
Abstract
The US treatment guidelines recommend Pneumocystis jiroveci pneumonia (PCP) prophylaxis for all HIV-infected persons with a CD4 count <200 cells/mm3 (ie, eligible for PCP prophylaxis). However, some studies suggest PCP prophylaxis may be unnecessary in virally suppressed patients. Using national data of HIV-infected adults receiving medical care in the United States during 2009 to 2012, the authors assessed the weighted percentage of eligible patients who were prescribed PCP prophylaxis and the independent association between PCP prophylaxis prescription and viral suppression. Overall, 81% of eligible patients were prescribed PCP prophylaxis. Virally suppressed eligible patients were less likely to be prescribed PCP prophylaxis (prevalence ratio: 0.84; 95% confidence interval: 0.80-0.89). Although guidelines recommend PCP prophylaxis for all eligible patients, some HIV care providers might not prescribe PCP prophylaxis to virally suppressed patients. Additional data on the risk for PCP among virally suppressed patients are needed to clarify this controversy.
Keywords
Introduction
In the United States, the incidence of Pneumocystis jiroveci pneumonia (PCP) among HIV-infected persons has declined dramatically in the era of antiretroviral therapy (ART). A large US cohort study shows that PCP incidence has been below 1 case per 100 person-years since 2000. However, PCP remains the second most frequently diagnosed AIDS-defining opportunistic illness. 1 It is still a life-threatening disease even in developed countries with high-quality medical care. 2,3
The US treatment guidelines recommend PCP prophylaxis for all HIV-infected persons with a CD4 count <200 cells/mm3 or a history of oropharyngeal candidiasis. 4 Recent data suggest that PCP prophylaxis may be unnecessary for virally suppressed patients even if their CD4 counts are <200 cells/mm3. 5 –7 In this report, we present the national percentage of HIV-infected persons with a CD4 count <200 cells/mm3 who were prescribed PCP prophylaxis, and evaluate sociodemographic and clinical characteristics that may be associated with PCP prophylaxis prescription, in particular, durable viral suppression.
Methods
The Medical Monitoring Project (MMP) is a supplemental surveillance system designed to produce nationally representative estimates of behavioral and clinical characteristics of HIV-infected adults receiving medical care in the United States and Puerto Rico. 8 The MMP utilizes a 3-stage, complex sampling design in which the US states and territories are sampled, followed by facilities providing outpatient HIV medical care in those jurisdictions and then HIV-infected adults (aged 18 years and older) receiving care in those facilities. Data were collected by interviews and medical record abstractions. The surveillance period included the 12 months prior to interview. We combined data from the 2009 through 2012 cycles for this analysis. All sampled states and territories participated and the facility response rates were 76%-85% across all years. Approximately 50% (ranging from 47% to 53% across years) of eligible persons sampled from these facilities completed an interview and had their medical records abstracted. Data were weighted to account for unequal selection probabilities, and both facility and patient nonresponse.
The MMP is a public health surveillance activity and not subject to federal institutional review board (IRB) approval. 9 However, some jurisdictions obtained local IRB approvals. All participants provided informed consent to participate.
We analyzed data on 2143 patients who had at least 1 CD4 count <200 cells/mm3 during the first 6 months of the surveillance period to allow adequate opportunity for providers to prescribe PCP prophylaxis. We excluded 154 patients who were diagnosed with PCP during the surveillance period to avoid potential misclassification of PCP treatment as prophylaxis.
The CD4 count, HIV plasma viral load, and prescription information were abstracted from medical records. Durable viral suppression was defined as all viral load results <200 copies/mL during the surveillance period. Provider prescription of PCP prophylaxis was ascertained via medical record documentation of PCP “prophylaxis,” or documentation that the patient was either prescribed or continued on medical regimens typically provided for prophylaxis. Brief antibiotic prescriptions for 2 weeks or less were likely treatment of an acute infection and therefore were not considered as prophylaxis. Medications included atovaquone, aapsone, leucovorin, pentamidine, pyrimethamine, and trimethoprim–sulfamethoxazole. Medical record abstractors received training on how to identify and abstract PCP prophylaxis for quality assurance. We assessed the weighted percentage of HIV-infected patients with a CD4 count <200 cells/mm3 who were prescribed PCP prophylaxis. We also assessed the association between selected characteristics and PCP prophylaxis prescription using bivariate analysis (Rao-Scott χ2 test). Durable viral suppression was of particular interest, so we employed a multivariable logistic regression model to elucidate its independent association with PCP prophylaxis prescription. In this multivariable modeling process, we considered sociodemographic and clinical factors that were associated with both durable viral suppression and PCP prophylaxis prescription, including race, education, poverty, homelessness, length of HIV diagnosis, and hospitalization, as potential confounders. Only potential confounders that changed the association by at least 10%, as measured by the prevalence ratio, were retained in the final model. All analyses accounted for the complex sample design by using the survey procedures in SAS 9.3 (SAS Institute) and SUDAAN 10.0.1 (RTI International).
