
Abstract
Background:
We identified factors associated with complete hepatitis B vaccination of patients with HIV.
Methods:
Retrospective analysis of patients undergoing HIV clinic orientation from 2000 to 2010. Vaccine-eligible patients had negative hepatitis B serologies at baseline. Receipt of at least 3 doses was defined as complete vaccination.
Results:
Of 1242 patients, 519 (42%) were completely vaccinated. Complete vaccination was positively associated with missing ≤25% of the visits during the first year of care (adjusted odds ratio [aOR] = 2.35, 95% confidence interval [CI]: 1.79-3.09), being naive to care (aOR = 1.50, 95% CI: 1.13-1.99), and living at the clinic’s county (aOR = 1.33, 95% CI: 1.02-1.75). Complete vaccination was negatively associated with failure to remain in care >2 years (aOR = 0.18, 95% CI: 0.13-0.24), history of intravenous drug use (aOR = 0.48, 95% CI: 0.27-0.87), and baseline CD4 count <200 cells/mm3 (aOR = 0.69, 95% CI: 0.53-0.92).
Conclusion:
Poor retention in HIV care is strongly associated with suboptimal hepatitis B vaccination.
Introduction
HIV and hepatitis B virus (HBV) share routes of transmission and are both important public health issues with millions of patients infected worldwide. One-third of HIV-infected patients have evidence of prior exposure to HBV and on average 10% of these patients have chronic infection. 1 Coinfection has prognostic implications and has been associated with increased mortality when compared with HIV monoinfection, and mortality is highest with lower nadir CD4 counts. 2,3 After the development of highly active antiretroviral therapy (HAART) and its significant impact on AIDS-related mortality, liver disease has become a leading cause of death among HIV-HBV-coinfected persons. 4 Routine provision of hepatitis B vaccine is highly cost-effective among high-risk adults in the United States and should be routinely offered to these individuals. 5,6 The US National Committee for Quality Assurance jointly with the HIV/AIDS Work Group had recognized the importance of hepatitis B immunization and considered it a key measure of quality in HIV care. 7
Despite this recognition, the successful implementation of hepatitis B vaccine programs in HIV care centers has been a challenge. In settings such as primary care, sexually transmitted disease clinics, and other venues, the percentage of complete vaccination is also poor and a multitude of barriers and facilitators to effective hepatitis B vaccination have been identified in prior survey-based studies. Those barriers are patient specific such as (1) perceived medical and personal severity, (2) perceived practical issues such as time availability to be vaccinated, (3) trust in acquaintances previously vaccinated and trust in the physician, (4) disease risk perception, (5) financial constraints to pay for the vaccine, (6) fear of needles, and (7) overall familiarity with the vaccine. Barriers to effective vaccination are also health care provider-specific and include lack of clinical experience, younger age, lack of knowledge about specific risk factors of HBV transmission, and lack of subspecialty training. 8 –13
In the HIV primary care setting, the percentage of complete 3-dose vaccination among eligible patients broadly ranges from 16% to 63% during the HAART era. 14 –16 In these studies, hepatitis B vaccine efficacy was assessed in patients engaged in care for at least 6 months or longer. Therefore, little is known about the barriers to vaccination and the missed opportunities to administer the vaccine at all stages of the HIV linkage to care process. 17,18 Therefore, we aimed to assess the factors associated with hepatitis B vaccination in a population of patients undergoing linkage to and engagement in HIV care.
Methods
We conducted this retrospective analysis within the University of Alabama at Birmingham 1917 Clinic. This is an inner-city, Ryan White funder HIV primary care clinic. We obtained institutional review board approval prior to initiation of the study. We extracted data from the electronic medical records for all adult HIV-infected persons (N = 2554) who had an orientation visit scheduled between January 2000 and December 2010 (Figure 1). Sixty-eight patients were excluded due to “no show.” Of the remaining 2486 patients who had an orientation visit, we further excluded 1244 patients as they were vaccination ineligible (prior vaccination, prior virus clearance, or chronic HBV infection). Therefore, 1242 patients who were negative for both hepatitis B surface antigen (HBsAg) and hepatitis B surface antibody (HBsAb) were eligible to be included in the analysis. Vaccination in the clinic includes standard doses of recombinant HBV vaccine (Engerix B or Twinrix). For determining the number of doses each patient received, we extracted data until December 2011. Thereby, patients had the opportunity of being engaged in care for at least 1 year and undergo routine vaccination doses given at 0, 1, and 6 months according to clinic providers’ decisions.

