
Abstract
Lyme carditis is a rare manifestation of early disseminated Lyme disease with an incidence of 0.5% with left ventricular dysfunction and valvular involvement being exceedingly rare. Clinical manifestations typically occur 1 to 2 months after infection and include arrhythmias, conduction abnormalities, myopericarditis, and ventricular dysfunction. If left untreated, Lyme carditis can lead to acute heart failure and sudden cardiac death thus prompt diagnosis and treatment are essential in management. Here, we present a case of Lyme carditis with left ventricular dysfunction and valvular involvement occurring shortly after known tick exposure.
Introduction
Lyme disease is the most common vector-borne disease in North America with about 34,945 cases reported in 2019. 1 While Lyme disease most frequently affects the skin, joints, and nervous system, cardiac involvement is relatively rare. Earlier studies had reported the incidence of Lyme carditis to be from 4% to 10%, however, recent surveillance data from the Centers of Disease Control and Prevention (CDC) from 2008 to 2018 estimated it to be at 1%.1,2 Cardiac features of early disseminated Lyme disease usually occur about 1 to 2 months after infection. We report a case of Lyme myopericarditis presenting 1 week after known tick exposure complicated by a significant troponin elevation, left ventricular dysfunction, and new onset mitral valve regurgitation.
Case Presentation
A 22-year-old male with a past medical history of morbid obesity (body mass index [BMI]: 40.41) who presented to the emergency department with chest pain and lightheadedness for the past few days. The chest pain was in the substernal region and reported to be sharp in nature with occasional pressure-like episodes. It was reported to have started suddenly at rest, with a radiation to the left shoulder and associated worsening upon inspiration. He denied current illicit drug use, alcohol use, nausea, vomiting, dyspnea, or palpitations. Vitals signs on presentation were notable for tachycardia at 115 bpm, blood pressure of 103/63 mmHg, SpO2 of 98% on room air, and temperature of 36.8°C. On physical examination, he was noted to be diaphoretic and tachycardic. The presence of a single circular erythematous macular lesion was noted on the left flank. (Figure 1) Physical examination otherwise revealed no other abnormalities. Electrocardiogram (EKG) showed normal sinus rhythm with slight ST segment elevations in the inferolateral leads (Figure 2). Troponin T was elevated at 1.15 ng/mL (<0.01 ng/mL) and which then increased up to 1.38 ng/mL (<0.01 ng/mL) on subsequent testing 6 hours later (Table 1). Patient was started on intravenous heparin (weight-based infusion protocol) for suspicion of non-segment elevation myocardial infarction (STEMI) and was admitted to the coronary care unit (CCU). Echocardiogram was done which showed a left ventricular ejection fraction (LVEF) of 49% with mild diffuse hypokinesis, and moderate to severe mitral regurgitation (Figure 3). Lyme antibody tests were sent at the time of admission as the patient was a recreational hunter and recalled removing an engorged tick from his left flank 1 week prior. These tests resulted as a positive Lyme IgM antibody, while IgG antibody testing came back negative. The patient was subsequently started on IV Ceftriaxone 2g daily for treatment of Lyme carditis, and the heparin infusion was stopped. The diagnosis was confirmed with detection of Borrelia burgdorferi V1sE1/pepC10 antibodies by enzyme linked immunosorbent assay (ELISA) which was 2.71IV (>1.10IV =positive result). A coronary artery computed tomography (CT) angiography did not show significant stenosis or coronary anomalies, an Agatston score of 0, and a left ventricular chamber size which was discerned to be at the upper limit of normal. A follow up cardiac magnetic resonance imaging(MRI) showed nodular subendocardial delayed enhancement in the nonvascular distribution which may represent myocarditis (Figure 4). The patient showed marked improvement in symptoms after initiation of antibiotic therapy. The patient’s rash resolved with treatment and subsequent measurement of Troponin T level was seen to be 0.95 ng/mL (<0.01 ng/mL), which was lower than previous measurements. A repeat echocardiogram was performed, which showed an improvement of the previously visualized mitral regurgitation and normalization of LVEF. Patient was discharged to home on oral doxycycline 100 mg twice daily as per standard treatment guidelines for a total antimicrobial course of 3 weeks. On a 1-month follow-up, patient remains asymptomatic and is back to his previous baseline.
Laboratory Values With Reference Ranges.
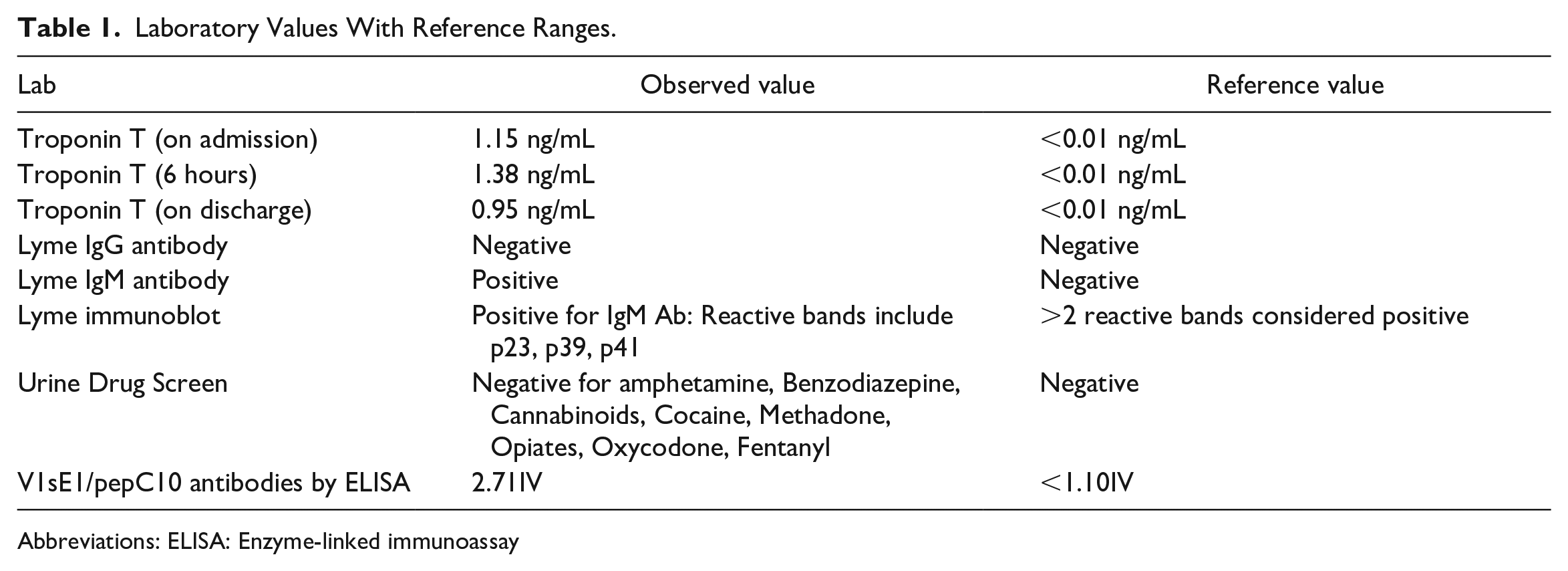
Abbreviations: ELISA: Enzyme-linked immunoassay

