
Abstract
This case report details a rare and life-threatening complication of heat stroke: necrotizing pancreatitis. While heat stroke is known to affect multiple organ systems, its association with acute pancreatic necrosis is extremely uncommon and poses significant diagnostic and management challenges. In this report, we examine the patient’s clinical progression and discuss the possible underlying pathophysiological mechanisms linking heat stroke to necrotizing pancreatitis. We also highlight the multidisciplinary medical interventions undertaken, emphasizing the importance of early recognition and aggressive management in improving outcomes for patients with such severe complications.
Introduction
Heat-related illnesses encompass a spectrum of disorders resulting from elevated body temperature, primarily caused by prolonged heat exposure. Various factors influence clinical presentation, including individual susceptibility, the type of heat exposure, and sociocultural determinants. 1 Heat stroke, the most severe form, is classified into 2 types: classic and exertional. Classic heat stroke occurs in the absence of strenuous activity and is typically seen in individuals with preexisting conditions, often triggered by high ambient temperatures (>40.5 °C) and/or humidity. 1 Exertional heat stroke, on the other hand, results from the body’s inability to dissipate heat effectively due to either external heat exposure or increased metabolic heat production from intense physical exertion. 1
The combination of hyperthermia and dehydration in heat stroke can lead to circulatory failure and subsequent multiorgan dysfunction. 1 Beyond the immediate complications, heat-related illnesses have also been associated with the exacerbation of preexisting conditions. Studies have reported increased incidence of ischemic heart disease, cardiac dysrhythmias, ischemic stroke, asthma, chronic obstructive pulmonary disease, respiratory infections, hyperglycemia, kidney failure, and neuropsychiatric disorders, including psychosis, anxiety, depression, suicides, and homicides. Additionally, adverse birth outcomes, such as preterm delivery and small-for-gestational-age infants, have been linked to heat exposure. 1
We present the case of a 37-year-old female who suffered heat stroke, with recovery complicated by severe necrotizing pancreatitis. Her condition further deteriorated due to the development of a pancreatic pseudocyst, abscess, and fistula formation, ultimately requiring necrosectomy.
Case Presentation
A 37-year-old female with a history of hypothyroidism and schizophrenia on a long-acting injectable antipsychotic presented for altered mental status after spending the day working outside in temperature peaking at 35.5 °C. A seizure was witnessed by the family. Upon arrival at the Emergency Department, her Glasgow Coma Scale was 8 (E3, V1, M4). She was febrile at 42.2 °C, hypotensive with a mean arterial pressure of 54 mmHg, tachycardic with a heart rate of 140 bpm, and tachypneic with a respiratory rate of 40 breaths/minute. Immediate cooling measures including cool mist, ice packs, and an orogastric tube with cold water were initiated, leading to improved temperature control. Initial laboratory findings revealed a blood urea nitrogen of 20 mg/dL, creatinine of 1.88 mg/dL, lipase of 353 U/L, lactic acid of 5.1 mmol/L, creatine kinase of 626 U/L, troponin of 172 ng/L, and ammonia of 79 µmol/L. A venous blood gas showed a pH of 7.2, pCO2 of 37 mmHg, pO2 of 49 mmHg, and HCO₃− of 14 mmol/L (Table 1). A computed tomography (CT) scan of the abdomen and pelvis with contrast revealed calcified gallstones, fatty liver infiltration, and moderate peripancreatic fat stranding, suggesting acute pancreatitis (Figure 1).
Labs for HD 1, HD 4, HD 12, and HD 55 With Normal Ranges and Units of Measurement.

Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; HD, hospital day; mg/dL, milligrams/deciliter; mmHg, millimeter of mercury; mmol/L, millimoles/liter; ng/L, nanograms/liter; µmol/L, micromoles/liter; U/L, units/liter.