Results
The sociodemographic and clinical characteristics of patients who had at least 1 CD4 count <200 cells/mm3 are shown in Table 1. Among them, 64% had durable viral suppression, and 81% were prescribed PCP prophylaxis. Patients with a PCP prophylaxis prescription were not significantly different from patients without a prescription with regard to gender, age, education, homelessness, illicit drug use (excluding marijuana), or hospitalization (P > .05). Patients of white or Hispanic race/ethnicity, those above poverty level, or diagnosed with HIV for 5 years or more were less likely to be prescribed PCP prophylaxis (P < .05).
Sociodemographic and Clinical Characteristics of HIV-Infected Persons with a CD4 Count <200 cells/mm3 and Receiving Medical Care in the United States, Medical Monitoring Project, 2009 to 2012.
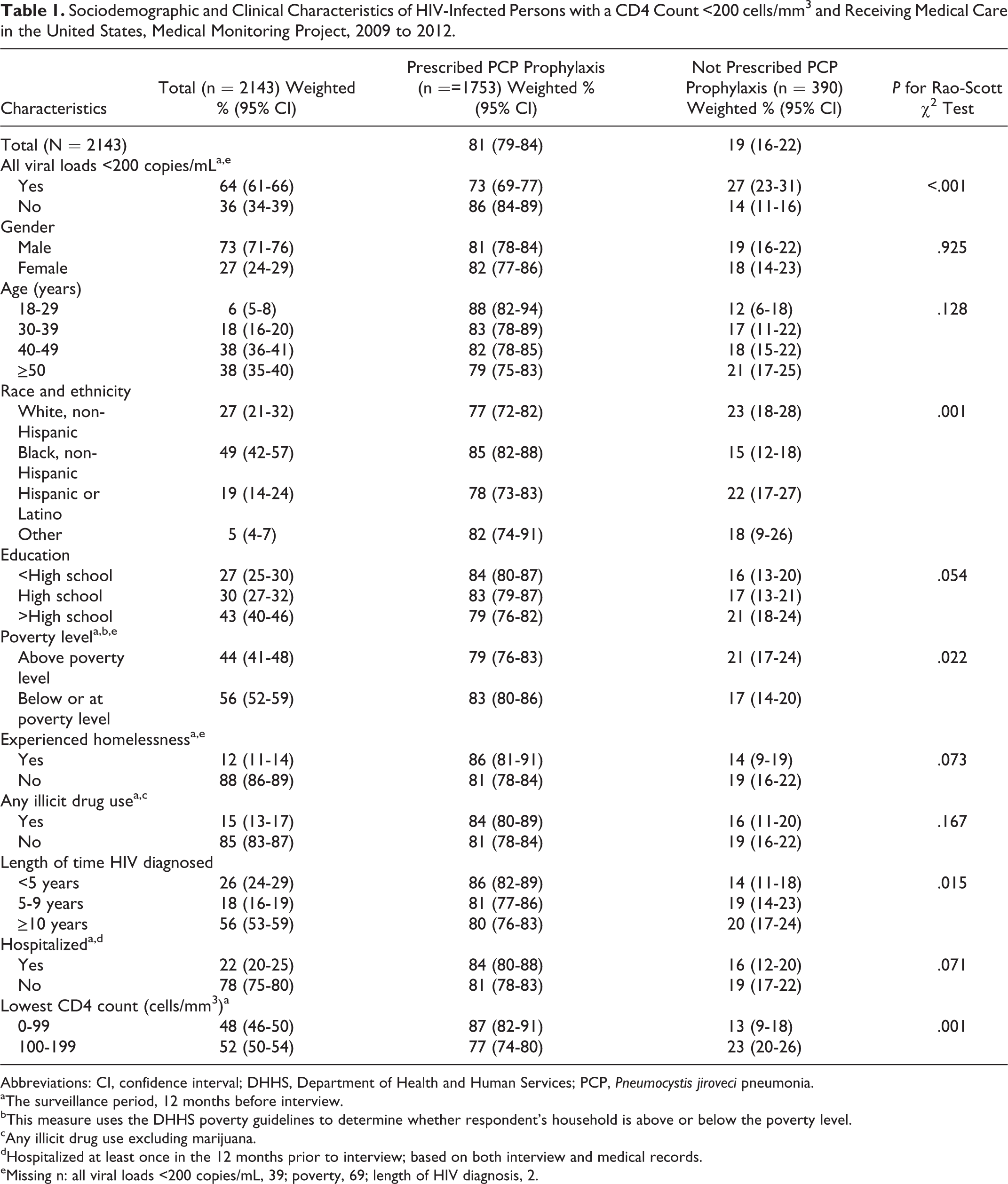
Abbreviations: CI, confidence interval; DHHS, Department of Health and Human Services; PCP, Pneumocystis jiroveci pneumonia.
aThe surveillance period, 12 months before interview.
bThis measure uses the DHHS poverty guidelines to determine whether respondent’s household is above or below the poverty level.
cAny illicit drug use excluding marijuana.
dHospitalized at least once in the 12 months prior to interview; based on both interview and medical records.
eMissing n: all viral loads <200 copies/mL, 39; poverty, 69; length of HIV diagnosis, 2.
