patients on second-line ART, results from larger, multisite adherence programs should be examined. Further research could examine the impact of psychosocial and other factors that impact adherence to inform interventions. Specifically, interventions to improve adherence while also addressing many of the contextual variables that impact adherence, such as stigma, disclosure, depression, and other opportunistic infections are warranted. Adherence interventions specific to adolescents and young adults should be considered.
Conclusions
The current Kenya ART guidelines for HIV control focus on improving the continuum of HIV care from diagnosis to VS, and medication adherence is an important part of HIV care and maintaining VS. Our findings indicate that VS remains high despite the complexity of second-line ART regimens, including multiple pills, drug-to-drug interactions, and adverse effects. In this population, adherence was strongly associated with VS; hence, those with suboptimal adherence was at greater risk of non-suppression, underscoring the need to adequately address the barriers to adherence before switching regimens and consistently monitoring patients who switch regimens.
Supplemental Material
sj-xlsx-1-smo-10.1177_20503121231162354 – Supplemental material for Factors associated with adherence and viral suppression among patients on second-line antiretroviral therapy in an urban HIV program in Kenya
Supplemental material, sj-xlsx-1-smo-10.1177_20503121231162354 for Factors associated with adherence and viral suppression among patients on second-line antiretroviral therapy in an urban HIV program in Kenya by Rose Nyaboke, Habib Omari Ramadhani, Taylor Lascko, Patrick Awuor, Elvis Kirui, Emily Koech, Immaculate Mutisya, Carol Ngunu and Rebecca Wangusi in SAGE Open Medicine
Footnotes
Acknowledgements
This work was accomplished by a group of investigators from the Centre for International Health, Education and Biosecurity (CIHEB Kenya), E. Koech, Rebecca.W, P. Awuor, E. Kirui, and collaborators from the Nairobi Metropolitan services, Carol. N.; the Center for Disease Control and Prevention (CDC Kenya), I. Mutisya; the University of Maryland, Baltimore, Habib.O, R, Taylor L. Special thanks to Nairobi County healthcare facilities and healthcare workers, the CIHEB Kenya strategic information team.
Author contributions
RON, PA, EK, EK, CN,RNW made substantial contributions to the conception, design, drafting and revising of the manuscript. HOR, TL, IM, made substantial contributions to data acquisition, analysis and interpretation. All authors read and approved the final manuscript. All authors are accountable for the accuracy and integrity of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) through the U.S. Centers for Disease Control and Prevention (CDC) under the terms of grant number 5NU2GGH001962/GH16-1701.
Ethics approval
Ethical approval for this study was obtained from Kenyatta National Teaching and referral Hospital-University of Nairobi Ethical Review Committee—KNH-UON ERC P (435/06/2018).
Informed consent
Not applicable.
The ethical review committee gave a waiver for consent.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.