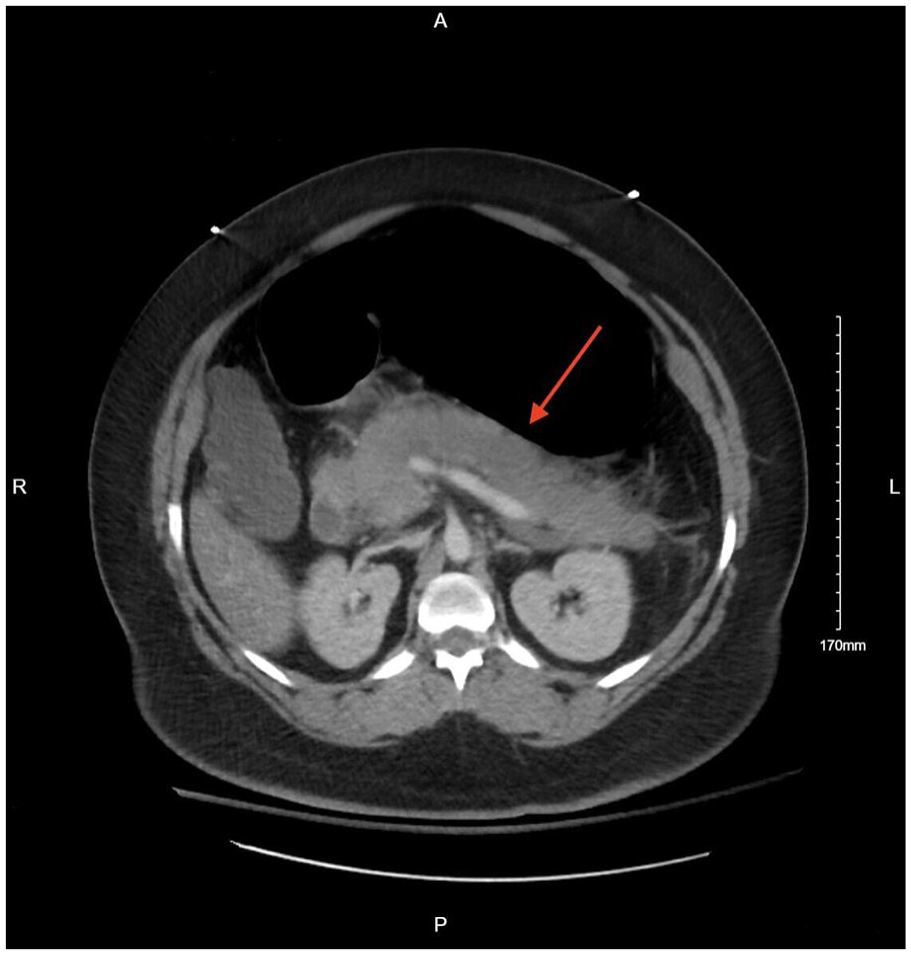
Axial computed tomography of the chest, abdomen, and pelvis w/ contrast showing moderate diffuse peripancreatic soft tissue fat stranding suggesting acute pancreatitis (red arrow).
On day 4, a triglyceride level of 1293 mg/dL was detected, alongside an elevated lipase of 1270 U/L (Table 1). An ultrasound of the abdomen revealed choledocholithiasis, nonspecific gallbladder wall thickening, and a dilated common bile duct. Due to her hemodynamic instability and ongoing need for vasopressor support, magnetic resonance cholangiopancreatography was deferred. A repeat CT scan of the abdomen and pelvis showed progressive peripancreatic fat stranding with fluid extending into the paracolic gutters and pelvis, persistent gallstones, and no biliary duct dilation. By day 22, the patient developed a fever and increased vasopressor requirements. A follow-up CT scan confirmed necrotizing pancreatitis, characterized by large areas of nonenhancing pancreatic tissue and multiloculated fluid collections extending into the retroperitoneum, suggesting an acute necrotic collection (Figure 2). A subsequent CT scan revealed large pancreatic pseudocysts measuring ~21 cm in the left upper quadrant and a loculated fluid collection abutting the left lateral abdominal wall, concerning for an evolving abscess. Due to poor oral tolerance, likely secondary to gastric compression from the pseudocyst, a percutaneous endoscopic gastrostomy tube was placed.

Computed tomography of the chest, abdomen, and pelvis w/ contrast showing findings of necrotizing pancreatitis with multiloculated collections seen surrounding the pancreas (red arrow).
The patient was discharged on day 55 given improvement in labs and adequate feeding site but was readmitted the following day after pulling out her G-tube and presenting with fever and tachycardia (Table 1). CT imaging showed progression of peripancreatic fluid collections, now measuring up to 31 cm, with gas bubbles present within the collections, consistent with infected pseudocysts, and small blind-ending tracts extending anteriorly raised suspicion for an evolving fistula (Figure 3). On day 63, a cystenterostomy with partial pseudocyst drainage was performed, along with reinsertion of the G-tube. The patient later developed gastric outlet obstruction due to pseudocyst compression and failed a gastric emptying study, necessitating an endoscopic necrosectomy via esophagogastroduodenoscopy.