During the logistic regression model selection process, the change in the association between durable viral suppression and PCP prophylaxis prescription by potential confounders ranged from 0% to 2%, so no confounders were included in the final model. Therefore, we used the unadjusted prevalence ratio to measure the independent association between durable viral suppression and PCP prophylaxis prescription. Virally suppressed patients were 16% less likely to be prescribed PCP prophylaxis (prevalence ratio: 0.84; 95% confidence interval: 0.80-0.89) compared with patients who were not virally suppressed.
Of note, among patients with a CD4 count <200 cells/mm3 who were not virally suppressed, 14% were not prescribed PCP prophylaxis (Table 1). In addition, 13% of the patients with a CD4 count <100 cells/mm3 were not prescribed PCP prophylaxis, regardless of viral loads (Table 1).
Discussion
Using nationally representative data of HIV-infected adults receiving medical care in the United States during 2009 to 2012, we estimated that 81% of patients who had at least 1 CD4 count <200 cells/mm3 were prescribed PCP prophylaxis. Our estimate indicates improved adherence to guidelines compared with the 2003 estimate of 76% produced using the Centers for Disease Control and Prevention’s Adult/Adolescent Spectrum of HIV Disease, which assessed trends in receipt of PCP prophylaxis among HIV-infected persons in the United States during 1994 to 2003. 10
We also found that among patients indicated for PCP prophylaxis, virally suppressed patients (viral loads <200 copies/mL) were less likely to be prescribed PCP prophylaxis compared with patients with HIV viral loads ≥200 copies/mL. Several recent studies have found a low incidence of PCP in HIV-infected persons with CD4 count <200 cells/mm3 if they are on ART and virally suppressed, and this may explain why providers in our analysis were less likely to prescribe PCP prophylaxis to virally suppressed patients. A large European cohort study and a case series found that PCP prophylaxis may be safely discontinued for patients who had plasma viral loads <400 to 500 copies/mL and had CD4 counts 100 to 200 cells/mm3, but not for patients who had CD4 counts <100 cells/mm3, regardless of viral suppression status. 6,11 One clinical trial and 2 case series revealed that PCP prophylaxis may be unnecessary for virally suppressed patients, regardless of CD4 count; however, they did not compare PCP incidence among virally suppressed patients with CD4 counts <100 cells/mm3 and patients with CD4 counts 100 to 200 cells/mm3. 7,12,13
Patients with advanced immunosuppression are more likely to be diagnosed with PCP. 14 In our analysis, we found that >10% of HIV-infected patients with CD4 counts <100 cells/mm3 were not prescribed PCP prophylaxis. Given the lack of evidence to support discontinuation of PCP prophylaxis for patients with CD4 counts <100 cells/mm3, prophylaxis is warranted in these individuals.
The major strengths of our analysis are that we generated national estimates on percentages of HIV-infected patients who were prescribed PCP prophylaxis by characteristics. There are at least 2 limitations to this analysis. First, while current treatment guidelines recommend PCP prophylaxis for all patients who have a CD4 count <200 cells/mm3, a history of oropharyngeal candidiasis, CD4 cell percentage of <14%, or a history of an AIDS-defining illness, we used CD4 count <200 cells/mm3 as our sole criterion for inclusion. Per treatment guidelines, CD4 count <200 cells/mm3 has the strongest evidence to support the use of PCP prophylaxis compared to the other criteria and should cover the majority of patients eligible for PCP prophylaxis. Second, given the cross-sectional nature of the analysis, we may have failed to capture PCP prophylaxis prescriptions provided after the end of the data collection period. To minimize this concern, we limited the analysis to participants who had at least 1 CD4 count <200 cells/mm3 during the first 6 months of the surveillance period to allow providers opportunities to prescribe prophylaxis if warranted.
In summary, 81% of HIV-infected persons with at least 1 CD4 count < 200 cells/mm3 were prescribed PCP prophylaxis. Compared with patients who had detectable HIV viral loads (≥200 copies/mL), virally suppressed patients were less likely to be prescribed PCP prophylaxis. While recent data suggest that PCP prophylaxis may be safely discontinued in virally suppressed patients with CD4 counts between 100 and 200 cells/mm3, the Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents has determined that evidence is insufficient to change the current recommendations. 4 Additional data on patient characteristics associated with PCP incidence in the ART era are needed to determine which individuals are at the highest risk for PCP and would benefit most from PCP prophylaxis.
Footnotes
Acknowledgments
The authors thank the MMP patients, facilities and Community and Provider Advisory Board members. They also thank the MMP staff (2009–2012): http://www.cdc.gov/hiv/pdf/research_mmp_studygroupmembers_2009.pdf; http://www.cdc.gov/hiv/pdf/research_mmp_studygroupmembers_2010.pdf; http://www.cdc.gov/hiv/pdf/research_mmp_studygroupmembers_2011.pdf; ![]() .
.
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the CDC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.