Selection of study participants. Number of hepatitis B vaccine doses received until December 2011. HBsAg indicates hepatitis B surface antigen; HBsAg, hepatitis B surface antibody.
During orientation visit, patients newly diagnosed with HIV infection (or previously known to be HIV infected and transferring care to our clinic) responded to a comprehensive demographic and behavioral questionnaire. This was done prior to the first doctor’s appointment. At the orientation visit, patients received counseling, education, and psychosocial support. Clinic staff obtained baseline laboratory tests including hepatitis B serologic testing (HBsAg and HBsAb).
We reviewed electronic records for baseline demographic characteristics (age, sex, race, educational level, insurance status, and county of residency), risk factors for HIV acquisition (sexual orientation and history of intravenous drug use), substance abuse history (alcohol, cocaine, and intravenous drugs), detection of hepatitis C virus (HCV) antibody, baseline CD4 count, and plasma HIV RNA level. We retrieved from the electronic appointment log the frequency of missed visits in the first year after linkage to care and the total length of care for each patient.
Statistical Analysis
The outcome of interest in this study was vaccination status: patients who received at least 3 doses of HBV vaccine were considered completely “vaccinated,” while those who received 1, 2, or no doses were considered “undervaccinated.” Categorical independent variables were reported using frequencies and percentages. Continuous independent variables were reported using mean with standard deviation or median with quartiles. Associations between the dichotomized outcome variable and various independent variables were examined using univariate and multivariable logistic regression method producing crude odds ratios (ORs) and adjusted odds ratios (aORs), respectively, with corresponding 95% confidence intervals (CIs). In multivariable analysis, the following clinically important variables were included: sexual orientation (men who have sex with men [MSM]: yes/no), insurance status (private: yes/no), residency within the clinic county (yes/no), naive to care (yes/no), history of intravenous drug use (IVDU [yes/no]), duration of care (<2 years: yes/no), missed visits (≤25% versus >25%), baseline CD4 count (<200 versus ≥200 cells/mm3), baseline viral load (<400 versus ≥400 copies per mL), and HCV antibody status (positive versus negative). Multicollinearity of the independent variables was examined with variance inflation factor (VIF) by adjusting the linear combinations by the weight matrix used in the maximum likelihood algorithm 19 ; the VIF for all the factors was <1.2, thus indicating no multicollinearity. Hosmer-Lemeshow goodness-of-fit test chi-square P value for the multivariable model was .31, indicating model fit. Statistical significance was set at .05 (2-tailed test). Analysis was performed using SAS software version 9.2 (SAS Institute, Cary, North Carolina).
Results
Among the 1242 patients with negative HBsAg and HBsAb (eligible for hepatitis B vaccination upon orientation visit), 519 (42%) patients subsequently received ≥3 doses of HBV vaccine (vaccinated). Among the remaining 723 (58%) undervaccinated patients, 160 received 2 doses, 114 received 1 dose, and 449 patients received no doses at all (Figure 1).
Baseline characteristics of the patients with comparison between the vaccinated and undervaccinated groups are presented in Table 1. Overall mean age was 37.7 years, 71% were males, and 57% were African Americans. No significant differences were found between the 2 groups regarding age, gender, race, or education. Approximately half of the patients reported being MSM (48%) and 9% reported history of IVDU. Overall, median duration of care was 3.8 years, longer in the vaccinated group (4.8 years) compared to the “unvaccinated” group (1.5 years).