Computed tomography of the chest, abdomen, and pelvis w/ contrast showing necrotizing pancreatitis with multiple surrounding infected pseudocysts that are increasing in size (right arrow) and small blind-ending tracks extending anteriorly from the peripancreatic fluid collection without definite fistulous communication (left arrow).
The following day, a rapid response was called due to increased work of breathing and hypotension, with a mean arterial pressure between 40 and 50 mmHg. A CT angiogram of the chest, abdomen, and pelvis revealed active hemorrhage into the peripancreatic fluid collection. Interventional radiology (IR) identified a splenic artery pseudoaneurysm with brisk extravasation and a splenic arteriovenous fistula, likely sequelae of severe pancreatitis. Splenic artery embolization was performed on day 77. On day 103, the patient was readmitted for hematemesis and diagnosed with multiple intra-abdominal abscesses secondary to necrotizing pancreatitis. A pigtail drainage catheter was placed in the left lower quadrant on day 115. Fluid cultures grew Enterobacter cloacae ssp cloacae, Candida albicans, and Candida glabrata. On day 126, video-assisted retroperitoneal debridement was performed. Further complications included fistula formation, confirmed via CT imaging, showing communication between the pancreatic bed and the left retroperitoneal collection. Additional pigtail drainage catheters were placed in the left upper quadrant for splenic abscess drainage, with cultures yielding Klebsiella pneumoniae, E. cloacae ssp, and vancomycin-resistant Enterococcus faecalis. The patient was transferred to a higher-level care facility for definitive necrosectomy.
At the outside facility, the patient underwent a robotic cholecystectomy on day 148 for source control due to previous cultures growing C. albicans and C. glabrata. On day 154, AXIOS stent removal and necrosectomy were performed by gastroenterology, complicated by a duodenal leak, which was assessed by an IR sinogram but required no new intervention. A repeat CT showed no new collections, allowing for the removal of left upper quadrant and left lower quadrant drains on day 162 which was redemonstrated on a CT obtained at the local facility (Figure 4).

Computed tomography of the chest, abdomen, and pelvis w/ contrast showing residual mild fat stranding with no significant abnormal sizeable fluid collection (red arrow).
The patient’s hospital course was additionally complicated by a non-ST elevation myocardial infarction, cardiogenic shock with an ejection fraction of 30%, acute kidney injury requiring continuous renal replacement therapy and hemodialysis, shock liver, disseminated intravascular coagulation, left lower extremity nonocclusive deep vein thrombosis, and ventilator-associated pneumonia with septic shock requiring tracheostomy. Ultimately, the patient was discharged to an acute rehabilitation facility, where she received physical therapy, occupational therapy, and speech-language pathology to facilitate the transition from tube feeding to oral intake.
Discussion
This report presents a rare case of necrotizing pancreatitis in the setting of heat stroke. The complications of necrotizing pancreatitis in this patient included pseudocyst formation, fistula development, intra-abdominal abscesses, splenic artery pseudoaneurysm, and gastric outlet obstruction. This case is particularly noteworthy as pancreatitis is an uncommon complication of heat stroke, and the severity of the pancreatic disease in this patient necessitated multiple interventions, including gastric tube placement, cystenterostomy with pseudocyst drainage, endoscopic necrosectomy, splenic artery embolization, video-assisted retroperitoneal debridement, multiple drain placements, and cholecystectomy for source control.
Acute pancreatitis is a common condition resulting from an acute injury to the pancreas. 2 Gallstones and alcohol use are the 2 most common causes of acute pancreatitis, accounting for 65% to 70% of cases. Less common causes include autoimmune disorders, hypertriglyceridemia, post-endoscopic retrograde cholangiopancreatography, pancreatic duct injuries, medications, infections, anatomical abnormalities, and systemic diseases such as systemic lupus erythematosus. 2 The pathophysiology of acute pancreatitis involves inhibition of secretion, intracellular activation of proteases, and the release of inflammatory mediators. 3 Stressful physiological events have been shown to predispose individuals to acute pancreatitis episodes, triggering the formation of heat shock proteins (HSPs), which play a protective role by reducing inflammatory marker production, enhancing pancreatic recovery, and inducing cellular defense mechanisms. 4 Although acute pancreatitis accounts for ~275 000 hospital admissions annually, the majority of cases are mild, requiring only a few days of inpatient care, with an overall mortality rate of 2%. 2 This context underscores the extraordinary severity of pancreatitis in this patient, as she experienced multiple complications requiring prolonged hospitalization and extensive interventions.