Left flank lesion.

Electrocardiogram from admission showing normal sinus rhythm with slight ST-segment elevations in the inferolateral leads.

Doppler echocardiogram from admission showing an apical view with moderate-severe Mitral regurgitation.

Cardiac Magnetic Resonance Imaging (A) Axial view with red arrow showing nodular subepicardial enhancement and (B) Sagittal view with red arrow showing subepicardial enhancement that does not involve the endocardium.
Discussion
Lyme carditis is a rare manifestation of Lyme disease with a reported incidence of about 1%. Patients usually present with lightheadedness, syncope, shortness of breath, palpitations, and/or chest pain. Sudden cardiac death associated with Lyme disease has also been reported. 3 Clinical manifestations of Lyme carditis include arrhythmias, conduction abnormalities, myopericarditis, ventricular dysfunction, and acute heart failure. 4 The diagnosis of Lyme carditis is established by presence of potential tick exposure in endemic areas, positive Lyme serologic testing, and previously mentioned clinical manifestations. Atrioventricular (AV) conduction abnormalities including AV blocks of varying severity are the most common manifestation as well as the most dangerous. Left ventricular dysfunction, as seen in our patient, has been reported to have an incidence of 0.5%. 4 Lyme carditis is usually mild and self-limiting and rarely leads to cardiomyopathy. 5 Cardiac manifestations in Lyme disease typically occur 1 to 2 months after the onset of infection and are due to local inflammation caused by myocardial invasion by B. burgdorferi. 5 In our patient, however, Lyme carditis was seen a little over 1 week after known tick exposure. Furthermore, the Lyme IgM Immunoblot was positive and IgG was negative indicating early infection. To date, about 7 cases of valvular involvement in Lyme carditis have been reported making this phenomenon exceedingly rare. 6 Proposed pathophysiology includes local invasion of pathogen and macrophage causing leaflet edema. Mitral valve endocarditis due to Borrelia spp. has also been reported and is gaining increasing recognition according to a recent review by Nikolić et al. 7
The prognosis of Lyme carditis is good among patients who are treated, as seen in our patient who had a complete reversal of valvular dysfunction and decrement in LVEF with treatment. Fatalities have been reported but are rare. A case series published by the CDC reported 3 individual deaths that were attributed to Lyme disease by postmortem examination indicating that lack of treatment can lead to fatalities. 3 Given the propensity of life-threatening complications such as complete AV block and sudden cardiac death, early diagnosis and treatment are essential. If there is a high suspicion for Lyme carditis, empiric treatment with antibiotics should be started while the initial evaluation is pending.
Conclusion
Lyme carditis is a rare manifestation of disseminated Lyme disease; left ventricular dysfunction and valvular involvement are rarer still. Lyme disease should be considered as a part of workup for acute onset cardiomyopathies irrespective of timing of tick exposure. Early diagnosis and treatment are essential for preventing cardiac complications and death.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because there is no patient identifying information included in this manuscript.