Sociodemographic and Clinical Characteristics of the HIV-Infected Patients Attending UAB 1917 Clinic during 2000-2010, by Hepatitis B Vaccination Status.a
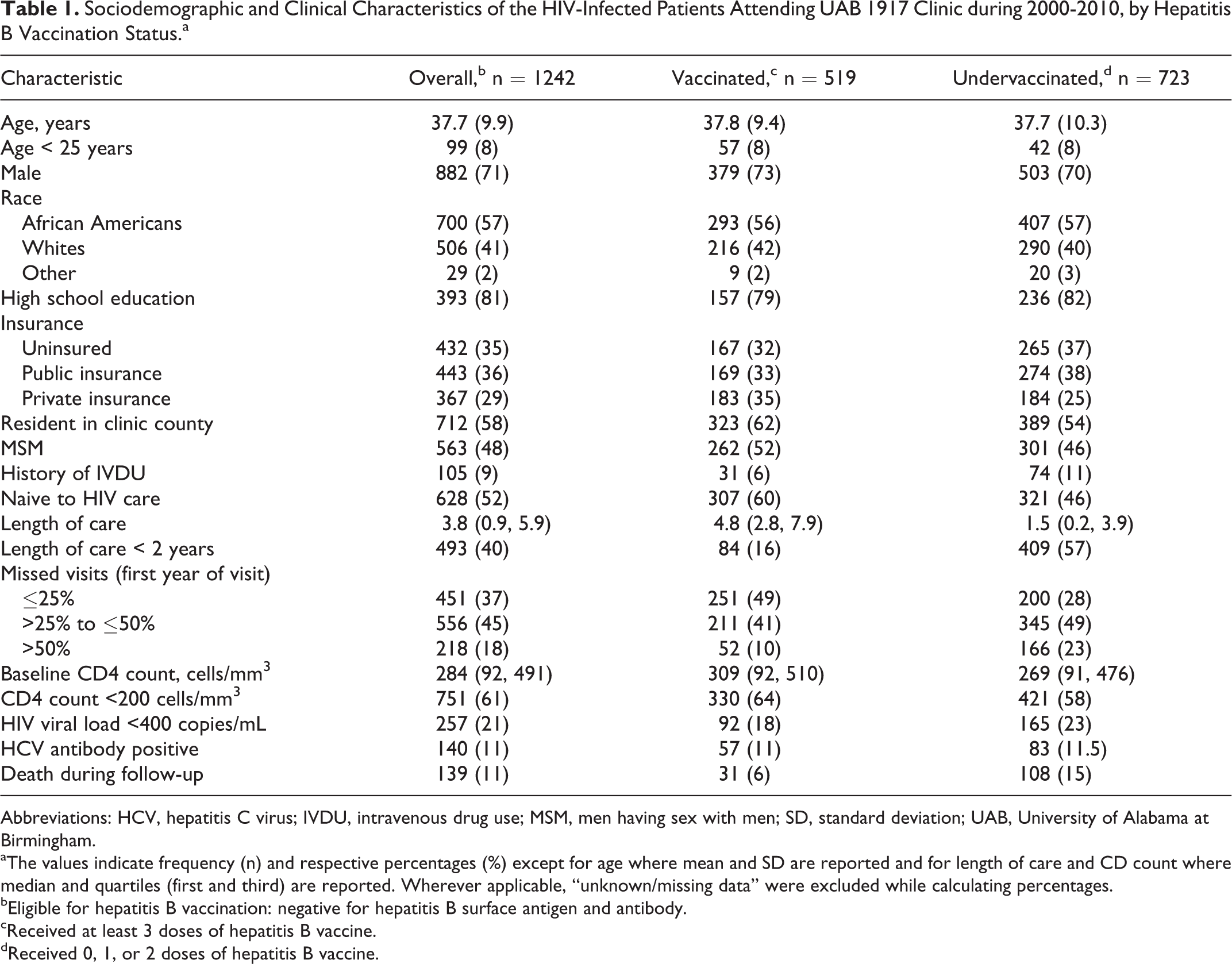
Abbreviations: HCV, hepatitis C virus; IVDU, intravenous drug use; MSM, men having sex with men; SD, standard deviation; UAB, University of Alabama at Birmingham.
aThe values indicate frequency (n) and respective percentages (%) except for age where mean and SD are reported and for length of care and CD count where median and quartiles (first and third) are reported. Wherever applicable, “unknown/missing data” were excluded while calculating percentages.
bEligible for hepatitis B vaccination: negative for hepatitis B surface antigen and antibody.
cReceived at least 3 doses of hepatitis B vaccine.
dReceived 0, 1, or 2 doses of hepatitis B vaccine.