Although the patient’s inciting injury was clearly secondary to heat stroke, multiple additional etiologies of pancreatitis were identified throughout her hospital course, complicating the treatment approach. While hyperthermia may induce protective factors through the stimulation of HSPs, heat stroke as an etiology is a rarely reported cause of acute pancreatitis. 5 The exact pathophysiology of the association between heat stroke and acute pancreatitis is not well understood, though it is hypothesized to resemble the mechanisms observed in pancreatitis secondary to septic shock. Severe hypotension and tissue hypoperfusion are key contributors to pancreatic ischemia, with proposed mechanisms including cellular apoptosis, increased endothelial nitric oxide release, platelet activation, and ischemia-reperfusion injury. 6 Studies have demonstrated that transient pancreatic ischemia lasting as little as 40 minutes can result in significant histological damage, including peripheral necrosis of pancreatic lobules. 6
Several other factors likely contributed to the severity of the patient’s pancreatic injury. Her history of hypothyroidism may have predisposed her to impaired thermoregulation, increasing susceptibility to heat-related illness. Furthermore, she was receiving monthly intramuscular injections of paliperidone for schizophrenia, a medication that has been linked to rare cases of drug-induced pancreatitis. 3 Initial imaging on the day of admission revealed calcified gallstones, a known cause of pancreatitis, though gallstone pancreatitis was deemed unlikely in this case. However, subsequent workup demonstrated worsening lipase elevation and ultrasound findings concerning for choledocholithiasis. While choledocholithiasis may not have been the primary cause of pancreatitis given the acute presentation of her lipase elevation, the systemic inflammatory response triggered by heat stroke could have exacerbated underlying biliary disease, contributing to the progression of pancreatic injury. 7
The patient also developed hypertriglyceridemia exceeding 1000 mg/dL, likely secondary to propofol administration, a known risk factor for pancreatitis. 2 Consequently, she was transitioned to midazolam, and an insulin drip was initiated to mitigate the combined effects of hypertriglyceridemia and heat stroke-related pancreatic injury. Another significant factor was the development of cardiogenic shock during her hospital course, with an echocardiogram revealing an ejection fraction of 30%. Studies have indicated that cardiogenic shock can contribute to pancreatic ischemia, further compounding the severity of her condition. 8 Collectively, these factors highlight the multifaceted nature of her disease progression and underscore the complexity of managing pancreatitis in the setting of multiple overlapping etiologies.
Raising awareness about heat stroke-induced pancreatitis is crucial for several reasons. First, as global temperatures continue to rise due to climate change, the incidence of heat-related illnesses is expected to increase, potentially leading to more cases of rare complications like pancreatitis. Prompt recognition of this association can lead to earlier diagnosis and timely interventions, potentially preventing the development of severe complications such as necrosis or multiorgan failure. Additionally, because heat stroke is often treated supportively, awareness among healthcare providers about its potential to trigger pancreatic injury could prompt earlier imaging, laboratory testing, and consideration of alternate causes for abdominal symptoms. Educating clinicians, especially those in emergency and critical care settings, on this rare but severe manifestation may improve diagnostic accuracy and outcomes. Furthermore, a better understanding of the pathophysiological mechanisms linking hyperthermia to pancreatic injury could drive research into targeted therapies, preventive strategies, and more effective clinical protocols. Overall, greater awareness and knowledge dissemination regarding this uncommon presentation can ultimately enhance patient safety and reduce morbidity and mortality associated with heat stroke-induced pancreatitis.
Conclusion
The pathogenesis of this patient’s necrotizing pancreatitis and associated complications was multifactorial, with heat stroke being the primary inciting event. Further research is needed to elucidate the precise mechanisms by which heat stroke precipitates acute pancreatitis and to determine the relative contributions of other predisposing factors. Given the potential for severe morbidity associated with pancreatic injury, a deeper understanding of this pathophysiology could inform treatment strategies and improve outcomes for patients with heat stroke-induced pancreatitis.
Footnotes
Acknowledgements
None.
Author Contributions
Hobart Lai, Edvard Davtyan, Anna Vajda, Jiayan Tan, Anna Mikami, and Zahur-Saleh Subedar participated in the writing and revisions of the manuscript. Conceptualization of this novel case is attributed to Hobart Lai, who served as the supervising faculty. Review of literature referenced, manuscript preparation, and critical intellectual revisions of content were completed by all authors. All authors reviewed, edited, and agreed upon the final version of the manuscript prior to submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This report study received approval by Kern Medical Center’s (KMC) Institutional Review Board (#24208). Documented patient approval for the use of images and the description of this case was obtained prior to publication.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.