In univariate analysis, multiple characteristics were found to be significantly associated with complete vaccination, except for HCV antibody status (Table 2). In multivariable analysis (Table 2), complete vaccination was positively associated with missing ≤25% of the visits during the first year of care (aOR = 2.35, 95% CI: 1.79-3.09), being naive to care (aOR = 1.50, 95% CI: 1.13-1.99), and being a resident of the clinic’s county area (aOR = 1.33, 95% CI: 1.02-1.75). Furthermore, complete vaccination was negatively associated with failure to remain in care >2 years (aOR = 0.18, 95% CI: 0.13-0.24), history of IVDU (aOR = 0.48, 95% CI: 0.27-0.87), and baseline CD4 count <200 cells/mm3 (aOR = 0.69, 95% CI: 0.53-0.92). The multivariable logistic regression model also included sexual orientation, insurance status, baseline viral load, and HCV antibody status. These variables were found not to be independently associated with the outcome of interest.
Examination of Associations of Various Characteristics with Complete Hepatitis B Vaccination in HIV-Infected Patients Attending UAB 1917 Clinic During 2000-2010.

Abbreviations: CI, confidence interval; HCV, hepatitis C virus; IVDU, intravenous drug use; MSM, men having sex with men; OR, odds ratio; UAB, University of Alabama at Birmingham; VL, viral load.
aHosmer-Lemeshow goodness-of-fit test chi-square P value = .31 (indicating model fit).
bStatistically significant at .05 level.
Discussion
Our findings demonstrated low rates of complete hepatitis B vaccination in a cohort of patients undergoing linkage to HIV care who are susceptible to HBV infection. Facilitators of HBV vaccination included missing less visits in the first year after linkage to care, being HIV treatment naive, and living in close proximity to the clinic. Important barriers to HBV vaccination included history of IVDU and a baseline CD4 count lower than 200 cells/mm3.
Hepatitis B vaccination has been recommended for HIV-infected patients since 1982. 20 More recently, the US National Committee for Quality Assurance had considered hepatitis B vaccination a key measure of quality in HIV care, in recognition of the public health importance of HBV, the prognostic implications of HIV/HBV coinfection, and the cost-effectiveness of hepatitis B vaccine. 7 However, previous studies have demonstrated poor adherence to vaccination guidelines. In studying the predictors of developing protective antibody responses after hepatitis B vaccination, Overton and colleagues identified complete vaccination rates of 63%. 14 Also during the HAART era, Tedaldi and collaborators 16 reported that although 81.9% of HIV-infected patients were screened for HBV, only 32% of vaccine-eligible individuals received at least 1 dose of vaccine. This rate was comparable to other reports in the pre-HAART era. 21 –23 In our study, 42% of the HBV-susceptible patients had completed the vaccination series and 64% received at least 1 dose.
Our findings suggest that barriers in engagement in care may play an important role in the receipt of complete vaccination series. This is exemplified by the median length of follow-up among vaccinated patients of 4.8 years, compared to only 1.5 years among undervaccinated ones. In Tedaldi’s study, vaccinated individuals had significantly higher number of clinic visits compared to unvaccinated ones (6.8 versus 5.8 average visits). 16 Among patients within 1 year after HIV care initiation, Fordham and colleagues also observed that only 22% of the 23 patients with documented nonimmunity to hepatitis B had begun hepatitis vaccination, despite having greater than 80% of these patients otherwise receiving Pneumocystis jirovecii prophylaxis, CD4 count assessment, and HIV therapy. 22 In our study, which accounted for all patients seen in orientation visit, almost one-fourth of them failed to engage in care for longer than 6 months.
Variables such as age, sex, race, education level, sexual orientation, insurance status, and HCV antibody status had similar distribution between vaccinated and undervaccinated groups. Considering the sociodemographic disparities found in HIV care retention and treatment, we have not expected these similarities between the 2 groups initially. 24,25 Possible explanations for the negative findings may rely on how the Ryan White care model makes access to care more uniform across demographic groups. 26 The absence of such disparities in achieving complete hepatitis B vaccination could hypothetically be explained by how vaccination may be a more feasible task to accomplish compared to long-term control of HIV viremia with HAART. 24
We have also observed the following: (1) patients were more likely to complete the vaccination series if they were residents at the clinic county area, suggesting that difficulties with transportation could be a potential barrier to vaccination. Messeri and collaborators, in assessing the impact of ancillary HIV services in New York City, concluded that provision of transportation was significantly associated with better maintenance of such services 27 ; (2) patients who were naive to care had better vaccination rates. It is possible that lack of continuity for patients transferring care from other clinics and difficulties in obtaining prior vaccination records may have contributed to these findings; and (3) history of IVDU was a factor that negatively impacted complete vaccination, independently of engagement in care, length of follow-up, and baseline CD4 counts. It is possible that measures toward addiction treatment and HIV medication compliance may have taken precedence to preventative measures such hepatitis B vaccination. Drug addiction and ongoing criminalization are well-recognized priorities to be addressed in the emerging strategic use of HIV treatment as prevention and engagement in care. 28
Patients who missed ≤25% of their scheduled visits in the first year were more likely to complete vaccination, while those who engaged in care for <2 years had 5 times lower odds of completing the vaccination schedule. Moreover, CD4 counts <200 cells/mm3 were an independent factor associated with undervaccination. Two years were chosen as reasonable time frame to count for those patients who would need immune recovery prior to vaccination, whenever CD4 counts were lower than 200 cells/mm3 at baseline. Due to concerns about poor vaccine responses, intentional delays in vaccination until CD4 count recovery are a common practice in our clinic. Considering the median follow-up of 4.8 years (quartile 1-quartile 3: 2.8-7.9) in the vaccinated group, patients undergoing longer follow-ups in care may have had more opportunities to receive preventative interventions than did patients who had shorter follow-ups. Therefore, the above-mentioned results could be explained by (1) the relatively long follow-up required for completeness of the schedule; (2) the dynamics involving provider compliance to vaccination guidelines and patient’s vaccine acceptance as suggested by others 8 –13 ; and (3) the likely impact of delaying vaccination until CD4 recovery.
Despite our reasonable sample size and the inclusion of patients undergoing the continuum of engagement in care in all phases, our study has several limitations. It is limited by its retrospective design and by the electronic data extraction that could not grasp in-depth data on key potential patient-specific and provider-specific barriers that affect retention in care and hepatitis B vaccination practices. Rather, our work is hypothesis generating, indicating that specific factors such as IVDU history, transportation difficulties, low CD4 counts, transfers of care between one HIV clinic to another, and overall engagement in care are potential starting points for further research aimed at improving hepatitis B vaccination practices for people living with HIV. Suboptimal engagement in care was a strong independent variable influencing vaccination rates in our study. Patient and provider-related barriers to engagement in care and vaccination delivery that were not covered in our statistical models deserve further studies.
Conclusion
Hepatitis B vaccination is of great importance to HIV-infected individuals based on sound clinical evidence. It is a measure of quality in HIV care and considered to be feasible of effective implementation. Nevertheless, hepatitis B vaccination programs face complex barriers that involve patients, providers, and the health system. This study demonstrates the powerful influence of engagement in HIV care on this key prevention measure. Living in proximity to the clinic and optimal attendance to visits in the first year after linkage to care were independently associated with complete vaccination series. Conversely, failure to remain in care longer than 2 years conferred decreased odds of complete vaccination. Moreover, patients with CD4 count <200 cells/mm3 had decreased odds of complete vaccination. The latter likely reflects a warranted provider bias (postponing vaccination until immune recovery) and highlights the dilemma between the need of better vaccination practices and the poor vaccine efficacy in this subgroup of patients. Likewise, IVDU was independently associated with incomplete vaccination. This is certainly a population at high risk of contracting HBV. In addition to the programmatic implications, our findings are helpful in identifying patient groups who may benefit from focused prevention efforts in the Ryan White funded model of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.